ISLAMABAD, Oct. 22 (Xinhua) — Two policemen were killed when unidentified militants opened fire at them in Pakistan’s southwestern Balochistan province on Wednesday, police said.
The incident occurred in Noshki district, where unidentified…
ISLAMABAD, Oct. 22 (Xinhua) — Two policemen were killed when unidentified militants opened fire at them in Pakistan’s southwestern Balochistan province on Wednesday, police said.
The incident occurred in Noshki district, where unidentified…

After a huge race weekend in Austin, another one awaits as the teams make the relatively short trip south to Mexico City. With 40 points covering the top three drivers in the championship and plenty of young drivers set to get track time, it’s…

A White House official has said there is “zero truth” to a report that Donald Trump is considering commuting Sean “Diddy” Combs’s prison sentence as early as this week.
On Monday, US entertainment site TMZ reported the US president…

MICHELIN Stars are awarded to restaurants offering outstanding cooking, taking into account five universal criteria: the quality of the ingredients; the harmony of flavours; the mastery of techniques; the personality of the chef as…

Scientists have uncovered a “hidden order” in drylands across the planet, where plants follow disordered hyperuniformity — a layout that looks random and disorganized up close but adheres to a clear pattern when viewed from farther away.
The…

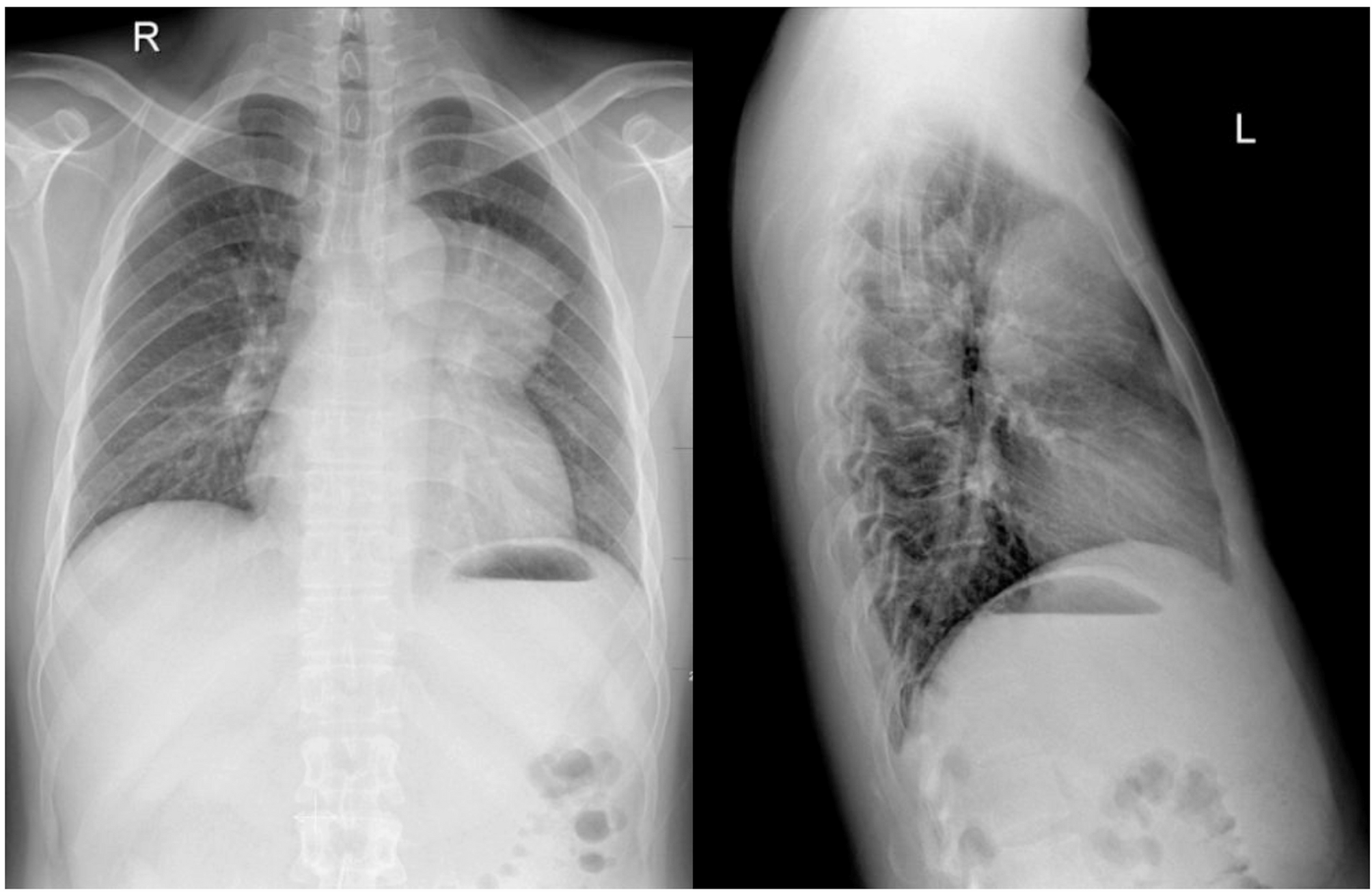
A 28-year-old man presented with spasmodic cough lasting for more than 1 month. Physical examination was normal. The chest radiography demonstrated a large, mass-like opacity located at the left side of the upper mediastinum(‘. 1). A…

We report a case of a 29-year-old Han male patient. On 17 October 2024, he presented to the First Affiliated Hospital of Anhui Medical University with complaints of fatigue and palpitations for 2 weeks. A complete…
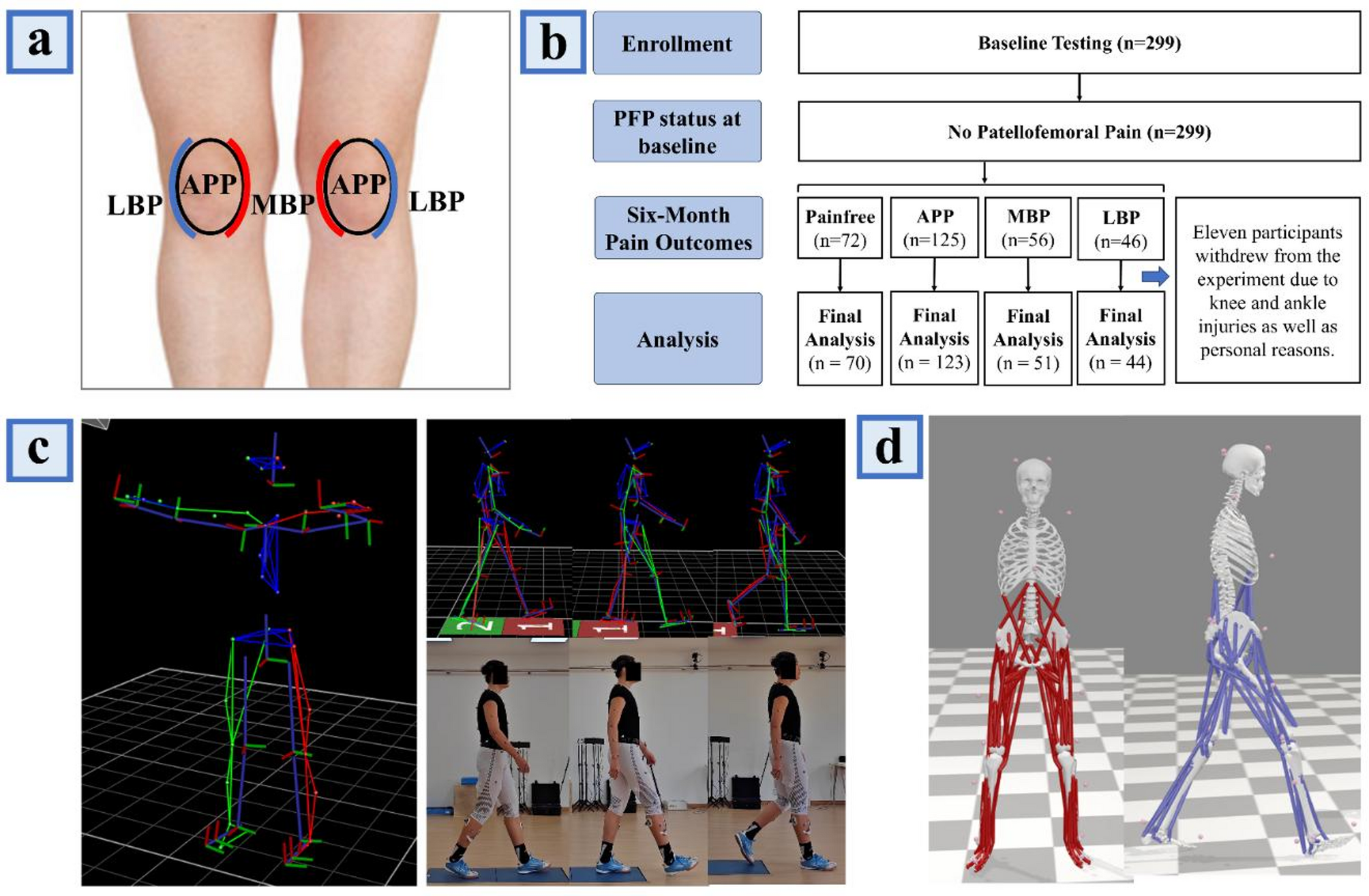
In this study, we developed and evaluated an artificial intelligence (machine learning) model to elucidate the muscle force-production characteristics associated with the recurrence of pain in the APP, MBP, and LBP regions. The findings support our hypothesis, indicating that the muscle force–related factors underlying PFP recurrence differ across anatomical regions. Among the three machine learning classifiers employed, the XGBoost model exhibited the highest accuracy, with predictive performance ranging from 95.9% to 98.3% in forecasting pain across these regions. Consequently, SHAP values were computed based on the XGBoost model to visually represent the importance of each feature, thereby delineating the key muscle force patterns that precipitate PFP in distinct regions.
In addressing overfitting, it is noteworthy that XGBoost incorporates embedded regularization during training, specifically the L1 (lambda) and L2 (alpha) penalties, which effectively constrain model complexity and reduce the likelihood of overfitting to the training set [36]. In addition, we employed five-fold cross-validation within the training data to optimize hyperparameters, thereby avoiding the inappropriate use of the test set for model tuning and further mitigating the risk of overfitting. Nevertheless, given that the AUC achieved by the XGBoost models in this study was relatively high (>0.99), it remains possible that some degree of uncontrollable overfitting occurred. This observation highlights the need for future research to expand both sample size and feature dimensionality, as well as to improve group balance during testing, in order to further safeguard against overfitting.
Insufficient strength in the gracilis, tibialis anterior, and internal oblique muscles, combined with excessive strength in the adductor longus and tensor fascia latae, constitutes the principal precipitating factors for pain in the APP region. Although both the gracilis and adductor longus are located on the medial thigh, their distinct insertion sites result in different contributions to joint kinematics [37, 38]. Specifically, the gracilis inserts on the medial aspect of the proximal tibia, facilitating hip internal rotation, whereas the adductor longus terminates at the linea aspera of the femur and functions to externally rotate the hip [37, 38]. Consequently, insufficient strength of the gracilis, combined with excessive strength of the adductor longus, may result in exaggerated hip external rotation during gait. Cadaveric studies have demonstrated that a hip external rotation of 30° can significantly increase patellofemoral joint contact forces [39]. During ambulation, the contact force generated by hip external rotation is continuously loaded onto the anterior aspect of the patella, peaking at knee flexion angles between 30° and 60°. Over time, this repetitive loading may precipitate the recurrence of pain in the APP region [39]. It is noteworthy that recent studies suggest potential differences in neural innervation and functional roles between the proximal and distal regions of the same muscle [40]. For the gracilis, the proximal fibers, originating from the medial aspect of the ischiopubic ramus, may primarily contribute to hip joint motion. In contrast, the distal fibers extend across the knee joint, where they merge with the tendons of the sartorius and semitendinosus to form the pes anserinus, inserting onto the superior medial tibia [41]. This anatomical arrangement suggests that the distal fibers may be more directly involved in knee movement and tibial internal rotation. Considering that current evidence generally supports the association between gracilis insufficiency and the recurrence of PFP, primarily through alterations in hip joint mechanics as previously discussed [37,38,39], clinical practice should place particular emphasis on targeted activation and rehabilitation of the proximal gracilis. Such interventions may help prevent recurrent pain in the APP region.
Our findings indicate that insufficient tibialis anterior strength is a primary precipitant of pain in the APP region. Notably, previous cohort studies have not clearly delineated the relationship between tibialis anterior strength and PFP. The present study’s ability to capture this association may be attributable to the employment of a machine learning model, which can discern more subtle inter-variable relationships that may be pivotal for PFP prevention. Inadequate tibialis anterior strength disrupts the balance between plantarflexor and dorsiflexor forces at the ankle, thereby impairing sagittal plane stability [42]. As a consequence, the ankle’s capacity for sagittal attenuation is markedly diminished, allowing unbuffered ground reaction forces to be transmitted proximally to the knee and patellofemoral joints, which leads to excessive localized loading on the patellar surface and ultimately precipitates APP pain [43]. Furthermore, the machine learning model revealed that diminished internal oblique strength is associated with APP pain, corroborating findings from previous cross-sectional studies [44]. Insufficient internal oblique strength increases trunk inclination and rotation during ambulation. In particular, when the internal oblique of the contralateral side is weak, the trunk tends to rotate and tilt toward the affected side. Given that the trunk accounts for over 50% of body weight, such a shift in mass distribution results in an increased overall load on the affected limb, thereby elevating patellofemoral joint stress [44]. This heightened joint stress exacerbates anterior patellar wear during knee flexion-extension cycles, ultimately culminating in APP pain [45].
Excessive strength in the tensor fascia latae is also a major predictor of APP region pain. Previous studies have further reported that such overexertion of the tensor fasciae latae can induce hip flexion [46]. However, during gait, excessive hip flexion results in forward tilting of the trunk, thereby shifting the center of mass anteriorly and increasing the load on the anterior aspect of the knee, ultimately precipitating recurrent APP pain [47]. Moreover, excessive force of the tensor fasciae latae may disrupt the strength balance between the hip flexors and extensors [48], thereby undermining sagittal-plane core stability and consequently amplifying anterior–posterior displacement of the center of mass [49]. In response, the lower limb joints often adopt a “stiff” movement pattern to stabilize the center of mass and prevent falls. Nevertheless, in such a “stiff” gait pattern, energy absorption by tissues distal to the knee may be reduced, thereby increasing the mechanical load on the knee joint. This load may be repeatedly transmitted to the anterior patellar region, ultimately resulting in patellar cartilage damage and the recurrence of APP [47].
The machine learning model identified that excessive strength in the rectus femoris, gracilis, gluteus maximus, and adductor longus muscles, coupled with insufficient strength in the semitendinosus, constitutes the primary mechanism underlying MBP region pain. Notably, the rectus femoris serves as a knee extensor, whereas the semitendinosus—being part of the hamstring group—functions as a knee flexor. Excessive rectus femoris force, combined with insufficient semitendinosus strength, may lead to an increased knee extension moment during gait. Prior investigations have demonstrated that when the knee extension moment reaches 240 Nm, the patellofemoral joint stress escalates by 3.9 MPa [50]. Furthermore, inadequate semitendinosus strength may compromise the dynamic control of the knee’s frontal plane, resulting in augmented lateral displacement of the patella, exacerbation of medial patellar wear, and ultimately the manifestation of MBP region pain in patients with PFP [51]. Recent studies have reported that the proximal and distal compartments of the semitendinosus exhibit distinct discharge rates and differences in the variability of neural drive [40]. It is speculated that the region of the semitendinosus located closer to the knee joint may be more directly involved in knee and patellofemoral joint loading and movement, and thus more strongly associated with the recurrence of MBP. Consequently, targeted stimulation and rehabilitation of this knee-adjacent region of the semitendinosus during clinical training may yield greater therapeutic benefits and improve the effectiveness of preventing MBP recurrence. However, this assumption remains speculative and requires confirmation through future cohort studies.
During ambulation, excessive force generated by the gracilis and adductor longus muscles is a key precipitant of MBP region pain. In addition to mediating hip internal and external rotation, both muscles are part of the hip adductor group; their combined force production may lead to pronounced hip adduction [52]. Studies by McKenzie et al. [53] and Willson et al. [54] have shown that patients with PFP exhibit significantly greater hip adduction during functional activities—such as running, jump landing, and squatting—compared with healthy controls, thereby further validating these findings. Ultrasonographic data indicate that when hip adduction reaches 20°, lateral displacement of the patella increases by approximately 7.3 mm [55]. Repeated lateral displacement may exacerbate friction at the medial femoral condyle and medial patellar region, ultimately precipitating pain in the MBP region [55].
Results from the machine learning model indicate that excessive gluteus maximus strength is one of the contributing factors to pain in the MBP region. Previous studies have demonstrated that excessive force production by the gluteus maximus during gait leads to heightened frontal-plane stiffness at the hip joint [56]. Given that the hip and knee joints serve as the primary sites for frontal-plane energy absorption during ground contact—accounting for 59.1% and 38.5% of energy absorption, respectively [57]—excessive hip stiffness markedly reduces its capacity to absorb energy. Consequently, unbuffered ground reaction forces are transferred to the knee joint [57], increasing the frontal-plane load and elevating medial patellar pressure [57]. Moreover, excessive force production by the gluteus maximus during gait may promote an overly upright trunk posture, thereby elevating the center of mass and increasing lateral trunk sway. The lateral forces generated by this trunk movement are repeatedly imposed on the knee joint, which is already burdened by high energy absorption demands [58], ultimately leading to repeated compression of the medial patellar margin and significant pain over time.
Our explainable machine learning model revealed that insufficient strength in the rectus femoris, tensor fascia latae, and gluteus maximus, coupled with excessive force generated by the adductor longus and gracilis, constitutes the primary mechanism underlying pain in the LBP region. Among these, the rectus femoris—an integral component of the quadriceps—primarily generates the knee extension moment during gait [59]. Powers et al. [60] reported that PFP patients exhibit a knee extension moment of 23.6 N·cm/kg, compared to 30.4 N·cm/kg in healthy individuals; the inability of the rectus femoris to produce an adequate extension moment may therefore serve as a precipitating factor for PFP. Moreover, the quadriceps play a critical role in controlling patellar tracking during knee flexion-extension. Weakness in this muscle group can result in aberrant patellar kinematics, including increased frontal plane displacement of the patella and consequent excessive compression of its lateral edge, ultimately leading to pain [59]. It should be noted that previous studies have reported regional heterogeneity in the activation of the rectus femoris under different contraction tasks. Specifically, hip flexion predominantly activates the proximal region of the muscle, whereas knee extension primarily recruits its central and distal regions [61]. This task-dependent distribution is thought to arise from the relatively segregated organization of motor neuron pools within the spinal cord, where neurons innervating the proximal region are mainly located in the rostral part of the motor nucleus, while those serving the distal region are positioned more caudally [61]. Such topographical differentiation provides a mechanistic explanation for the distinct activation patterns of the proximal versus distal regions of the rectus femoris [61]. In the context of the present study, the distal region may be a critical contributor to LBP-related pain, as it is more directly associated with knee and patellofemoral joint function, suggesting that this region should receive particular attention during clinical interventions [61]. However, we did not directly examine the relationship between regional rectus femoris activation and LBP pain in this study. Accordingly, this interpretation remains speculative and requires systematic investigation in future research.
Based on our findings, insufficient gluteus maximus strength predisposes individuals to LBP region pain. The gluteus maximus not only facilitates hip extension but also functions as a hip external rotator; when its strength is diminished, the hip and femur tend to exhibit excessive internal rotation. Powers et al. [62] demonstrated via magnetic resonance imaging that an 8° increase in femoral internal rotation can induce a 13° patellar external rotation, during which the lateral edge of the patella is repeatedly subjected to friction and compressive forces against the lateral femoral condyle. Moreover, owing to the inherent anatomy of the patellofemoral joint, the lateral force on the patella during gait (0.54 BW) far exceeds that on the medial side (0.15 BW) [63]. Collectively, this loading environment markedly increases the risk of LBP region pain. Furthermore, our machine learning results indicate that insufficient tensor fascia latae strength, combined with excessive force generated by the adductor longus and gracilis, further predisposes to LBP region pain. The tensor fascia latae, a principal component of the hip abductor group [64], contrasts with the adductor longus and gracilis, which are key elements of the hip adductor group. Reduced strength of the tensor fascia latae, combined with excessive force production by the adductor longus and gracilis, leads to pronounced hip adduction during ambulation [52, 65]. Ultrasonographic evidence indicates that, compared with a neutral position, 20° of hip adduction results in a 0.24-cm increase in lateral patellar displacement. Repeated lateral displacement of the patella may exacerbate wear and local compressive loading on its lateral margin, ultimately precipitating LBP region pain [66].
Targeted neuromuscular training may alleviate regional PFP by correcting specific deficits in force-generation patterns. For the prevention of APP region pain, it is imperative to enhance the strength of the hip internal rotator group to counteract the excessive force generated by the adductor longus, which predisposes the hip to external rotation. In addition, incorporating resistance exercises for the tibialis anterior, alongside relaxation protocols for the tensor fascia latae to prevent its overcontraction during the stance phase, is recommended. Furthermore, targeted training of the contralateral internal oblique may help correct trunk lean during gait, thereby reducing unilateral knee loading.
In the context of MBP region pain, emphasis should be placed on augmenting hamstring strength to restore a balanced knee flexion–extension moment and improve knee joint stability. Concurrently, targeted strengthening of the hip abductor group is recommended to counteract the aberrant force production by the gracilis and adductor longus during gait. Furthermore, relaxation training for the gluteus maximus may increase the hip joint’s frontal-plane mobility and its capacity for energy absorption, thereby reducing the overall load on the knee joint.
For LBP region pain, priority should be given to reinforcing the rectus femoris and gluteus maximus. Concurrently, targeted strengthening of the hip abductor group (e.g., tensor fascia latae) should be implemented, while relaxation training for the hip adductor group (e.g., adductor longus and gracilis) is recommended to correct imbalances between hip adduction and abduction. This integrated approach is expected to enhance proximal joint stability and ultimately reduce lateral displacement and loading of the patellofemoral joint.
It should be emphasized that although the SHAP dependence plots identified apparent “thresholds” for these risk factors, these values do not represent clinically meaningful cut-off points. Rather, they indicate the points at which the relationship between a given feature and the risk of PFP recurrence begins to change within the model. Accordingly, these thresholds cannot be directly applied in clinical practice and should instead be viewed as preliminary reference values that require further verification and refinement through systematic clinical studies.
Looking ahead, our model could be integrated into clinical decision-support tools, such as OpenSim-based musculoskeletal modeling platforms or gait analysis systems, to enable direct identification of region-specific risks of PFP recurrence and the muscle strength deficits most in need of improvement. Such integration would not only facilitate the development of individualized intervention strategies but also provide more robust evidence to inform clinical decision making. Furthermore, review studies have indicated that different regions within the same muscle exhibit distinct levels of focal adhesion kinase (FAK) phosphorylation during eccentric and concentric training [67]. For instance, following eccentric training of the vastus lateralis, pY397-FAK levels in the distal region were approximately four times higher than those observed after concentric training, contributing to distal hypertrophy of the quadriceps [67]. Given that different training modalities induce region-specific muscle hypertrophy, future strength interventions for patients with PFP should first identify the specific muscle regions implicated in the condition and then select training strategies that effectively target these regions. This study provides only a preliminary intervention framework by treating the muscle as a single functional unit. Future research should build on these findings to investigate more refined, region-specific approaches.
Although this study provides preliminary evidence of distinct muscle force strategies associated with PFP across different anatomical regions, several limitations should be acknowledged. First, although SHAP was used to preliminarily identify the points at which the relationship between muscle strength features and the risk of PFP recurrence begins to shift within the machine-learning model, their generalizability may be limited by individual variability and environmental context. To translate these thresholds into clinical practice, further clinical studies are needed for validation and refinement. Furthermore, although a six-month follow-up in a cohort of 299 participants yielded important initial findings, a longer observation window and a larger, more heterogeneous sample would likely offer a more comprehensive understanding of the temporal dynamics and recurrence patterns of PFP. Finally, recent studies have suggested that neural innervation and activation levels may vary across different regions (proximal versus distal) of the same muscle [40]. In the present study, however, the OpenSim modeling approach treated each muscle as a single unit, which made it difficult to examine how region-specific muscle activation might be related to the recurrence of PFP. This limitation underscores the need for future cohort studies to further investigate these region-dependent mechanisms underlying PFP recurrence. Finally, recent studies have demonstrated that neural innervation and activation levels can differ across distinct regions of the same muscle, such as proximal versus distal segments [40, 61]. This phenomenon is likely attributable to the differential spatial organization of motor neurons within the spinal cord that control the proximal and distal portions of the muscle [61]. However, in the present study, the OpenSim modeling approach treated each muscle as a single unit, limiting our ability to investigate the relationship between region-specific muscle activation and PFP recurrence. This limitation underscores the need for future cohort studies to examine the region-dependent mechanisms underlying PFP recurrence. In addition, evidence from training studies indicates that different muscle regions exhibit distinct molecular responses during concentric and eccentric exercises, which can lead to region-specific hypertrophy [67]. Because the present study considered muscles as whole units, it provides limited guidance for interventions targeting specific muscle regions, representing a key limitation of this work.