American Ballet Theater doesn’t typically align its seasonal galas with a company member’s farewell, but in the case of Misty Copeland, whose trailblazing career has irrevocably changed the 85-year-old institution, an exception was made. A…
From 12-18 October 2025, the United Nations Office for Disarmament Affairs (UNODA) and the United Nations Department of Safety and Security (UNDSS) organized the fifth training course on ‘Safe and Secure Approaches in Field Environments’…
Helicobacter pylori (H. pylori) infections correlate with chronic active gastritis, peptic ulcer development, gastric mucosa-associated lymphoid tissue lymphoma, gastric cancer, and other digestive diseases, as well as extradigestive disorders such as cardiovascular, hematologic, and autoimmune diseases [-]. A recent meta-analysis of data from 73 countries revealed a global H. pylori infection rate of 44.3%, higher in low- and middle-income countries (50.8%) than in high-income countries (34.7%), imposing significant economic burdens []. These findings underscore H. pylori’s pervasive harm, heightening global public health concerns for its eradication []. Standard triple and quadruple therapy combining proton pump inhibitors or bismuth with 2 antibiotics is established for H. pylori eradication [,]. However, despite widespread antibiotic use, eradication rates remain suboptimal, often due to antibiotic resistance and poor patient compliance [].
Poor patient compliance significantly impacts H. pylori eradication treatment as it increases the risk of treatment failure and contributes to the development of secondary antibiotic resistance due to inadequate drug dosages [,]. According to research involving a large patient cohort, those with good compliance, defined as completing over 80% of prescribed medication regimens, achieved eradication rates of 85% to 94%, whereas those with poor compliance achieved rates of only 39% to 53% []. Various factors influence patient compliance, including the complexity of the eradication regimen, treatment duration, adverse reactions, physician motivation, and patient awareness [,]. Currently, the prevailing eradication regimen typically lasts 7 to 14 days and involves administering 3 to 4 drugs before or after meals []. However, the regimen’s complexity and extended duration pose challenges for both physicians and patients, prompting widespread discussion among gastroenterologists on how to effectively address this issue.
Objectives
To combat poor patient compliance in H. pylori eradication treatment, various strategies have been implemented to enhance medication adherence, including health education, information communication, medication guidance, feedback on adverse drug reactions, and regular question-and-answer sessions. The emergence of new media technologies—such as telephone-supported follow-ups, SMS text messaging, and social media– or app-based modules—has opened up new avenues for patient education and supervision. In this review, we define new media–based education (NME) as a form of patient education and adherence support distinct from traditional oral or paper-based approaches. It is digitally delivered and interactive, implemented through mobile or networked platforms (eg, telephone-supported follow-ups, SMS text messaging, and various social media– or software-based applications). NME typically incorporates targeted communication and reminders, multimedia educational content, and bidirectional messaging in alignment with established digital health (mobile health) frameworks [-]. Despite its widespread use, the precise impact of NME on H. pylori eradication remains uncertain. Three meta-analyses published in 2022 suggested that enhanced educational interventions may improve eradication rates and patient compliance without increased adverse events [-]. However, these reviews were limited by relatively small sample sizes and the absence of comprehensive subgroup analyses, leaving uncertainties regarding the consistency and generalizability of their findings. To address these gaps, we conducted an updated and more comprehensive meta-analysis to evaluate the efficacy of NME in improving H. pylori treatment outcomes.
Methods
Registration and Implementing Guidance
This study adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and was registered on PROSPERO under registration number CRD42024517954.
Search Strategy
We systematically searched PubMed, Embase, Web of Science, and the Cochrane Library from inception to February 2025. The review protocol was registered in PROSPERO in February 2024, and an updated search was conducted in February 2025 to ensure the inclusion of the most recent studies. Eligible study designs included randomized controlled trials (RCTs) and retrospective cohort studies evaluating NME interventions for patients with H. pylori infection. The search strategy combined MeSH (Medical Subject Headings) terms and free-text keywords such as “Helicobacter pylori,” “patient education,” “educational technology,” “mobile phone applications,” “smartphone,” “short message service (SMS),” “text messaging,” “WeChat,” “tele-education,” “internet,” and “telemedicine” using Boolean operators (AND and OR) to maximize sensitivity. An example search string for PubMed was as follows: (“Helicobacter pylori” OR “H. pylori”) AND (“patient education” OR “health education” OR “educational technology” OR “mobile phone” OR “cell phone” OR “smartphone” OR “text message*” OR “short message service” OR “SMS” OR “WeChat” OR “tele-education” OR “telemedicine” OR “digital health”) AND (“randomized controlled trial” OR “controlled clinical trial” OR “cohort study”). The reference lists of the included studies and relevant reviews were also screened to identify additional eligible articles. The complete and detailed search strategies for each database are provided in in accordance with the PRISMA 2020 reporting guidelines.
Study Selection
Two investigators independently screened the initially retrieved bibliography using a 2-stage screening process. Any discrepancies were resolved through discussion or consultation with a third investigator. In the first phase, duplicates were automatically removed, followed by manual removal of any remaining duplicates. Studies were excluded based on inclusion and exclusion criteria by reviewing titles, abstracts, and full texts.
The following inclusion criteria were used in this study: (1) participants were individuals with H. pylori infection confirmed via rapid urease test, urea breath test, stool antigen test, culture, or histology with at least one positive result and who had not previously received eradication therapy; (2) the intervention was implementation of NME methods, such as telephone-based follow-up, SMS text messaging, or mobile apps, in combination with a standard eradication regimen (triple or quadruple therapy); (3) the comparator was a standard eradication regimen with conventional oral or written instructions; (4) the primary outcomes included H. pylori eradication rate and patient compliance, and the secondary outcomes included adverse events and patient satisfaction; and (5) the study design was RCTs and retrospective cohort studies. Retrospective studies were included due to limited available evidence and their comparable design and intervention quality to those of RCTs. The exclusion criteria were as follows: (1) publications in the form of comments, letters, protocols, conference abstracts, or reviews; (2) studies with insufficient data or duplicate reports; and (3) ongoing studies without available results.
Data Extraction
Two independent investigators extracted data from eligible studies using a predefined data collection form. Discrepancies were resolved through consensus. Extracted data included study characteristics, patient demographics, outcomes, and details of risk-of-bias assessment.
Risk-of-Bias Assessment
The methodological quality of the included studies was independently assessed by 2 reviewers, with disagreements resolved by a third reviewer. For RCTs, we applied the revised Cochrane risk-of-bias tool for randomized trials (RoB 2), which evaluates 5 domains: bias arising from the randomization process, bias due to deviations from the intended intervention, bias due to missing outcome data, bias in measurement of the outcome, and bias in the selection of the reported results. Each domain was judged as “low risk,” “some concerns,” or “high risk,” and an overall risk-of-bias judgment was assigned accordingly. In total, 11 RCTs were evaluated using the RoB 2 tool.
For nonrandomized cohort studies, we used the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool, which assesses 7 domains: bias due to confounding, bias in the selection of participants, bias in classification of interventions, bias due to deviations from the intended intervention, bias due to missing data, bias in measurement of outcomes, and bias in the selection of the reported results. The overall risk of bias for cohort studies was categorized as low, moderate, serious, or critical. The 2 retrospective cohort studies included in this review were assessed using the ROBINS-I tool.
Statistical Analysis
We calculated risk ratios (RRs) and 95% CIs to evaluate associations between groups and outcomes. The primary outcomes were the pooled RRs of H. pylori eradication rate and patient compliance, whereas the secondary outcomes were pooled RRs of adverse events and patient satisfaction. We selected intention-to-treat (ITT) analysis as the primary approach because of its stronger scientific rationale, greater clinical applicability, and its ability to reflect real-world practice. Although some of the included studies (10/13, 77%) reported per-protocol (PP) data, only 69% (9/13) provided PP results for eradication, and just 31% (4/13) provided PP results for compliance. Given this limited number, it was not feasible to conduct meaningful subgroup analyses based on PP data, and conducting a pooled PP analysis under such circumstances would have resulted in too small a sample size, thereby reducing statistical robustness and potentially introducing bias. Consequently, we relied exclusively on ITT analysis to ensure the consistency, validity, and reliability of the findings while also minimizing the risk of selective reporting.
Heterogeneity was assessed using the I2 statistic, with thresholds of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. In line with current recommendations, we used a random-effects model for all meta-analyses to account for potential between-study heterogeneity and provide more conservative estimates.
Prespecified subgroup analyses were conducted to explore potential sources of heterogeneity. Subgroups were stratified according to intervention type (WeChat, telephone, telephone combined with other methods, and SMS text messaging), treatment regimen (triple vs quadruple therapy), age group (≤60 vs >60 years), country socioeconomic status (high income vs low and middle income), whether baseline outpatient education was provided, and whether WeChat group functionality was used.
Sensitivity analyses were conducted by sequentially excluding each study to assess its influence on the overall effect size.
Compliance definitions varied among studies, with 100% compliance defined as taking the prescribed dose. Publication bias was assessed using funnel plots, the Egger linear regression test, and the Begg rank correlation test. All primary meta-analyses were conducted using RevMan (version 5.4.1; The Cochrane Collaboration). Additional statistical analyses, including sensitivity analyses and publication bias assessments, were conducted using the Comprehensive Meta-Analysis software (version 3.0; Biostat, Inc).
Results
Study Flow
Our initial search identified 476 potentially relevant clinical trials. After thorough review and screening, of the 476 studies, 11 (2.3%) RCTs and 2 (0.4%) retrospective cohort studies [-] met the inclusion criteria and were included in the meta-analysis. The study selection process is detailed in .
Figure 1. Flowchart of study selection.
Risk of Bias
Using the RoB 2 tool [], most of the 11 (85%) included RCTs were judged to be at low risk of bias, with some concerns mainly related to the randomization process and missing outcome data; no trial was rated as high risk (Figure S1A in ). The 2 retrospective cohort studies were assessed using the ROBINS-I tool [], which indicated a moderate risk of bias for one study [] and a serious risk for another [], largely due to confounding and limitations in participant selection and outcome measurement (Figure S1B in ).
Study Characteristics
The basic characteristics of the 13 eligible studies [-] are summarized in . These trials, conducted between 1999 and 2023, had sample sizes ranging from 80 to 566 participants, totaling 2942 across all studies. In total, 23% (3/13) of the trials [-] were conducted in high-income countries (England, the United States, and Australia), whereas the remaining 77% (10/13) [-] were conducted in low- and middle-income countries (China and Jordan). A total of 92% (12/13) of the studies [-,] reported on the eradication rate of H. pylori, 100% (13/13) [-] reported on patient compliance, 69% (9/13) [,,,,-,] reported on adverse events, and 23% (3/13) [,,] reported on patient satisfaction. The H. pylori eradication regimens included triple and quadruple therapies, with durations ranging from 7 to 14 days (). Control group patients received traditional oral and written medical instructions, whereas experimental group patients received additional intensive education instructions.
Table 1. Characteristics of the studies included in this meta-analysis.
Study
Year
Country
Type
Sample size, n
Age (y), mean
Female/male participants, n
NMEa method
Eradication regimen
Duration
Detection
Al-Eidan et al []
2002
England
Retrospective cohort study
80
50
22/54
TEL+b
Triple therapy
7 d
RUTc
Shoiab et al []
2023
Jordan
RCTd
200
—e
97/103
TEL+
Triple therapy
14 d
SATf
Lin et al []
2022
China
Retrospective cohort study
533
45
232/301
WeChat
Quadruple therapy
14 d
13C-UBTg
Wang et al []
2015
China
RCT
140
44
88/53
TELh
Triple therapy
10 d
13C-UBT
Henry and Batey []
1999
Australia
RCT
119
57
50/69
TEL+
Triple therapy
10 d
13C-UBT
Ma et al []
2021
China
RCT
566
—
—
WeChat
Quadruple therapy
14 d
14C-UBTi
Sun et al []
2022
China
RCT
226
44
128/98
WeChat
Quadruple therapy
14 d
UBTj
Lee et al []
1999
United States
RCT
125
49
90/35
TEL+
Triple therapy
14 d
—
Luo et al []
2020
China
RCT
222
50
134/88
WeChat
—
14 d
14C-UBT
Wang et al []
2019
China
RCT
310
46
148/162
SMS text messaging
Quadruple therapy
14 d
13C-UBT
Zhao et al []
2020
China
RCT
162
45
92/70
TEL+
Quadruple therapy
14 d
13C-UBT
Chen et al []
2021
China
RCT
196
44
91/105
TEL
Quadruple therapy
14 d
13C-UBT
Yang et al []
2023
China
RCT
254
35
133/121
WeChat
Quadruple therapy
14 d
13C-UBT
aNME: new media–based education.
bTEL+: telephone combined with other methods.
cRUT: rapid urease test.
dRCT: randomized controlled trial.
eNot available.
fSAT: stool antigen test.
gC-UBT: carbon-13 urea breath test.
hTEL: telephone.
iC-UBT: carbon-14 urea breath test.
jUBT: urea breath test.
Primary Outcome
H. pylori Eradication Rate
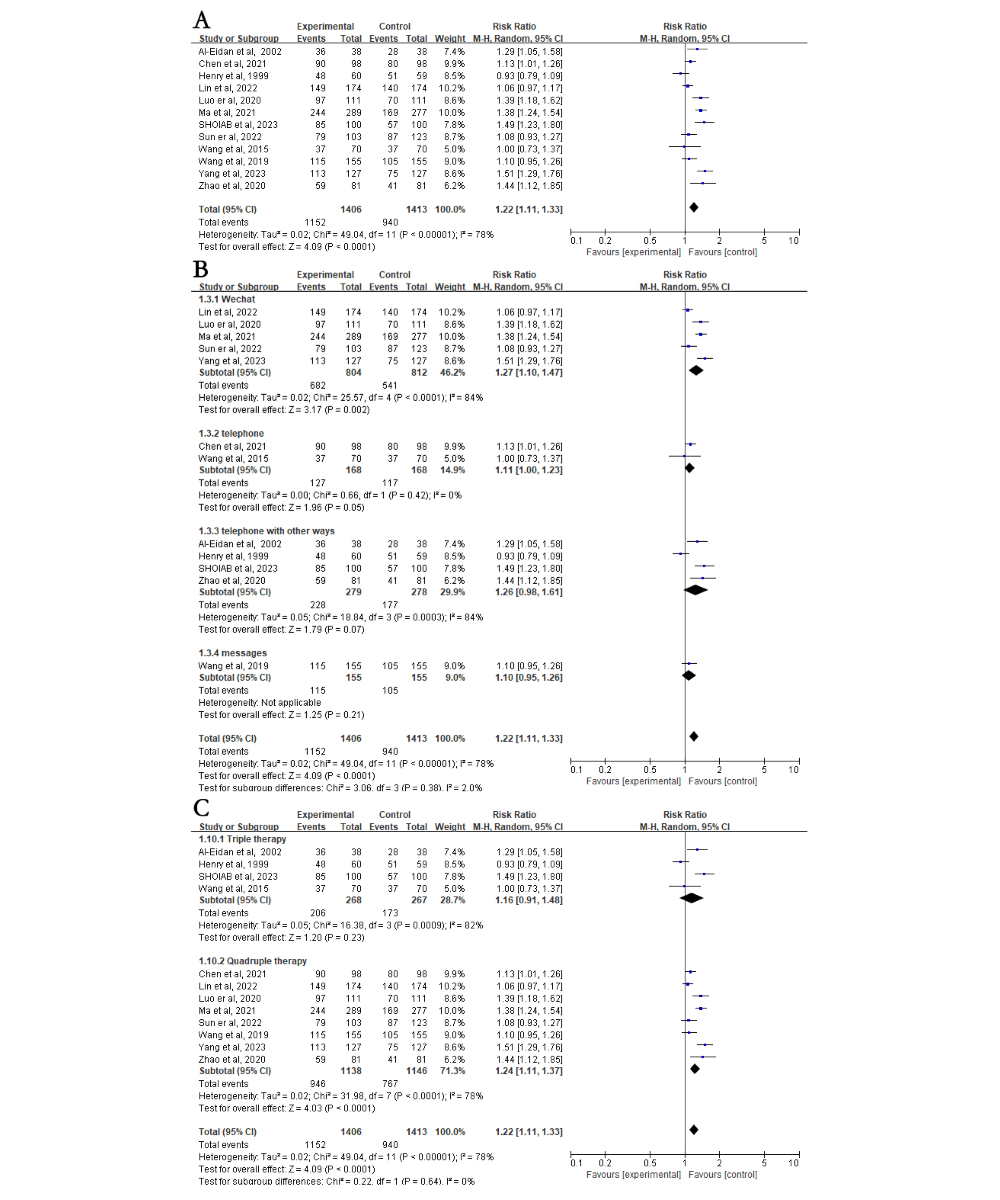
A total of 92% (12/13) of the studies involving 2819 patients reported data on patient H. pylori eradication rates. ITT analysis showed that eradication rates were significantly higher in the NME group compared with the control group (81.9% vs 67%; RR 1.22, 95% CI 1.11-1.33; P<.001; A [-]). A high level of heterogeneity was detected among the included studies (I2=78%; P<.001), but sensitivity analysis confirmed the stability of the results (A).
Figure 2. Forest plot comparing Helicobacter pylori (H. pylori) eradication in education versus control groups—subgroup analysis on intervention methods and regimens. (A) Forest plot comparing the H. pylori eradication rate between the education and control groups. (B) Subgroup analysis for H. pylori eradication rates based on different intervention methods. (C) Subgroup analysis for H. pylori eradication rates based on different treatment regimens. Control: traditional instructions; experimental: new media–based education instructions; fixed: fixed-effects model; random: random-effects model.
Subgroup Analysis of H. pylori Eradication Rate
Heterogeneous results require subgroup analysis. Subgroup analysis included different new media devices, different medication regimens, different age groups, the socioeconomic status of the country of origin, whether initial outpatient education was provided, and whether WeChat group functionality was used in conjunction with WeChat. In the intervention method subgroup, patients were categorized into WeChat, telephone, telephone with other methods, and SMS text messaging. In the medication regimen subgroup, patients were categorized into quadruple therapy and triple therapy. In the subgroup analysis of different populations, individuals were divided into age groups of ≤60 and >60 years and into high-income and low- and middle-income country groups based on the country of origin.
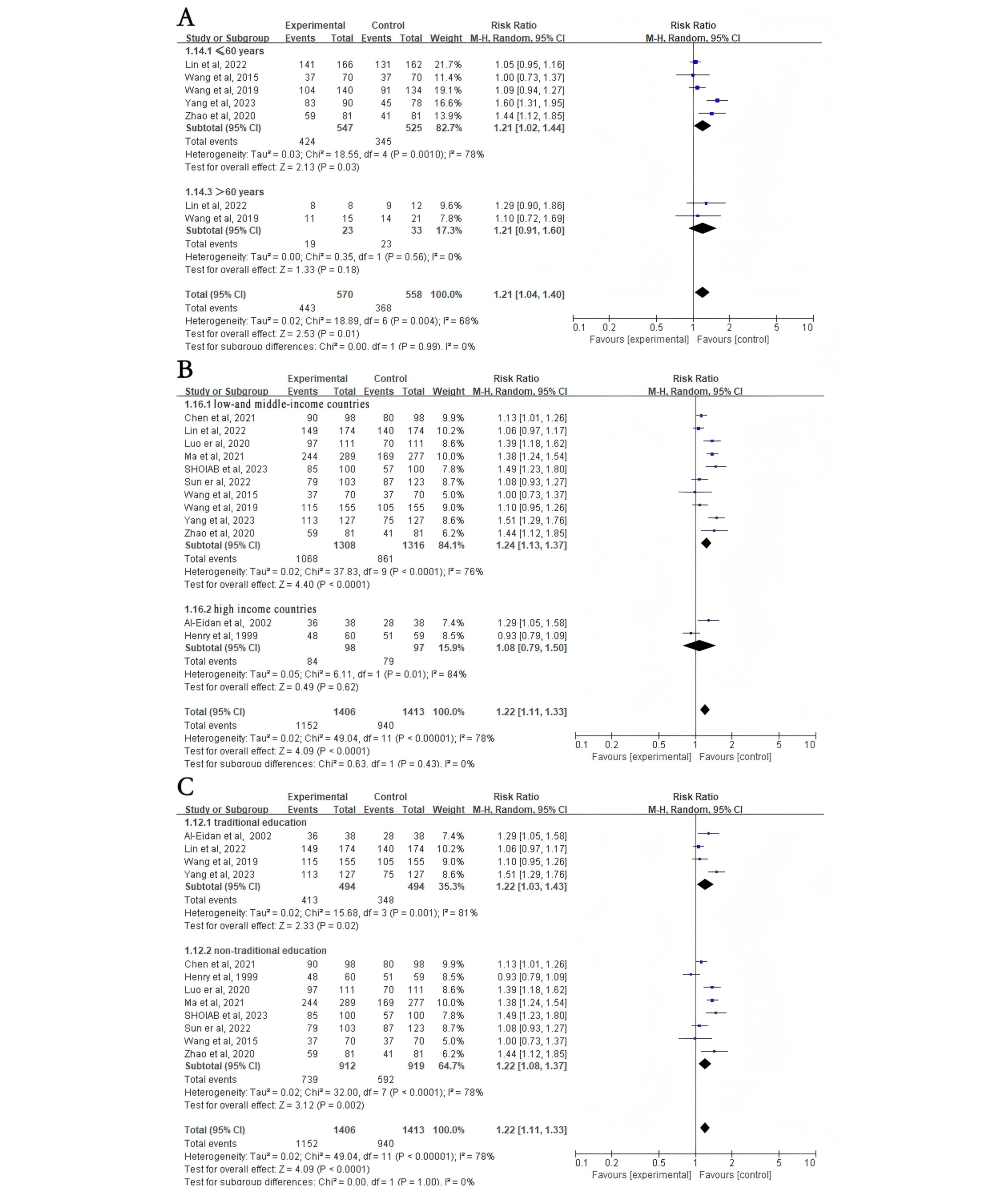
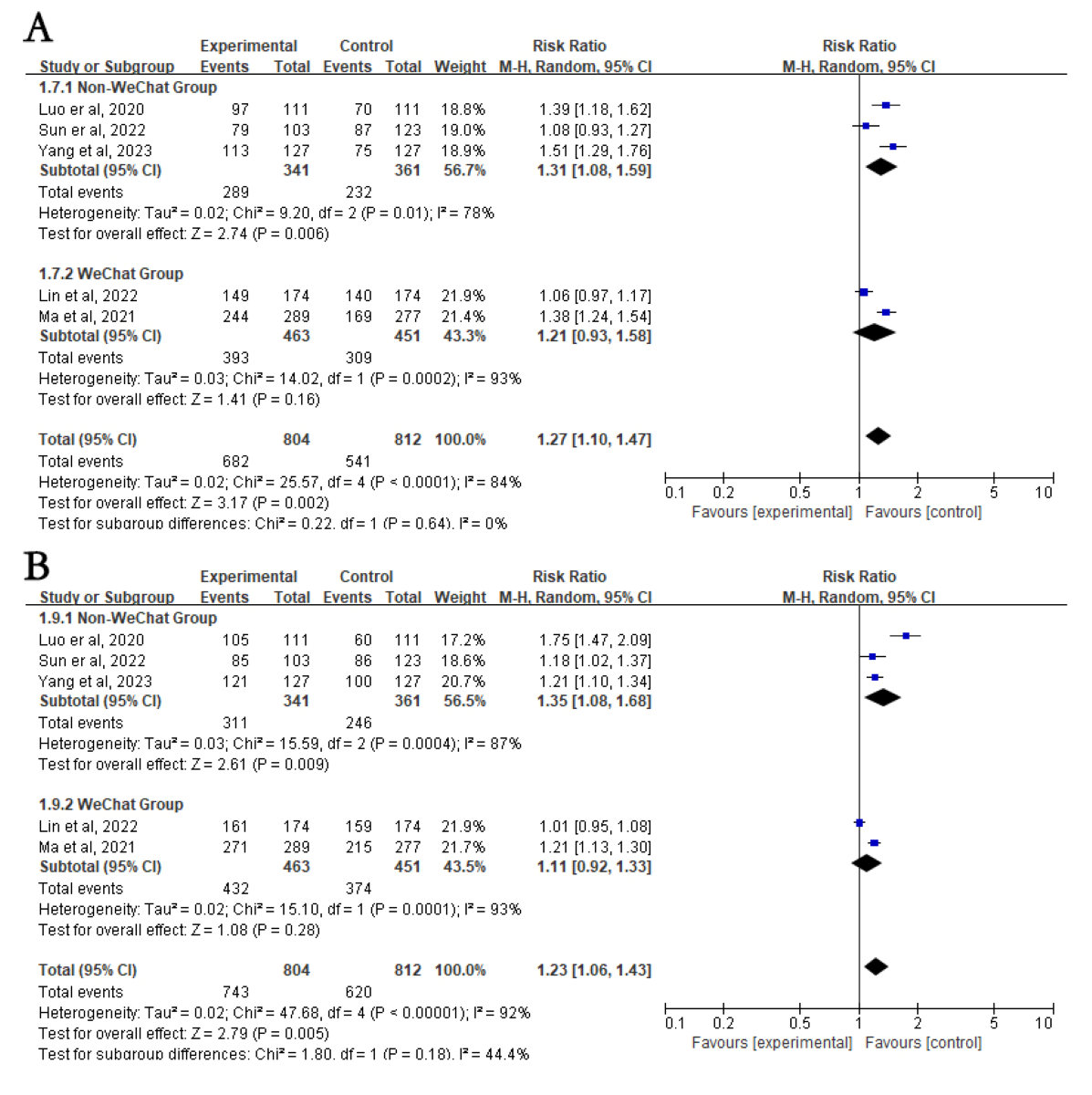
First, subgroup analyses were stratified according to different intervention methods. The intervention group had higher eradication rates in the WeChat subgroup (RR 1.27, 95% CI 1.10-1.47; P=.002; B). However, there was no difference in eradication rates between the intervention and control groups in the telephone (RR 1.11, 95% CI 1.00-1.23; P=.05), telephone with other methods (RR 1.26, 95% CI 0.98-1.61; P=.07), and SMS text messaging (RR 1.10, 95% CI 0.95-1.26; P=.21; B) subgroups. Subgroup analyses were then stratified according to different medication regimens. The intervention group had higher eradication rates than the control group in the quadruple therapy subgroup (RR 1.24, 95% CI 1.11-1.37; P<.001) but not in the triple therapy subgroup (RR 1.16, 95% CI 0.91-1.48; P=.23; C). In addition, compared to the control group, individuals aged ≤60 years had higher H. pylori eradication rates after NME (RR 1.21, 95% CI 1.02-1.44; P=.03), whereas those aged >60 years did not (RR 1.21, 95% CI 0.91-1.60; P=.18; A [-]). Interestingly, individuals from low- and middle-income countries showed significantly increased H. pylori eradication rates after NME compared to the control group (RR 1.24, 95% CI 1.13-1.37; P<.001), whereas there was no impact on individuals from high-income countries (RR 1.08, 95% CI 0.79-1.50; P=.62; B). Regardless of whether routine outpatient H. pylori eradication education was provided, NME yielded higher eradication rates in both the traditional (RR 1.22, 95% CI 1.03-1.43; P=.02) and nontraditional (RR 1.22, 95% CI 1.08-1.37; P=.002; C) education subgroup. Finally, using WeChat as a new media platform for H. pylori education, there was no significant difference in H. pylori eradication rates between the NME group and the control group when the WeChat group functionality was used (RR 1.21, 95% CI 0.93-1.58; P=.16; A [-]). However, when using WeChat for one-on-one education or other functionalities, the NME group showed higher H. pylori eradication rates (RR 1.31, 95% CI 1.08-1.59; P=.006; A). When the treatment duration was 14 days (RR 1.26, 95% CI 1.14-1.39; P<.001), the H. pylori eradication rate in the NME group was consistently higher than that in the control group (Figure S2A in ). However, when the duration was less than 14 days (RR 1.06, 95% CI 0.85-1.32; P=.61), there was no significant difference in eradication rates between the 2 groups (Figure S2A in ).
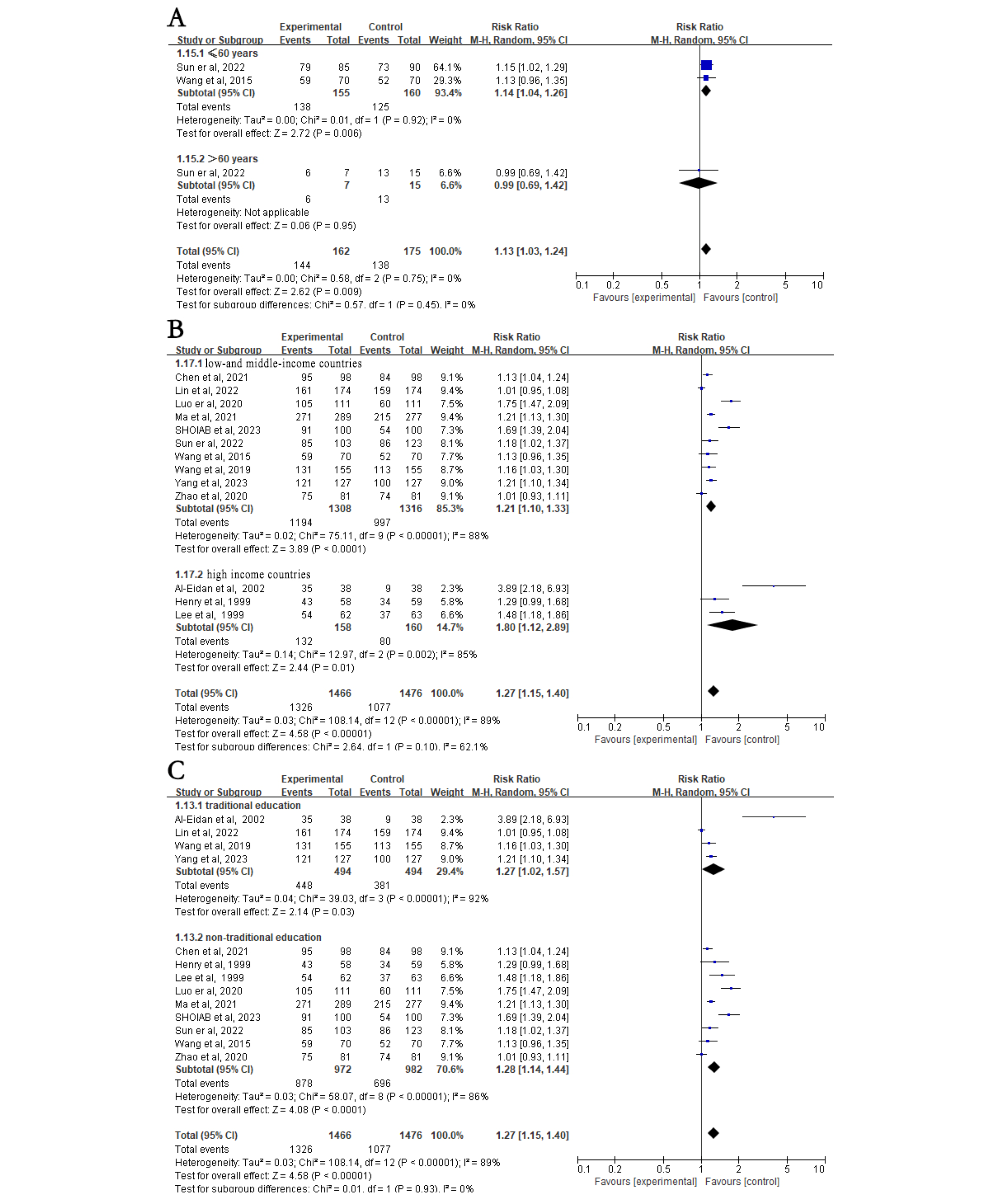
Figure 3. Subgroup analysis on Helicobacter pylori (H. pylori) eradication rates based on age (>60 years), country socioeconomic status (high income vs low and middle income), and education (traditional). (A) Subgroup analysis for H. pylori eradication rates based on whether patients were older than 60 years. (B) Subgroup analysis for H. pylori eradication rates based on whether patients were from high-income or low- and middle-income countries. (C) Subgroup analysis for H. pylori eradication rates based on whether patients received traditional education. Control: traditional instructions; experimental: new media–based education instructions. Figure 4. Subgroup analysis of Helicobacter pylori eradication rates and patient compliance based on whether patients used WeChat groups. (A) Subgroup analysis for Helicobacter pylori eradication rate. (B) Subgroup analysis for patient compliance. Control: traditional instructions; experimental: new media–based education instructions.
Patient Compliance
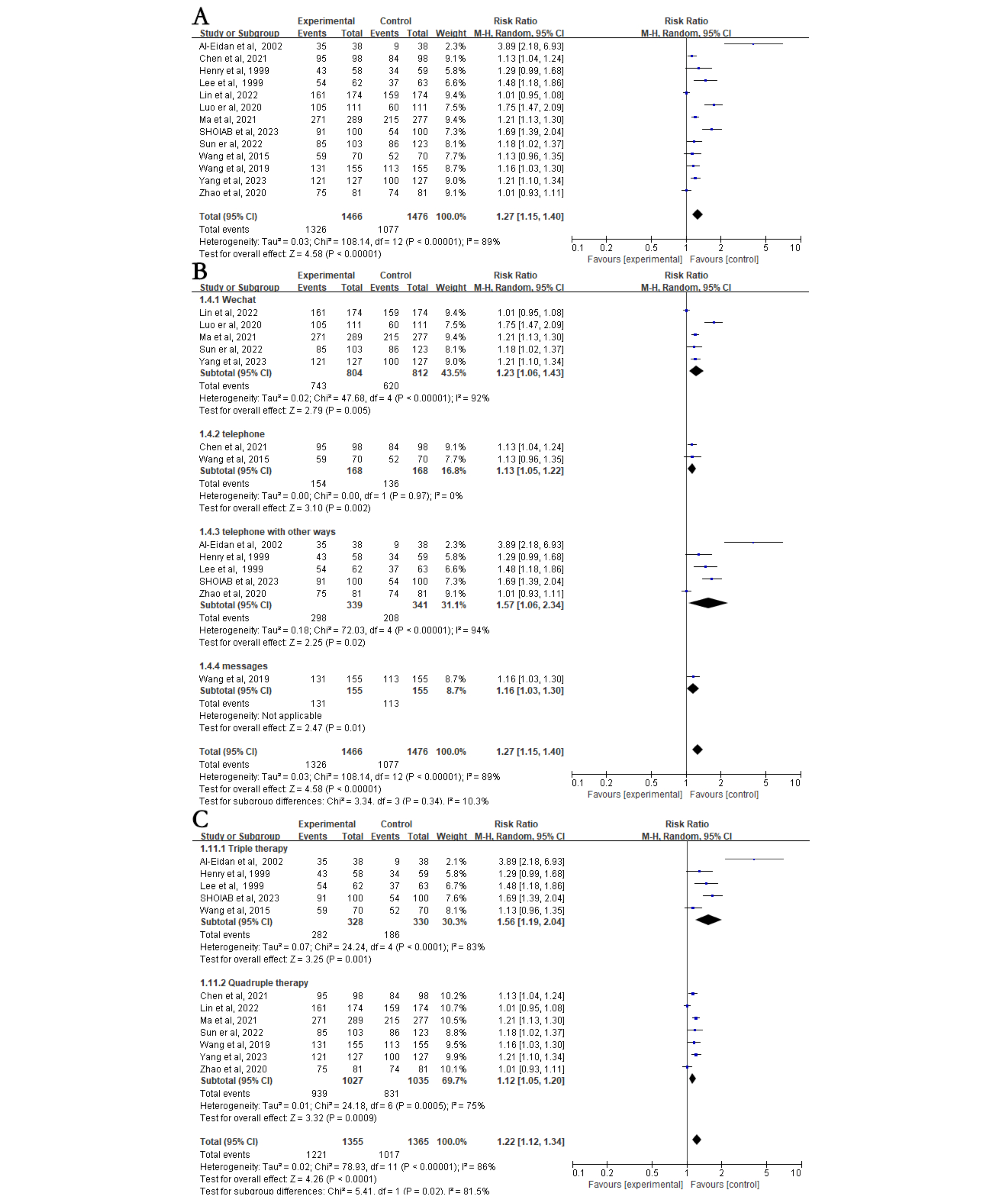
All 13 studies, involving 2942 patients, reported data on patient adherence. The analysis showed that patients in the NME group had significantly higher medication adherence compared to those in the control group (90.5% vs 73%; RR 1.27, 95% CI 1.15-1.40; P<.001; A [-]). There was high statistical heterogeneity between studies (I2=89%; P<.001), whereas sensitivity analysis showed stable results (A).
Figure 5. Forest plot comparing patient compliance in education versus control groups—subgroup analyses on intervention methods and regimens. (A) Forest plot comparing patient compliance between the education and control groups. (B) Subgroup analysis for patient compliance based on different intervention methods. (C) Subgroup analysis for patient compliance based on different eradication regimens. Control: traditional instructions; experimental: new media–based education instructions.
Subgroup Analysis of Compliance
A stratified analysis based on different NME methods and different medication regimens showed that the NME group clearly had better compliance than the control group using WeChat (RR 1.23, 95% CI 1.06-1.43; P=.005), telephone (RR 1.13, 95% CI 1.05-1.22; P=.002), telephone with other methods (RR 1.57, 95% CI 1.06-2.34; P=.02), SMS text messaging (RR 1.16, 95% CI 1.03-1.30; P=.01; B), triple therapy regimen (RR 1.56, 95% CI 1.19-2.04; P=.001), or quadruple therapy regimen (RR 1.12, 95% CI 1.05-1.20; P<.001; C). A stratified analysis based on patient age showed that NME group clearly had better compliance than the control group in the group aged ≤60 years (RR 1.14, 95% CI 1.04-1.26; P=.006) but not in the group aged >60 years (RR 0.99, 95% CI 0.69-1.42; P=.95; A). Another stratified analysis based on whether the patients were from high-income countries showed that the NME group clearly had better compliance than the control group in both the low- and middle-income country subgroup (RR 1.21, 95% CI 1.10-1.33; P<.001) and the high-income country subgroup (RR 1.80, 95% CI 1.12-2.89; P=.01; B [-]). Similarly, based on whether basic outpatient education was provided to all enrolled patients, the NME group clearly had better compliance than the control group in both the traditional education subgroup (RR 1.27, 95% CI 1.02-1.57; P=.03) and the nontraditional education subgroup (RR 1.28, 95% CI 1.14-1.44; P<.001; C). A stratified analysis based on whether WeChat group re-education was used showed that new media significantly increased patient compliance in the non-WeChat subgroup (RR 1.31, 95% CI 1.08-1.59; P=.009) but not in the WeChat subgroup (RR 1.21, 95% CI 0.93-1.58; P=.28; B). In the subgroup with a 14-day treatment duration, patient compliance was significantly higher in the NME group than in the control group (RR 1.24, 95% CI 1.12-1.37; P<.001; Figure S2B in ). In contrast, in regimens lasting less than 14 days, compliance did not differ significantly between the 2 groups (RR 1.65, 95% CI 0.97-2.82; P=.07; Figure S2B in ).
Figure 6. Subgroup analysis on patient compliance based on age (>60 years), country socioeconomic status (high income vs low and middle income), and education (traditional). (A) Subgroup analysis for patient compliance based on whether patients were older than 60 years. (B) Subgroup analysis for patient compliance based on whether patients were from high-income or low- and middle-income countries. (C) Subgroup analysis for patient compliance based on whether all patients received traditional education. Control: traditional instructions; experimental: new media–based education instructions.
Secondary Outcomes
Adverse Events
Adverse drug reactions were documented in 69% (9/13) of the studies. The primary adverse events reported included diarrhea, constipation, nausea, abdominal pain, taste disorder, and skin rash. No significant differences were found between the NME and control groups (RR 0.88, 95% CI 0.71-1.09; P=.23; Figure S3A in ). Although significant heterogeneity was present among the studies (I2=63%; P<.001), the findings remained stable in sensitivity analysis (Figure S3A in ).
Patient Satisfaction
A total of 23% (3/13) of the studies, involving 672 patients, provided data on patient satisfaction. Patient satisfaction in the NME group was notably higher than that in the control group (61% vs 47.7%; RR 1.30, 95% CI 1.13-1.49; P<.001). Low statistical heterogeneity was observed (I2=0%; P=.47; Figure S3B in ).
Sensitivity and Publication Bias Analyses
The results of this study revealed some statistical heterogeneity, which may be attributed to factors such as intervention frequency, intervention duration, patient source (ie, patients from high-income vs low- and middle-income countries), and variation in eradication regimens. Given that heterogeneity is a major concern in meta-analysis, we conducted sensitivity analyses by sequentially excluding individual studies. The pooled results for all 4 main outcomes (H. pylori eradication rate, patient compliance, adverse events, and patient satisfaction) remained stable. In addition, subgroup analyses were conducted according to intervention type, treatment regimen, age group, country socioeconomic status, provision of baseline outpatient education, and use of the WeChat group functionality.
For publication bias, we first conducted visual inspection of funnel plots and then applied the Egger linear regression test and Begg rank correlation test for the 2 primary outcomes (H. pylori eradication rate and patient compliance) as both included ≥10 studies. Although mild asymmetry was observed in the funnel plots upon visual inspection (Figure S4 in ), statistical tests did not suggest significant publication bias. For H. pylori eradication rate, the Egger test resulted in P=.93, whereas the Begg test showed a Kendall tau with continuity correction of −0.05 (P=.84). Similarly, for patient compliance, the Egger test resulted in P=.20, and the Begg test reported a Kendall tau with continuity correction of 0.32 (P=.13). These findings indicate a low likelihood of publication bias; however, the slight visual asymmetry warrants cautious interpretation of the results.
Discussion
Principal Findings
This meta-analysis delved into the impact of NME on H. pylori eradication rates using platforms such as the internet or mobile communication. Overall, NME exhibited superiority over traditional education in both H. pylori eradication rates and patient compliance. Specifically, interventions via WeChat demonstrated clear advantages over telephone and SMS text messaging interventions. However, in comparison to traditional education, NME did not significantly ameliorate the overall occurrence rate or specific adverse reactions.
Compared with previous meta-analyses [-], our study included a larger and more recent set of trials (13 studies up to February 2025), thereby enhancing statistical power and ensuring that the evidence reflected the latest data. Moreover, we conducted more comprehensive subgroup analyses, not only covering intervention type, treatment regimen, patient satisfaction, and adverse events but also further exploring patient age, country socioeconomic status, provision of baseline outpatient education, and WeChat intervention models (personalized one-on-one vs group based). These additional analyses allowed us to better explain heterogeneity and provide novel insights into the applicability and optimization of NME strategies across different populations and social contexts.
Patient compliance stands as a pivotal factor contributing to the poor eradication rate of H. pylori. Adequate compliance is pivotal for ensuring the correct implementation of any eradication program, whereas poor compliance often leads to failure [,]. Therefore, educational interventions aimed at enhancing patient compliance are essential. Particularly with quadruple therapy, which yields better H. pylori eradication effects than triple therapy but entails a broader spectrum of drugs and necessitates more frequent dosing, patients may easily overlook or miss doses []. Thus, based on the findings of this study, NME significantly bolsters H. pylori eradication rates in the quadruple therapy population.
Compared to other strategies to enhance eradication rates, such as selecting antibiotics based on drug susceptibility, educational interventions are deemed cost-effective and straightforward []. Furthermore, education can augment patient awareness of H. pylori, foster self-management, and facilitate physician-patient communication []. NME holds even more promise than traditional education methods as it equips patients to better comprehend treatment regimens, provides convenient information on adverse drug reactions and health knowledge, and offers more interactive solutions to patients’ issues []. Particularly in low- and middle-income countries, where the average educational attainment level may not match that of high-income nations, repetitive education via new media can significantly enhance understanding and, thereby, improve H. pylori eradication rates.
The intervention measures used in the studies included in this review encompassed telephone follow-ups, SMS text message reminders, and WeChat consultations. WeChat interventions were used in 38% (5/13) of the studies, all of which showcased its effectiveness in enhancing the eradication rate. WeChat serves as a valuable platform for timely communication between patients and physicians, facilitating the prompt resolution of medication-related issues.
It is pertinent to note the limitations of emerging technologies such as WeChat. The inference drawn from this study is that older individuals, who are less inclined to adopt electronic devices, may not derive as much benefit from WeChat software education. Conversely, younger and middle-aged individuals exhibit greater receptiveness to new technologies, thereby perfectly exemplifying the advantages of WeChat education. Notably, our findings suggest that education delivered through WeChat groups may be less effective compared to one-on-one interactions. This difference may be attributed to several factors. First, group-based education often lacks personalization and may dilute individual responsibility, leading to lower engagement. Second, patients may be reluctant to discuss personal health issues in a group setting due to perceived privacy concerns. Third, the passive nature of group messages can result in reduced attentiveness and limited interaction. In contrast, stand-alone applications or supervised one-on-one education offer more tailored support, thereby enhancing compliance and H. pylori eradication rates. Due to the absence of direct comparative studies across different NME delivery modes, the most effective approach or combination of methods remains uncertain.
The internet and smartphones have revolutionized information access, and mobile health apps can effectively deliver patient education []. Given the exponential growth of medical apps, evaluating their capacity to provide comprehensive health education is imperative [].
Enhancing patient compliance is not associated with potential adverse events. Given that treatment regimens usually incorporate antibiotics, side effects are often attributed to antibiotic-related adverse events []. However, different treatment schemes yield varying side effects, underscoring the significance of precisely defining adverse events in this context []. While fortified NME can mitigate adverse emotions and mild discomfort stemming from side effects through enhanced physician-patient communication, its efficacy in reducing the occurrence rate of side effects remains limited.
Given the limitations of certain studies, the findings of this review warrant cautious interpretation. Primarily, most studies (10/13, 77%) were conducted in Asia, with only 23% (3/13) originating from Western countries. This underscores the necessity for trials encompassing diverse ethnic groups as the H. pylori infection rate varies across geographic regions []. Consequently, prudence should be exercised when extrapolating the conclusions to other regions. Second, the overall sample size was relatively modest. The absence of multicenter and large-sample studies amplifies the potential for bias and error, underscoring the need for additional rigorously designed experiments. Third, the interventions spanned a spectrum across the study sample, rendering it challenging to draw overarching conclusions. Meanwhile, although this review primarily relied on RCTs, it also included 2 retrospective cohort studies. Despite a certain level of comparability in terms of intervention content and study quality, it is important to note that differences in study design may introduce additional systematic bias, thereby weakening the strength of the conclusions. Finally, all fortified education methods engendered a selection bias toward specific demographic groups. For instance, WeChat education may not be viable for patients without smartphones. Consequently, these intervention measures may not fully capture patients with diverse educational backgrounds and economic statuses. Therefore, future research should prioritize the inclusion of more high-quality RCTs while also expanding intervention approaches tailored to diverse populations to enhance the external validity and generalizability of the findings.
Conclusions
In summary, the findings suggest that NME holds promise in increasing the H. pylori eradication rate, particularly when implemented via mobile phone apps. Nevertheless, intervention methods and designs exhibit considerable heterogeneity, necessitating ongoing high-quality research. Furthermore, the evolution of artificial intelligence technology has shifted the focus of medical and health education from the populace to the individual level. Hence, deliberating on the creation of personalized education programs and their integration into clinical practice is imperative.
This study was supported by the Postgraduate Research & Practice Innovation Program of Jiangsu Province (SJCX25_0794). The funders had no role in the study design, data collection, data analysis, interpretation of the results, or manuscript writing. The authors declare that no generative artificial intelligence tools were used in any portion of manuscript writing.
The datasets generated or analyzed during this study are available from the corresponding author on reasonable request.
FY contributed to conceptualization, resources, project administration, and supervision. WF contributed to methodology, formal analysis, investigation, and writing original draft. YT contributed to methodology, data curation, and writing review and editing. JS contributed to validation and visualization.
None declared.
Edited by A Mavragani, A Stone; submitted 01.Jun.2025; peer-reviewed by B-G Zhou, Y-J Fang, M Abuelazm; comments to author 26.Aug.2025; revised version received 15.Sep.2025; accepted 23.Sep.2025; published 23.Oct.2025.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research (ISSN 1438-8871), is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.
This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!
Glenn Close has joined the cast of the Spanish drama The Black Ball (La Bola Negra), the new film from the writing-directing team of Javier Calvo and Javier Ambrossi (Veneno, The Messiah). Produced by Movistar Plus+ and Suma Content Films,…
This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!