Normington could minimally dress the yacht when needed, but most of her changes were to ensure continuity between the real ship and the sets her team built at Shepperton Studios, a film studio built outside of London. The sets included the…
Overall, 54 patients with SGC were included in this study. The most frequent entity was salivary duct carcinoma (SDC; 43.6%), followed by acinic cell carcinoma (ACC; 24.1%), mucoepidermoid carcinoma (MEC; 22.2%), and secretory carcinoma (Sec; 11.1%). The mean age across the whole cohort was 57.7 (± 17.5) years, and 46.3% of all patients were female. Most patients (57.7%) had T1/2 tumors. Among SDC, 81.1% were androgen receptor (AR)-positive, and 54.5% showed nuclear AR positivity in > 70% of tumor cells (ARhigh), whereas 45.5% showed nuclear AR positivity in ≤ 70% of tumor cells (ARlow). Furthermore, 36.4% of the SDC were positive for human epidermal growth factor receptor 2 (HER2; score 3 + or HER2-amplified). The primary therapy was surgery in 98.1% of cases, and chemoradiation in 1.9% of cases. Neck dissection was performed in 74.1% of the cases, and 57.4% of the patients received adjuvant (chemo-)radiation therapy. Detailed data for the specific entities are presented in Table 1.
Table 1 Clinicopathological data
With a median follow-up of 63.5 months for the entire cohort, SDC patients showed the most unfavorable five-year OS (50.6%), followed by MEC (83.3%), ACC (83.9%), and Sec patients (100.0%). Five-year RFS rates were 30.7% for SDC, 69.2% for ACC, 83.3% for MEC, and 66.7% for Sec. Moreover, five-year RFP was 39.9% for SDC, 69.2% for ACC, 91.7% for MEC, and 66.7% for Sec. Lastly, five-year DCR was 47.0% for SDC, 69.2% for ACC, 100.0% for MEC, and 83.3% for Sec.
A 13-marker IMC panel identifies distinct immune cell and CAF subsets in nonMYO SGC
We used tissue from SGC primaries and metastases from 54 patients with SGC to create a tissue microarray (TMA). Tissue sections from TMA were stained with a cocktail of 13 metal-conjugated antibodies. Ablation of the tissue slices produced single-channel images that were used to generate multichannel images. After segmentation, the cells were categorized into cellular subsets. The cellular frequencies and results from the spatial analyses were then correlated with clinical parameters and patient outcomes (Fig. 1A).
Fig. 1
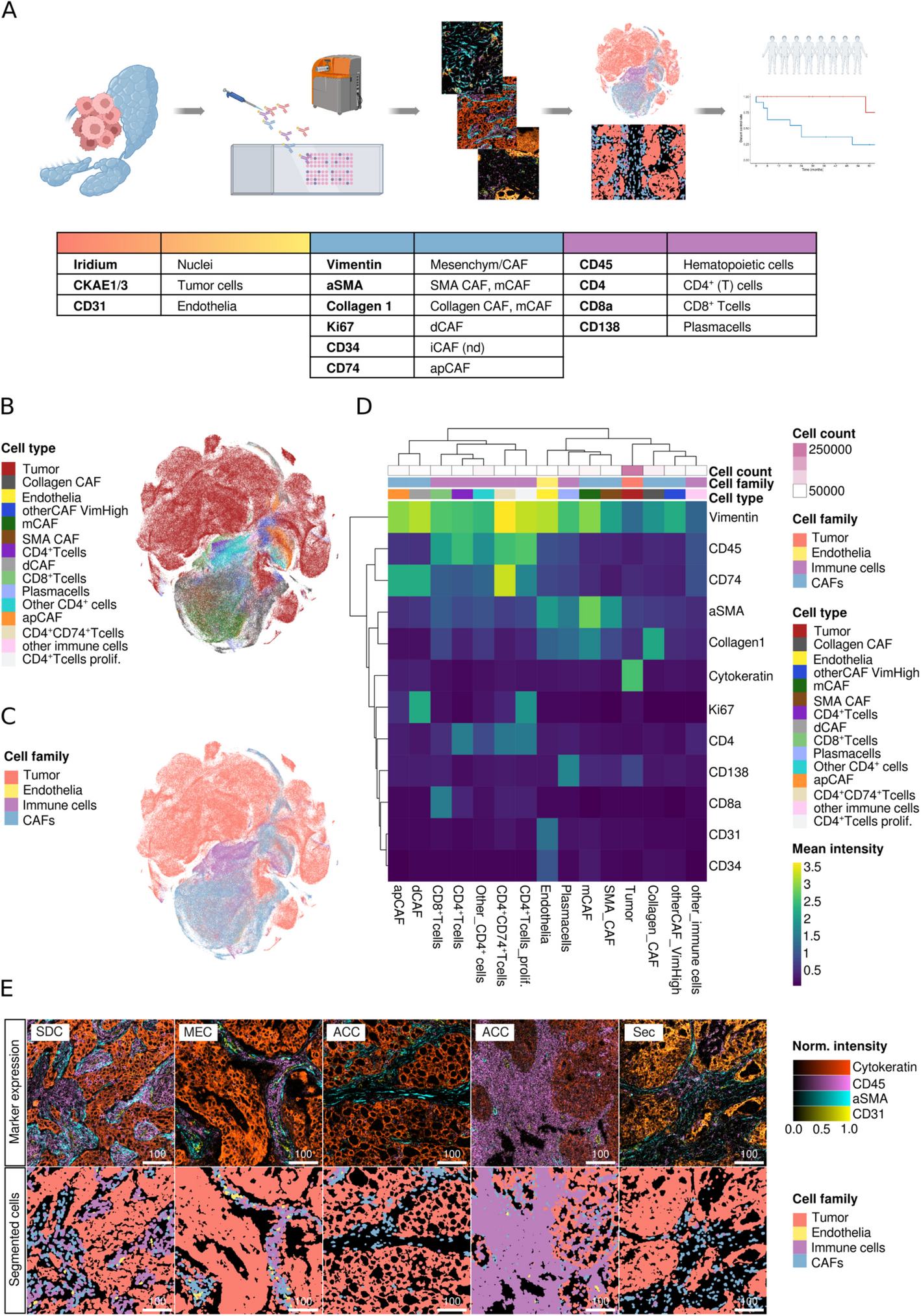
Phenotyping of the cellular SGC TME. A Overview of the study: SGC samples from 54 patients were captured on a TMA, which was incubated with 13 metal-conjugated antibodies and ablated using a Hyperion system. Through image segmentation, a spatially-resolved single cell dataset was obtained and cell phenotyping was carried out in a semi-supervised fashion with established cell type markers. Cell frequencies and cellular neighborhoods were then correlated with clinical data. B tSNE plots of all 408.939 cells colored by cell type and (C) cell category. D Heatmap depicting the mean marker expression by cell type. E Representative images of the tumor architecture by marker expression (top row) and cellular composition after phenotyping (bottom row). 100-micron scale bars
After the thorough exclusion of non-tumor-bearing TMA cores, we analyzed 199 SGC TMA cores from 54 SGC, including 188 primaries and 11 metastases from SDC, ACC, MEC, and Sec. A median cell count of 3,019 (ACC), 2,274 (Sec), 2,104 (MEC), and 2,029 (SDC) per 1 mm2 ROI was noted. Using a stepwise Gaussian mixture model of cytokeratin expression and SOM clustering, we measured the expression of 13 different markers in 408,939 cells, (Fig. 1B and C). First, we separated tumor cells (CKAE1/3+; n = 266,172) from endothelial cells (CD31+, CKAE1/3−; n = 1,349), immune cells (CKAE1/3−, CD45+, or CD138+; n = 50,432), and CAFs (CKAE1/3/CD45/CD31/CD138−; n = 90,986). Immune cells were then clustered into plasma cells (CD138+), CD8+ T cells, CD4+ T cells, and weakly CD4-expressing cells, which are most likely monocytes or other myeloid-derived cells (other CD4+cells; [5, 12, 19]). CD4+ T cells were subclassified as CD4+CD74+ T cells, which most likely correspond to effector Tregs [20, 21], proliferating CD4+ T cells (Ki67+), and other CD4+ T cells. Immune cells solely expressing CD45 were classified as “other immune cells.” To classify CAFs, we adopted an IMC-validated classification scheme proposed by Cords et al. [5, 25], separating mCAFs (SMA+Collagen1+), Collagen CAFs (SMA-Collagen1+), SMA-CAFs (SMA+Collagen1−), dCAFs (Ki67+, Vimentin+), and apCAFs (CD74+, Vimentin+). We also included CD73, IDO, and CD34 to detect rCAFs, ifnCAF/IDO CAFs, and iCAFs, respectively. However, the CD73 and IDO antibodies used did not produce a specific IMC signal. We could not discriminate iCAFs, since all CD34+ cells co-expressed CD31, a specific vascular marker, which was used to identify endothelia. Two subsets of cells did not display a specific marker profile: cells without expression of any of the markers used were designated as tumor cells, as they were located in tumor cell patches. Regarding the TME-centered focus of this work, we reasoned that this conservative approach would not impact TME-cell classification and thus minimize the chance of false-positive results. Cells with sole expression of Vimentin were classified as “other CAFs” with Vimentin expression (Fig. 1D). Figure 1E displays representative ROIs of the included tumor entities as multiplex images and the corresponding cellular maps after segmentation and cell phenotyping.
SGC entities are characterized by different TME cell frequencies
When pooling all ROIs, the cell type distribution across SGC tumor types displayed marked differences with a prominent immune cell compartment in ACC (Supplementary Figure S1C and D). No prominent differences in cell category contributions were noted when comparing primaries and metastases or peripheral and central tumor regions (Supplementary Figure S1E and F).
To account for differing numbers of ROIs per patient due to the exclusion of non-tumor-bearing and torn TMA cores, we calculated the median cell frequency per patient and compared the distribution of cells across the different SGC entities. We found a significantly varying abundance of immune cell subsets across tumor types (Fig. 2A), which was largely due to significantly elevated levels of CD4+ T cells (p = 0.03), CD8+ T cells (p = 0.04), other CD4+ cells (p = 0.03), and unclassified immune cells (p = 0.04) in ACC. This resulted in a significantly higher frequency of overall immune cells in ACC (p = 0.04; Fig. 2B and C).
Fig. 2
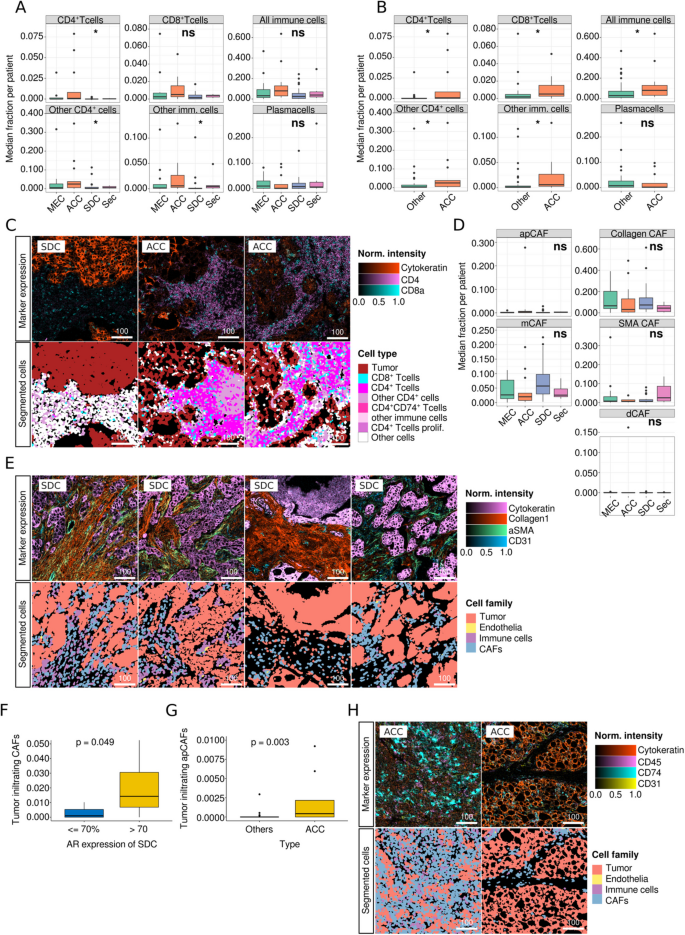
Comparison of median cell frequencies per patient across tumor subtypes (A) Immune cell subsets across SGC entities. B Immune cell subsets in ACC vs. other carcinoma types. C Representative core immune marker expression (top row) and selected immune cell subsets in SDC versus ACC. D Frequencies of CAF subtypes across SGC entities. E Examples of the spectrum of core CAF marker expression (top row) and cell categories (bottom row) in SDC. F Frequency of tumor-infiltrating CAFs dependent on AR expression in SDC. G Frequency of tumor-infiltrating apCAFs in ACC versus other SGC subtypes. H Representative images of CD74+ expression in apCAFs in ACC (top row) and corresponding cell categories after segmentation (bottom row). 100-micron scale bars
Although the overall distribution of CAFs did not significantly vary in SGC types (Fig. 2D), we detected the highest mean frequency of mCAFs in SDC, a CAF subset that has been associated with ECM production. However, in direct comparison with other entities, this elevation was not significant (Supplementary Figure S2A), probably because of the broad spectrum of mCAF frequencies within SDC (Fig. 2D and E).
We also analyzed the frequency of tumor-infiltrating CAFs using tumor patch detection (Supplementary Figure S2B). As AR and HER2 are frequently expressed in SDC and are molecular targets for systemic therapy approaches [26], we examined the association between AR/HER2 expression and CAF frequency. We were able to show that the number of tumor-infiltrating CAFs was significantly elevated in ARhigh SDC compared to ARlow tumors (p = 0.049; Fig. 2F). No other significant cellular TME alterations were noted when SDC was subgrouped based on AR (Supplementary Figure S2C-E) and HER2 status (Supplementary Figure S2F-H). In contrast, in direct comparison to other tumor types, ACC displayed elevated levels of tumor-infiltrating apCAFs (p = 0.003; Fig. 2G and H, Supplementary Figure S2I). However, the frequency of these cells was generally very low. No significant differences in tumor-infiltrating immune cells were noted across SGC tumor types (Supplementary Figure S2J).
Spatial interaction analyses reveal a co-localisation of mCAFs with intratumoral vasculature
The spatial composition of the TME is an integral feature of tumor biology and influences the response to immunotherapy and patient outcomes [27]. Therefore, we leveraged the spatial information preserved in the dataset.
After computing a spatial interaction graph (examples in Supplementary Figure S3A), we clustered cells based on their 20 nearest neighbors into 9 cellular neighborhoods (CN; Fig. 3A and B). We found that the tumor cell-rich neighborhoods were largely devoid of CAFs and immune cells (CN1 and CN3). In contrast, CD4+ T cells, proliferating CD4+ T cells, other CD4+ cells, and CD8+ T cells formed a distinct lymphocyte-rich cluster (CN9, Fig. 3C). Another immune-related CN mainly consisted of CD4+CD74+ T-cells, apCAFs, and dCAFs.
Fig. 3
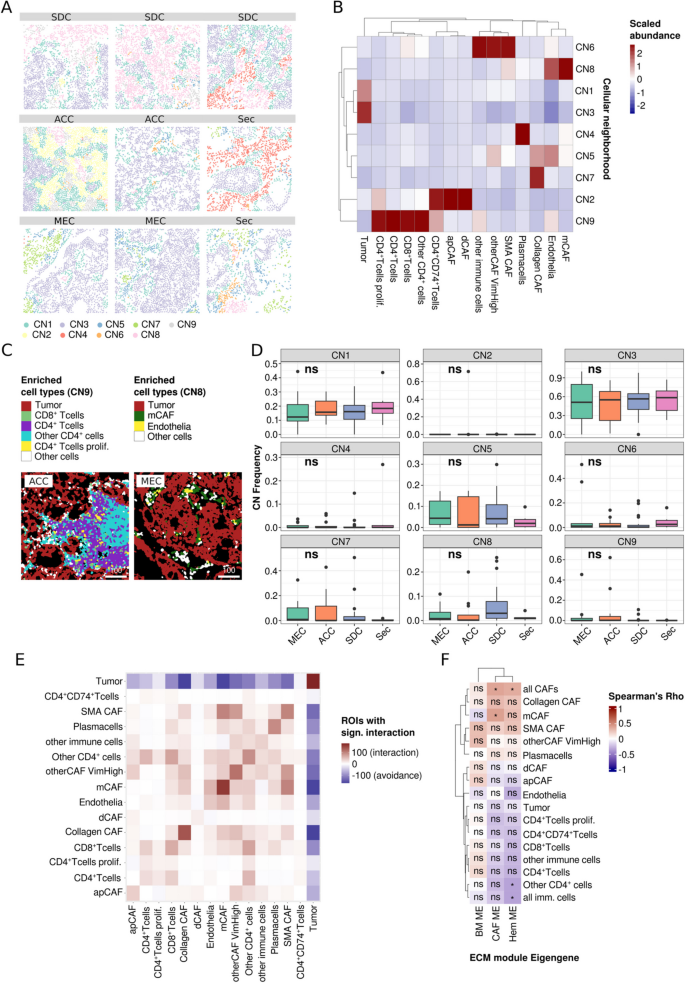
Spatial analysis of the TME of SGC and correlation with ECM protein modules. A Exemplary ROIs with cells colored by cellular neighborhood (CN). B Scaled cell abundance per CN. C Representative ROI rich in cells that mainly contribute to CN9 (ACC) and CN8 (MEC). D Frequency of CN across SCG types. E Spatial interaction of cell types colored by the number of ROIs with significant co-localization of two cell types. A red color indicates more ROIs with significant interaction while blue tiles indicate more ROIs with significant avoidance of two cell types. F Correlation of cell types with ECM module eigengenes which were published previously. Symbols within the tiles indicate the test significance (* p < 0.05, ns not significant). 100-micron scale bars
However, as the contributing cell types, the latter CN occurred at very low frequencies (CN2, Supplementary Figure S3B). SMA CAF and mCAFs contributed to two distinct CN with partial overlap (CN 6 and 8, respectively; Supplementary Figure S3C). Interestingly, the matrix-associated CAF-rich (mCAF-rich) CN8 displayed a strong contribution to endothelia (Fig. 3C). No specific marker for vCAFs, another cell type that was found to be associated with endothelia by Cords et al., was available in this panel. However, in contrast to mCAFs, very low expression of SMA and Collagen1 was reported in vCAFs [12], allowing for discrimination between the two cell types.
Although we did not observe significant differences in CN frequencies across SGC types, immune cell-rich CN was distinctively enriched in ACC. In addition, in SDC, we noted higher frequencies of the mCAF-rich CN8, but not of CNs 5, 6, and 7, which have high contributions of Collagen CAFs and SMA CAFs (Fig. 3D, Supplementary Figure S3C and D).
The CN analyses were complemented by a more direct spatial interaction analysis, as proposed by Schapiro et al. [22] (Fig. 3E). This approach compares the spatial interactions of cell type pairs with a null distribution in each ROI. The number of ROIs with significant positive (red) and negative (blue) interactions can then be summarized and graphically displayed. This methodically different analysis largely validated the aforementioned results, indicating potential interactions among immune cells and between mCAFs and endothelia as well as SMA CAFs. Again, mutual exclusion of TME and tumor cells was noted.
In summary, we describe distinct spatial cellular TME neighborhoods in SGC that largely show a mutually exclusive predominance of tumor cells, immune cells, and CAFs. However, mCAFs and Collagen CAFs tend to localize in proximity to the tumor vasculature.
CAFs and particularly mCAFs are associated with a distinct ECM profile
Recently, we dissected the ECM of SGC using an unbiased proteomic approach and discovered three protein clusters (“ECM modules”) that explain ECM differences across SGC tumor types via module Eigengenes (i.e., the resulting vector of the module’s proteomic signature) [15]. Using gene set enrichment analysis, these modules were biologically annotated and found to be enriched for classic CAF-associated (CAF-module), basement membrane-associated (BM-module), and peripheral blood-associated (Hem-module) biological terms. The most significant members of the latter include coagulation-related factors such as kallikrein, kininogen, prothrombin, plasminogen, and angiotensin. Since CAFs are considered the main source of ECM in carcinomas, we leveraged an overlap of 40 patients between that and the present SGC cohort and correlated the module Eigengenes with the cell type frequencies (Fig. 3F), thereby establishing a connection between the ECM and the cellular TME. As anticipated, we observed a strong positive correlation between CAFs with a more classic myofibroblastic phenotype (mCAF, Collagen CAF, SMA CAF) and the CAF protein module. However, only the correlation between mCAFs and overall CAFs was significant. In contrast, all immune cell subsets, except for plasma cells, were negatively correlated with the CAF module. Unexpectedly, very similar associations were found for the Hem-module, including an anti-correlation with endothelia and all immune cell subsets except plasma cells. We previously reasoned that this module consists of blood-related factors that are deposited within the ECM. However, the present data indicate that this does not imply exaggerated vasculature or deposition of cellular components of the peripheral blood. The BM module was mainly expressed in SGC with myoepithelial differentiation (e.g., adenoid cystic carcinomas), which were not analyzed in the present study.
Together, these data clearly link SGC mCAFs, Collagen CAFs, and SMA CAFs to an increase in classical CAF-associated ECM proteins and provide evidence that the ECM components of the CAF and the Hem module participate in an immune-exclusive TME.
Metastasis-associated signatures are enriched in tumor niches with a co-localization of mCAFs and endothelia and the interaction may be mediated by specific gene signatures
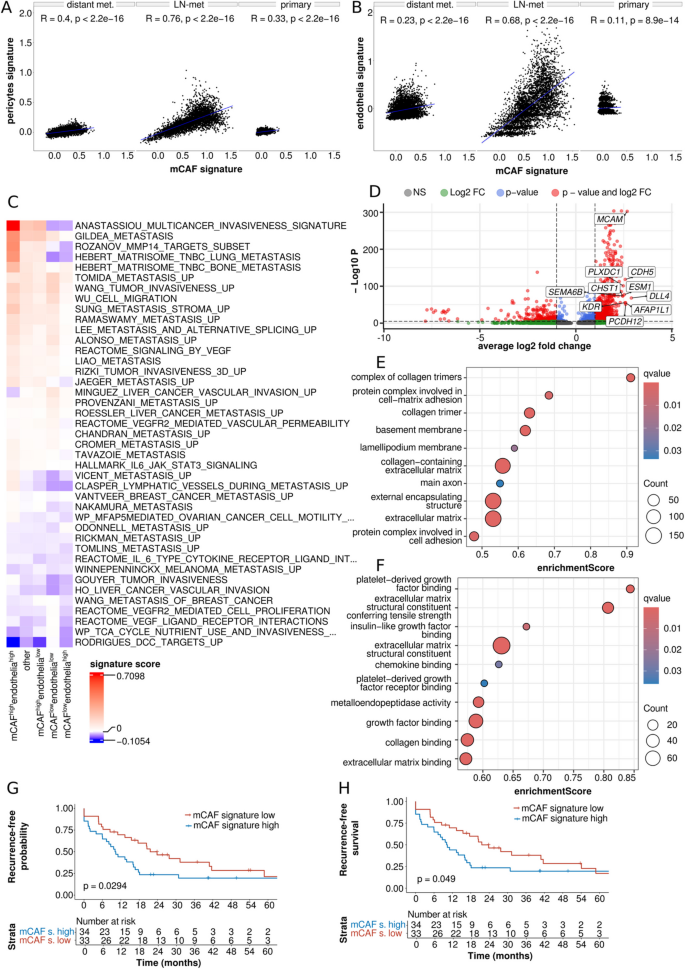
A significant positive correlation between mCAF-like and pericyte as well as endothelia signatures found in all three ST SDC data sets additionally supported the previously identified spatial co-localization of mCAFs and intratumoral vasculature (Fig. 5A and B; Supplementary Figure S5A and S5B).
A marked enrichment of metastasis-associated signatures such as “ANASTASSIOU_MULTICANCER_INVASIVENESS_SIGNATURE”, “GILDEA_METASTASIS”, “ROZANOV_MMP14_TARGETS_UP”, and “HEBERT_MATRISOME_TNBC_LUNG_METASTASIS” among others in mCAFhighendotheliahigh and a simultaneous depletion of those signatures in mCAFlowendothelialow ST spots (Fig. 5C) supported our previous clinically-based findings indicating that the spatial interaction of mCAFs and endothelia may be associated with metastasis. Notably, enrichment of metastasis-associated signatures was markedly higher in mCAFhighendotheliahigh than in mCAFhighendothelialow spots. In line with these findings, the invasiveness suppressing signature “RODRIGUES_DCC_TARGETS_UP” [28] was markedly depleted in mCAFhighendotheliahigh tumor niches. Alternative cut-offs for spot classification were evaluated and led to similar results, demonstrating the robustness of this approach (Supplementary Figure S6 A and B).
DE analysis followed by GSEA for mCAFhighendotheliahigh versus all other spots was performed to identify which factors may mediate the interaction between mCAFs and endothelia and therefore may be associated with metastasis of SDC (Fig. 5D-F and Supplementary Fig. 5 C). Notably, beside several ECM-/fibroblast-/collagen-related signatures, the “metalloendopeptidase activity” signature (enrichment score = 0.59; q-value < 0.001) was among the top-enriched signatures and, accordingly, the pro-metastatic matrix metalloproteinases [29,30,31] (MMP-28 (avg_log2FC = 2.10; p-adj. < 0.001), MMP-9 (avg_log2FC = 2.01; p-adj. < 0.001), MMP-11 (avg_log2FC = 1.69; p-adj. < 0.001), MMP-14 (avg_log2FC = 1.68; p-adj. < 0.001), and MMP-2 (avg_log2FC = 1.64; p-adj. < 0.001) were identified as strongly upregulated genes. More importantly, the “platelet-derived growth factor binding” (enrichment score = 0.84; q-value < 0.001) signature showed the second highest enrichment score among all signatures. Further, the “insulin-like growth factor binding” (enrichment score = 0.67; q-value = 0.007) signature ranked among the top-enriched signatures within mCAFhighendotheliahigh tumor niches. Accordingly, platelet-derived growth factor receptor β (PDGFRβ; avg_log2FC = 2.07; p-adj. < 0.001) and PDGFRα (avg_log2FC = 1.67; p-adj. < 0.001) as well as insulin-like growth factor family member 1 (IGFL1; avg_log2FC = 1.84; p-adj. < 0.001) were strongly upregulated genes within mCAFhighendotheliahigh niches (Supplementary Table S1).
A higher frequency of mCAFs is an independent prognostic factor for recurrence and distant metastasis in SDC
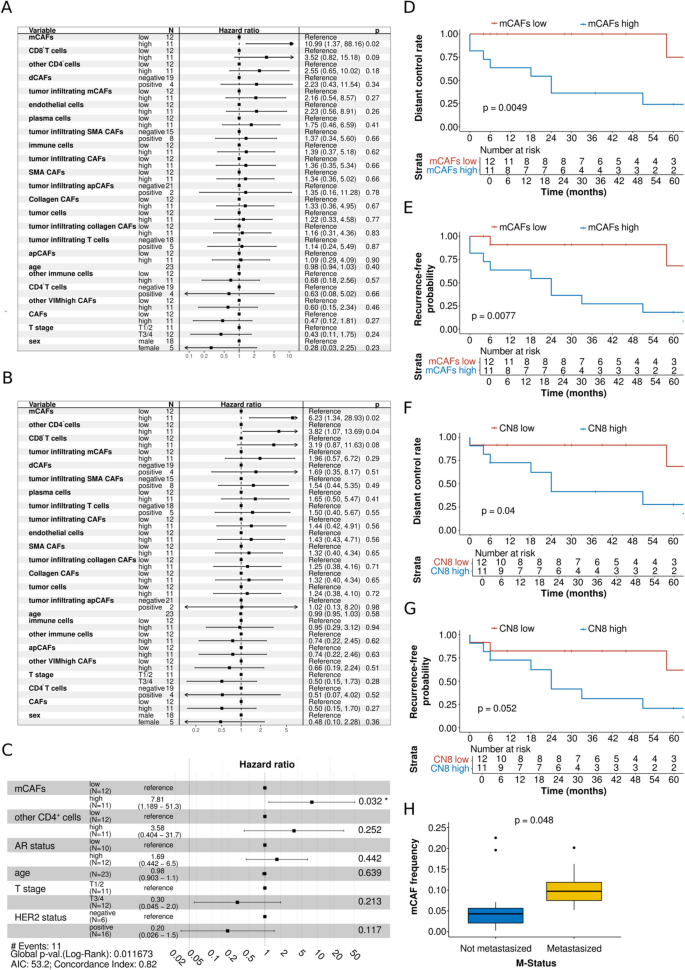
Cox regression analysis and log-rank test were performed to identify a potential influence of TME on the prognosis of SDC. The results of the univariate Cox regression model showed that a higher frequency of mCAFs was a prognostic factor for a higher rate of distant metastasis in SDC (p = 0.02; HR (95%CI) = 10.99 (1.37–88.16); Fig. 4A). Regarding RFP, a higher frequency of mCAFs (p = 0.02; HR (95%CI) = 6.23 (1.34–28.93)) and a higher frequency of other CD4+ cells (p = 0.04; HR (95%CI) = 3.82 (1.07–13.69)) were prognostic factors for a higher probability of recurrence in the univariate Cox regression model (Fig. 4B). Multivariate Cox regression revealed a higher frequency of mCAFs as an independent prognostic factor for a higher probability of recurrence (p = 0.032; HR (95%CI) = 7.81 (1.19–51.3); Fig. 4C). The five-year DCR was 75.0% for patients with a low frequency of mCAFs and 24.2% for those with a high frequency of mCAFs (p = 0.0049; Fig. 4D). The five-year RFP was 68.2% for patients with a low frequency and 18.2% for those with a high frequency of mCAFs (p = 0.0077; Fig. 4E). A high frequency of CN8 (mCAF-rich) was marginally non-significant as a prognostic factor for a higher probability of recurrence (p = 0.06; HR (95%CI) = 4.54 (0.94–22.01); Supplementary Fig. 4 A) and distant metastasis (p = 0.07; HR (95%CI) = 3.46 (0.91–13.10); Supplementary Fig. 4B) in the Cox regression model. Nevertheless, the five-year DCR was significantly lower in patients with a high frequency (27.7%) than in those with a low frequency of CN8 (68.2%; p = 0.04; Fig. 4F). Further, the five-year RFP was 20.4% for patients with a high frequency and 61.4% for those with a low frequency of CN8 (p = 0.052; Fig. 4G). The association between higher mCAF frequencies and a decreased DCR as well as RFP was consistent across AR subgroups (Supplementary Fig. 4 C and D). Finally, a significantly higher frequency of mCAFs was found in patients with distant metastatic disease than in those without (p = 0.048). Sex did neither show significance as prognostic factor for DCR (p = 0.23; HR (95%CI) = 0.28 (0.03–2.25), nor for RFP (p = 0.36; HR (95%CI) = 0.48 (0.10–2.28). When including survival data, a higher frequency of mCAFs was not a prognostic factor for OS (p = 0.90; HR (95%CI) = 1.10 (0.34–3.63) or RFS (p = 0.16; HR (95%CI) = 2.10 (0.74–5.91) in univariate cox regression. Furthermore, the five-year OS did not differ significantly between patients with a high frequency of mCAFs (45.5%) and those with a low mCAF frequency (58.3%; p = 0.87). There was no difference in the five-year RFS between patients with a high mCAF frequency (18.2%) and those with a low mCAF frequency (43.7%; p = 0.15). Notably, patients with low mCAF frequencies were markedly older (mean age = 69.17 years) than those with high mCAF frequencies (mean age = 63.64 years).
Fig. 4
Association of cell types with distant control rate (DCR), recurrence-free probability (RFP), and frequency of distant metastasis in salivary duct carcinoma (SDC) patients. A Univariate cox proportional hazards model for DCR for cell types and T stage, stratified by median proportion or as negative vs. positive in case median equals zero. N stage was excluded due to complete separation, resulting in an unbounded 95% confidence interval for its odds ratio. B Univariate cox proportional hazards model for RFP for cell types and T stage, stratified by median proportion or as negative vs. positive in case median equals zero. N stage was excluded due to complete separation, resulting in an unbounded 95% confidence interval for its odds ratio. C Multivariate cox proportional hazards model for RFP for mCAFs, AR status (ARhigh > 70% and ARlow ≤ 70 of tumor cells positive for AR), HER2 status, T stage, age, and other CD4+ cells. N stage was excluded due to complete separation, resulting in an unbounded 95% confidence interval for its odds ratio. D Kaplan–Meier plot with log-rank test for DCR comparing patients stratified as high and low based on the median proportion of mCAFs. E Kaplan–Meier plot with log-rank test for RFP comparing patients stratified as high and low based on the median proportion of mCAFs. F Kaplan–Meier plot with log-rank test for DCR comparing patients stratified as high and low based on the median proportion of CN8. G Kaplan–Meier plot with log-rank test for RFP comparing patients stratified as high and low based on the median proportion of CN8. H Boxplot displaying the proportion of mCAFs samples from patients with vs. without distant metastasis
When testing these results for validity within a previously published independent cohort with RNA-seq data from n = 67 SDC cases [23], we found that patients with low scores of the mCAF-like signature (mCAFhigh) had a significantly lower RFP (median RFP = 10.2 months; two-year survival = 23.5%) than mCAFlow patients (median RFP = 21.6 months; two-year-survival = 46.4%; p = 0.0294; Fig. 5G). Accordingly, mCAFhigh patients had a significantly lower RFS (median RFS = 10.2 months, two-year survival = 23.5%) than mCAFlow patients (median RFS = 21.6 months; two-year-survival = 46.4%; p = 0.049; Fig. 5H). RFS was also less favorable in mCAFhigh compared to mCAFlow patients when using mCAF-like signatures with different cut-offs (Supplementary Fig. 5 D-G).
Fig. 5
Validation analyses with RNA-seq and Spatial Transcriptomics (ST) data. A Spearman correlation of the mCAF-like module score with the pericytes and the B) endothelial module score, leveraging ST data of three SDC specimens. C Expression of metastasis-, IL-6- and VEGF-associated module scores in mCAFhighendotheliahigh ST-spots. IL-6- and VEGF-related signatures were not significantly enriched. D Differential expression analysis contrasting mCAFhighendotheliahigh ST-spots with all other ST-spots. The top10 overexpressed genes are highlighted. E Gene set enrichment analysis of DE-results depicted in C) using “Cellular Component” and (F) “Molecular Functions” GO terms. G and H) Kaplan–Meier plots and log-rank tests depicting the prognostic impact of the transcriptomic mCAF-like signature (top20% mCAF marker) after median dichotomization of 67 samples through estimation of the recurrence-free probability (G) and recurrence-free survival (H); LN = lymph node; met. = metastasis
No prognostic tests were performed for entities other than SDC because of the low absolute number of events within those entities.
Human classification, from celestial bodies to living organisms, often starts with their morphology. Depending on how something looks, it gets a certain label. This is all well and good until you find the exceptions, so you expand the category….
MENA-based production companies Front Row Filmed Entertainment and Dubai Bling producers Different Productions are teaming up with regional celebrity Nour Arida and independent creative agency Read the Room, to produce Confidence is Queen.
The new Tilta Extended Pro Monitor Mount adds a double-hinged swivel arm for fast height changes, tool-free tension control, and SmallHD-compatible locating pins, all in a compact NATO-based design. It is available for pre-order now at $53,…
A milestone has been reached in the search for planets beyond our solar system. The European Space Agency’s (ESA) Plato spacecraft has officially completed construction, with the final…
As there are few studies describing mental health in separate groups of sexual and gender minorities, and as there is much less knowledge about this in adolescent populations, we wanted to estimate prevalences in data from a longitudinal…
RECENT evidence has revealed a complex and time-dependent association between traumatic brain injury (TBI) and risk of amyotrophic lateral sclerosis (ALS), according to a large UK cohort study. Individuals with documented TBI showed a higher…