Blog
-
Just a moment…
Just a moment… This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!
Continue Reading
-
Genome-wide phylogeny reshapes our understanding of the evolution of deep-sea dragonfishes, bristlemouths, viperfishes, and allies (Stomiiformes) | BMC Ecology and Evolution
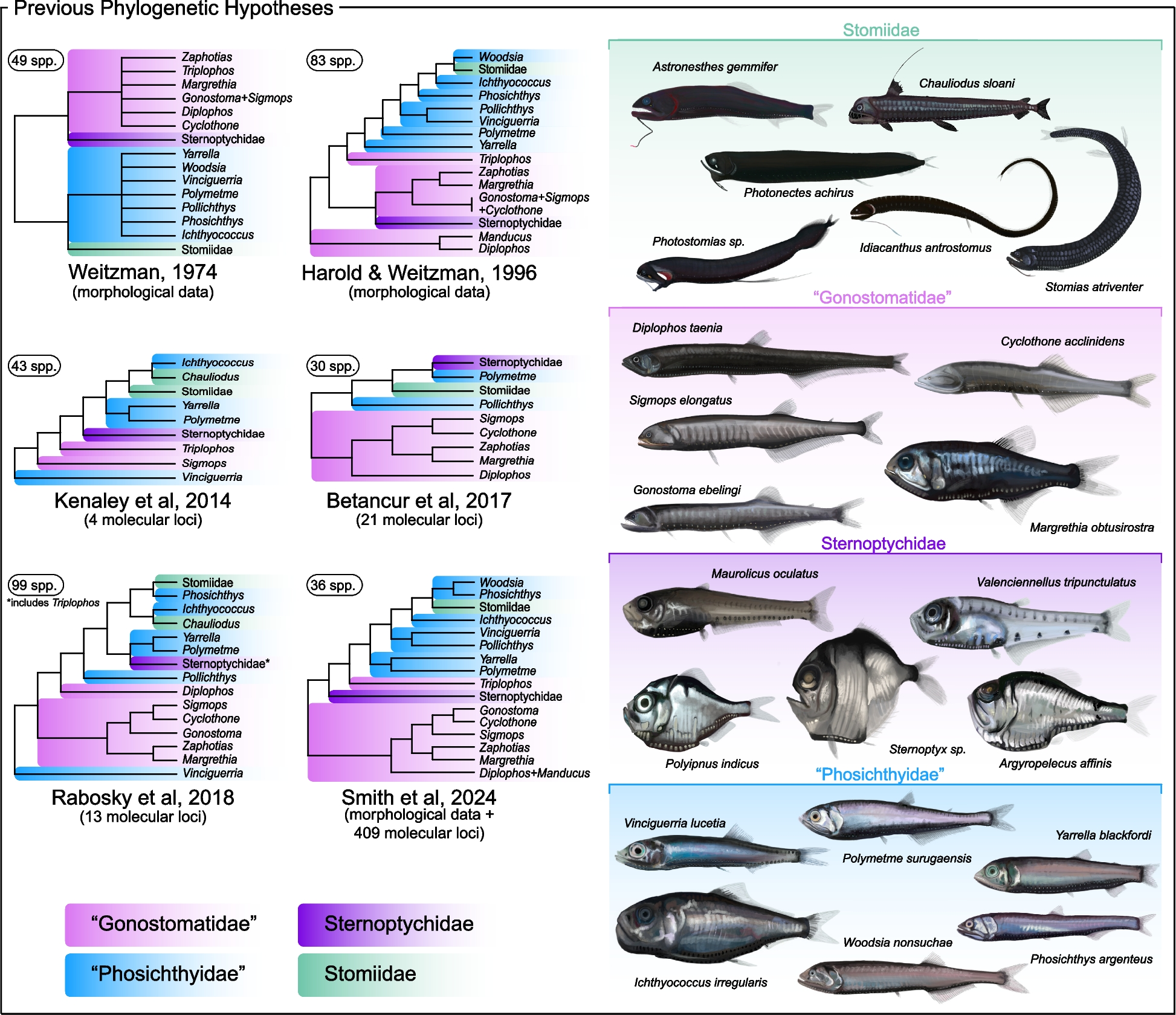
Phylogenomic analyses reveal novel deep-sea fish relationships
Our primary nuclear exon-based phylogenomic dataset included 60 stomiiform species [31 genera, 4 families] and four outgroup taxa, comprising 936 loci totaling 314,607 base pairs (bp),…
Continue Reading
-
Clinical features of MPP with or without viruses among hospitalized children in 2023, Wenzhou, Zhejiang, China | Italian Journal of Pediatrics
Study population
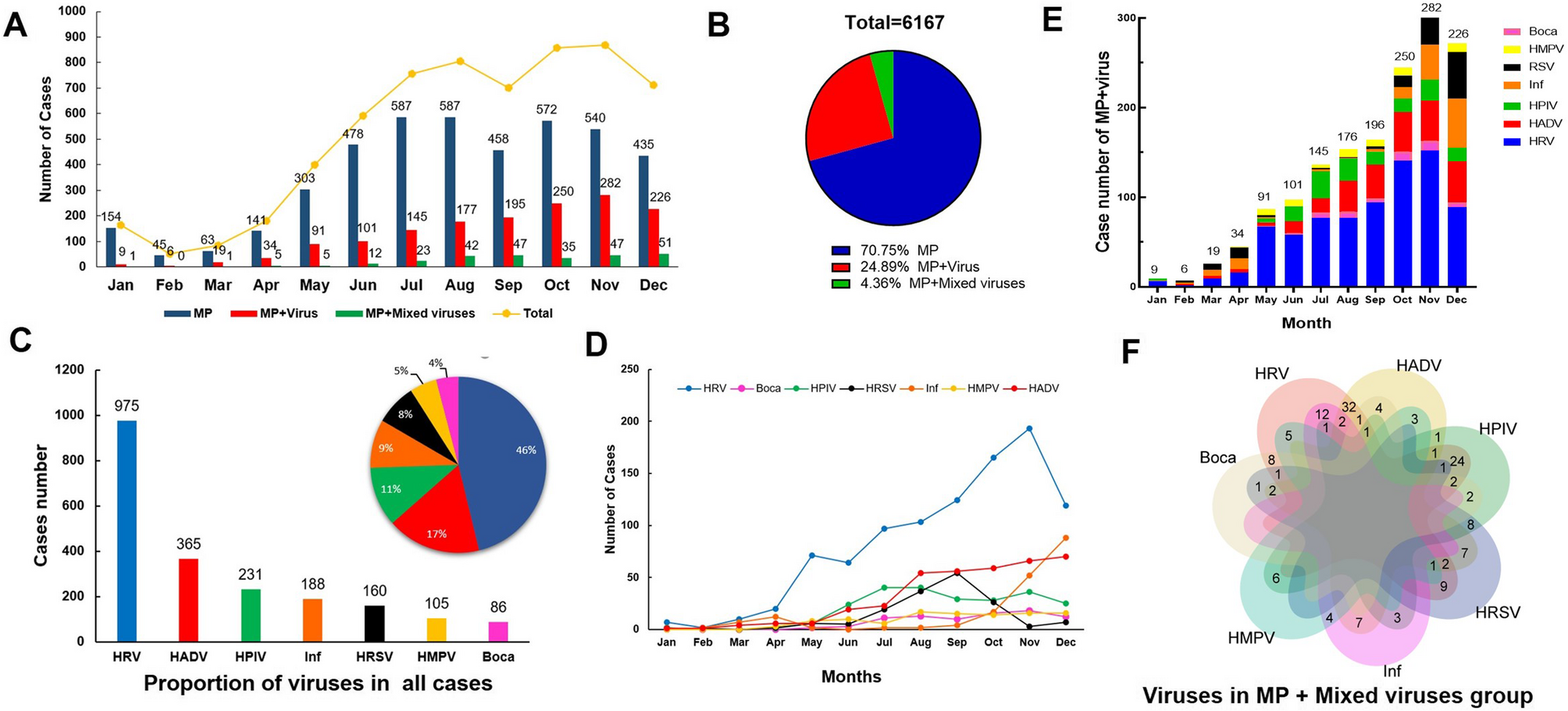
During the study period from Jan, 2023 to Dec, 2023, a total of 14,907 patients with CAP were initially included in this study, following the exclusion criteria, 6,167 pediatric patients were ultimately enrolled. Of these, 4347…
Continue Reading
-
Danon disease in male patients: a prospective natural history study to augment understanding of the phenotype | Orphanet Journal of Rare Diseases
Visit completion rates
Nine male patients were enrolled during January 2019 to September 2019. Due to the COVID-19 pandemic, study participation was incomplete. Pre-COVID pandemic onset (March 2020), 80.1% of the expected 171 visits were attended (including baseline visits). Post-COVID pandemic, 19.7% of the 458 scheduled visits were attended. The cognitive assessments DAS-II and VABS-3 were performed at baseline only. All other assessments had follow-up visits completed at varying time points (Supplementary Table 1).
Study population and genetic analysis results
We included eight pediatric males and one adult male from the USA, comprising eight families. The characteristics of the study population are summarized in Table 1. Nonsense mutations occurred in six patients (66%) and three patients (33%) had deletions (Table 2).
Table 1 Characteristics of the study cohort, n = 9 Table 2 Genetic screening results for the nine patients Patient reported outcome measures
PCQLI
Patient responses
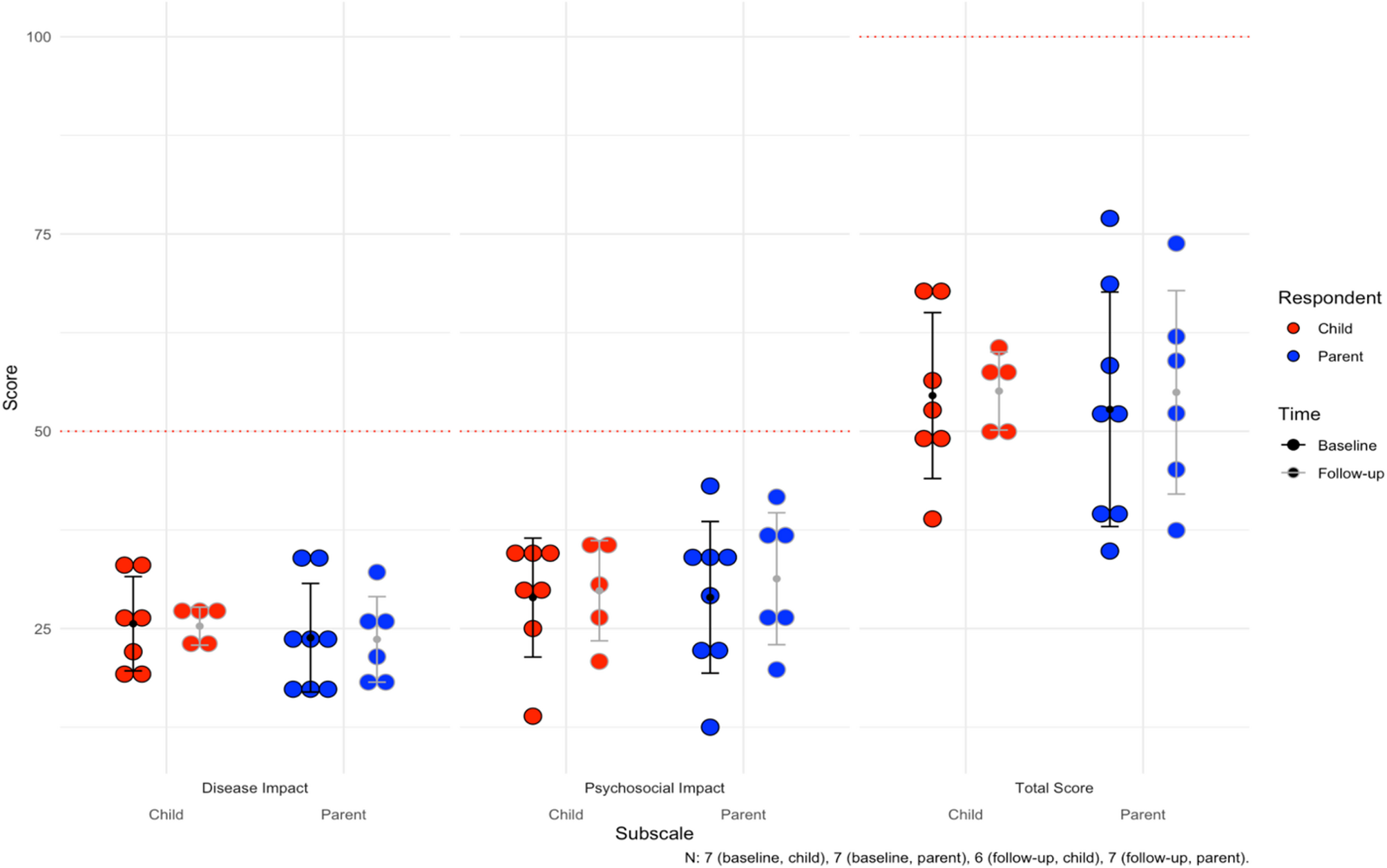
Seven of eight pediatric patients had baseline PCQLI responses (88%, n = 7), of which seven had follow-up responses (100%, n = 7). The baseline mean for the Disease Impact subscale was 25.6 ± 6.0. The mean follow-up time was 26.6 months for both patient and parent responses (see all responses in Supplementary Table 2). At last follow up, four patients (57%, n = 4) reported lower Disease Impact scores. For the Psychosocial Impact Score, the mean at baseline was 28.9 ± 7.5. At last follow-up, three patients (43%, n = 3) reported lower scores. For the Total Score, the mean was 54.5 ± 10.5 at baseline. At last follow-up, four patients (57%, n = 4) reported lower total scores.
Parent responses
For the parents, there were eight baseline responses (100%, n = 8), of which seven had follow-up responses (88%, n = 7). Mean follow-up time was 26.6 months. The baseline mean for Disease Impact was 23.8 ± 6.9, with three parents (43%, n = 3) reporting lower scores for their children at last follow up. Mean Psychosocial Impact score at baseline was 28.9 ± 9.6, with five parents (71%, n = 5) reporting lower scores at last follow-up. Finally, the mean Total Score was 52.8 ± 14.9 at baseline, and four parents (57%, n = 4) reported lower total scores for their children at last follow up. The mean scores can be visualized for children and parents in Fig. 1. Notably, average difference between patient and parent Total Scores were 9.1 ± 7.9 and concordance in longitudinal improvements or worsening of scores over time between patients and parents was 75% (n = 9).
Fig. 1 Average subscale and total scores for the Pediatric Cardiac Quality of Life Inventory (PCQLI) across the cohort. For Disease Impact and Psychosocial Impact subscales, 50 is the maximum score (100 for Total Score). The mean follow-up time is 26.6 months. The error bars are the mean and standard deviations for each subgroup
PQLQ
The average scores for the subscales of the PQLQ can be found in Table 3 (see all responses in Supplementary Table 3). Both patients and their parents responded to this. The max score for all subscales was 100. The mean follow-up time was 28.3 months. Figure 2 shows the scores for physical, emotional, social, and school functioning.
Table 3 Average subscale and total scores for the pediatric quality of life questionnaire Fig. 2 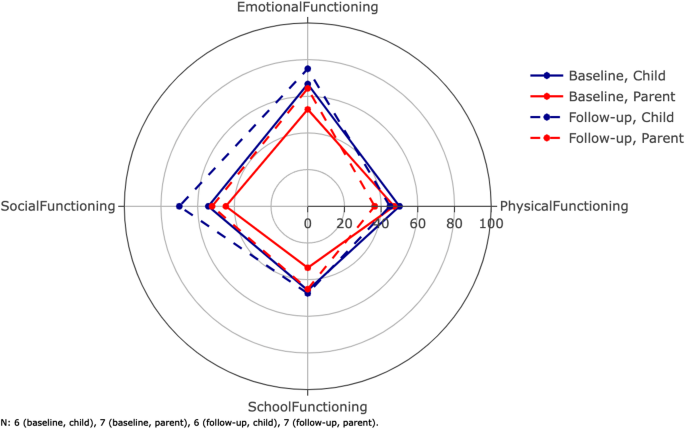
Average scores for the dimensions of the Pediatric Quality of Life Questionnaire (PQLQ). The inventory is filled out by both patients and parents. The parents score their children as functioning worse than the patients personally score themselves. The composite scores total scores are not shown on this radar plot (Table 3). Error bars are not included here in order to maintain visibility. The mean follow-up time was 28.3 months
Patient responses
Six of eight pediatric patients had baseline responses (75%, n = 6), of which five patients had follow-up responses (83%, n = 5). For the physical health summary score, which is equal to the physical functioning score, the baseline mean was 50.0 ± 6.3; two patients (40%, n = 2) reported lower physical health summary scores at follow-up. For the psychosocial health summary score, the baseline mean was 55.3 ± 24.7; one patient (17%, n = 1) reported a lower psychosocial health summary score for themselves at follow-up. For emotional functioning, baseline mean was 66.7 ± 24.8, and two patients (40%, n = 2) reported worse functioning at follow-up (Fig. 2). For social functioning, baseline mean was 54.2 ± 32.9, and four patients (60%, n = 3) reported worse functioning at follow-up. For school functioning, baseline mean was 45.8 ± 30.1, and four patients (60%, n = 3) reported worse functioning at follow-up. Finally, for the total score, baseline mean was 53.4 ± 17.6, and one patient (20%, n = 1) reported a lower total score at follow-up.
Parent responses
Seven parents had baseline responses (88%, n = 7), of which six had follow-up responses (86%, n = 6) (Table 3). For the physical health summary score, the mean at baseline was 47.1 ± 8.4. At follow-up, all parents (100%, n = 7) reported worse functioning in their child. For the psychosocial health summary score, the baseline mean was 43.7 ± 16.0 and only one parent (17%, n = 1) reported a lower follow-up psychosocial health summary score. For emotional functioning, baseline mean was 52.9 ± 30.4, and four parents (67%, n = 4) reported worse functioning at follow-up. For social functioning, baseline mean was 44.6 ± 13.7, and four parents (67%, n = 4) reported worse functioning at follow-up. For school functioning, baseline mean was 33.6 ± 9.4, and three patients (50%, n = 3) reported worse functioning at follow-up. Finally, for the total score, baseline mean was 44.9 ± 8.6, and four parents (67%, n = 4) reported lower total scores at follow-up. Average difference between patient and parent total scores was 13.4 ± 9.1. Additionally, concordance in longitudinal changes in patient and parent total scores was 58% (n = 5). Parents were more likely to describe physical decline at follow up compared to the patients themselves. Although the remaining emotional, social and school functioning dimensions were more concordant between parents and patients, the total PQLQ parent scores were still lower at follow up compared to patients.
Cognitive and neuropsychological assessment
In our cohort, all patients (100%, n = 9) were affected by neuropsychological symptoms that included: learning difficulties (100%, n = 9), attention-deficit hyperactivity disorder (56%, n = 5), anxiety (44%, n = 4), depression (44%, n = 4), autism (22%, n = 2) and global developmental delay (11%, n = 1).
DAS-II
Six patients in the cohort completed the DAS-II at baseline. Figure 3a shows the average score for our cohort in each of the domains (see the scores for each domain for each patient in Supplementary Table 4). The mean at baseline for each domain in our cohort was: GCA, 67.0 ± 14.7; verbal, 66.3 ± 19.0; nonverbal, 70.5 ± 18.3; spatial, 68.7 ± 18.3.
Fig. 3 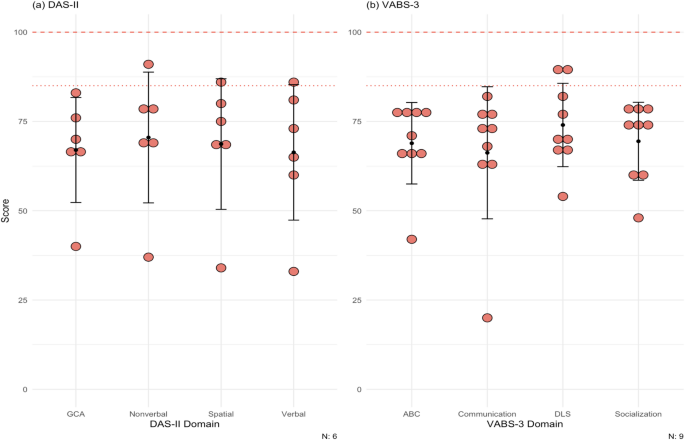
(a) Scores for patients for the DAS-II. Population mean and standard deviation for the domains tested are 100 (dashed line) ± 15 (dotted line). Patient 6, 8, 9 did not complete the DAS-II. Most DD patients lie below at least 1 standard deviation on both cognitive tests. (b) Scores for patients for the VABS-3. Population means and standard deviations for the domains tested are 100 (dashed line) ± 15 (dotted line). All patients completed this test at baseline only. The maximum score of the test is 170. Most of the patients scored below at least 1 standard deviation on all domains. DAS-II = Differential Ability Scales Second Edition, VABS-3 = Vineland Adaptive Behavior Scales Third Edition, GCA = General Conceptual Ability, ABC = Adaptive Behavior Composite, DLS = daily living skills
VABS-3
All patients completed the VABS-3 at baseline. The mean at baseline for each domain in our cohort was: ABC, 68.9 ± 11.4; communication, 66.2 ± 18.5; daily living skills 74.0 ± 11.7; socialization, 69.4 ± 10.9 (Fig. 3b; see the scores for each domain for each patient in Supplementary Table 5).
Ophthalmological assessment
DD patients very commonly have visual disturbances. In our cohort, eight patients had one or more ophthalmological changes (89%, n = 8): nyctalopia (11%, n = 1), photophobia (11%, n = 1), blurry vision (33%, n = 3), myopia (78%, n = 7), prescribed corrective lenses (78%, n = 7), and photophobia (89%, n = 8). The BCVA was within the normal range for all patients (100%, n = 9). Of note, hyperreflective foci were identified at the level of the outer nuclear layer (ONL) and the border of the outer plexiform layer in six patients (67%, n = 6) in SD-OCT (example in Fig. 4). These patients also had paler fundus pseudocolor images with what appeared to be a loss of retinal pigmentation. Fundus autofluorescence imaging demonstrated increased macular autofluorescence.
Fig. 4 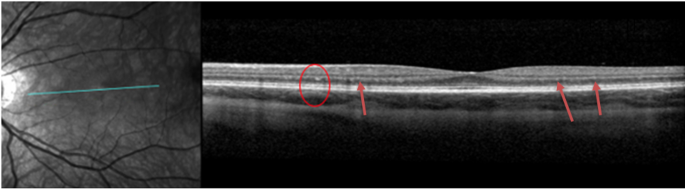
Spectral Domain Optical Coherence Tomography (SD-OCT) of the left eye of patient 5 showing hyper-reflective foci on the border of the outer nuclear layer (ONL) foci and outer plexiform layer (OPL) (red circle and red arrows)
Cardiopulmonary assessment
Most patients in the cohort reported cardiac related symptoms (78%, n = 7): dyspnea (33%, n = 3), palpitations (44%, n = 4), and chest pain (56%, n = 5). All nine patients had baseline echocardiograms (100%, n = 9) and seven patients had follow-up echocardiograms (78%, n = 7). Regarding outcomes, one patient underwent transplantation during the study period at age 14. There were no deaths or ventricular assist device implantations. Two pediatric patients had baseline data only; one patient underwent cardiac transplantation and another patient stopped following up due to the COVID pandemic. Due to standardized z-score reporting in pediatric patients, we separated the pediatric patients (n = 8) from the adult patient (n = 1). The mean follow-up time was 24.5 months for the pediatric patients. Mean EF at baseline was 68.9 ± 4.8%. After the mean follow-up time, all six pediatric patients with follow-ups had lower EF values (100%, n = 6). The mean EF at last follow-up was 64.3 ± 8.5%, with an average paired difference of -5.9% which based on the Wilcoxon signed-rank test, was not statistically significant. The adult patient had a baseline EF of 47% and at last follow-up 41%.
For wall thickness, we utilized a maximum wall thickness (MWT) that measured the largest of the septal or posterior wall. The average MWT at baseline for the pediatric patients was 13.6 ± 7.1 mm (z-score = 6.9 ± 6.2; 75% [n = 6] of pediatric patients had a z-score > 2 at baseline). At last follow-up, wall thickness increased in all six pediatric patients (100%, n = 6). The mean MWT at last follow-up was 15.6 ± 6.8 mm (z-score = 9.4 ± 7.6), with an average paired difference of 3.8 mm, which based on the Wilcoxon signed-rank test, was not statistically signfiicant. For the young adult, his MWT was 30.4 mm at baseline and 28.2 mm at last follow-up after six months.
Mean LVEDD at baseline for the pediatric patients was 37.8 ± 5.7 mm (z-score = -1.6 ± 1.8). At last follow-up, four patients had a smaller LVEDD (67%, n = 4). Both patients with increased LVEDD, dilated in isolation of ventricular wall thinning, but did experience a drop in LVEF. The mean at last follow-up for the pediatric patients was 36.5 ± 6.7 mm (z-score = -2.1 ± 1.5), with an average paired difference of -0.5 mm. For the young adult, who had LV wall thinning and a drop in his LVEF during follow up, his LVEDD was 43.1 mm at baseline and 46.2 mm at last follow-up after six months.
Mean LV mass at baseline for the pediatric patients was 192.7 ± 133.1 g (z-score = 7.5 ± 6.6). Of the pediatric patients in the cohort (n = 8), 75% (n = 6) had a z-score >2 at baseline. At follow-up (n = 6), six patients had increased LV mass (100%, n = 6). Mean LV mass at last follow-up was 200.7 ± 88.9 g (z-score = 10.9 ± 12.0), with an average paired difference of + 66.2 g, which based on the Wilcoxon signed-rank test, was not statistically significant. For the young adult, he had an LV mass of 835.1 g at baseline and 789.1 g at follow-up after six months. Mean GLS at baseline for the pediatric patients was − 14.1% ± 2.9% which is lower than the − 20% measured in children without any cardiomyopathy [20]. Four pediatric patients (50%, n = 4) had follow-up GLS values, of which two had a GLS that was less negative (50%, n = 2). Mean GLS at last follow-up was − 14.7% ± 5.1%, with an average paired difference of + 0.14%. For the adult patient, the GLS at baseline was − 5.8% and at last follow-up was − 3.0%. Of note, this patient’s LVEF was already less than 50% base baseline. All echocardiogram data can be seen in Table 4; Fig. 5, and Supplementary Fig. 1.
Table 4 Summary table for cardiac measurements at baseline and at last follow-up, with a mean follow-up time of 24.5 months Fig. 5 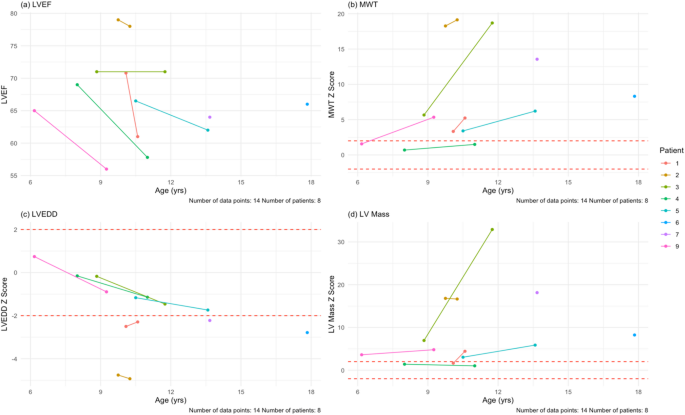
Echocardiogram findings for the pediatric patients in the cohort at their baseline and last follow-up visits. (a) LVEF plotted against age in our cohort. There is a downward trend (blue line) as age increases. (b) MWT z-scores plotted against age in our cohort. DD hearts thicken over time, as in this cohort. (c) LVEDD z-scores plotted against age. There is a downward trend in this age range. (d) LV mass z-scores plotted against age in our cohort. Despite the hearts having more mass, the scores remain relatively stable over time. The mean follow-up time for echocardiogram assessment was 24.5 months. MWT = maximum wall thickness, LVEDD = left ventricular end-diastolic dimension
Electrocardiogram findings
DD causes dysfunctional macroautophagy that results in accumulation of intracellular vacuoles, a mismatch between supply and demand of energy within cells and eventual cell death. The cardiac hypertrophy and fibrosis that occur result in significant electrophysiologic abnormalities including high voltage with repolarization abnormalities, conduction disorders, accessory pathways, and atrial and ventricular arrhythmias. Therefore, electrocardiogram (ECG) findings at baseline were also assessed in all nine patients. Baseline ECG findings included: Wolff-Parkinson-White (WPW) (56%, n = 5), LV hypertrophy (44%, n = 4), biventricular hypertrophy (22%, n = 1), sinus bradycardia (11%, n = 1), and 1st degree atrioventricular (AV) block (11%, n = 1).
Pulmonary function testing
Most of our patients (89%, n = 8) had respiratory related problems: wheezing (44%, n = 4), dyspnea (33%, n = 3), cough (22%, n = 2), asthma allergies (11%, n = 1), and sleep apnea (11%, n = 1). In our cohort, seven patients underwent PFTs at baseline (78%, n = 7) and five patients completed a follow-up visit (71%, n = 5). At baseline, the average percent of predicted seated upright FVC was 74.6% ± 8.5% (2.3 ± 1.3 L) (Table 5). After a mean follow-up time of 5.8 months, one patient had a lower upright FVC (20%, n = 1), one had no change (20%, n = 1), and three had an increase (60%, n = 3). The mean percent of predicted upright FVC at last follow-up was 74.0% ± 9.6% (2.4 ± 1.6 L).
Table 5 Pulmonary function testing results for the cohort Mean percent of predicted supine FVC at baseline was 60.7% ± 12.6% (1.8 ± 1.2 L). After the mean follow-up time, from the five patients who completed a follow-up visit, one patient had a lower FVC (20%, n = 1), one had no change (20%, n = 1), and the rest had an increase (60%, n = 3). Last follow-up percent of predicted supine FVC was 64.4% ± 14.0% (2.0 ± 1.3 L).
The mean percent of predicted FEV1 was 53.6% ± 16.6% (1.6 ± 1.0 L). At follow-up, two patients had a lower percent of predicted FEV1 (40%, n = 2). The mean percent of predicted FEV1 at follow-up was 61.6% ± 16.8% (1.8 ± 1.3 L).
For the FEV1/FVC ratio, the mean percent of predicted was 103.4% ± 1.6% (0.89 ± 0.09). At follow-up, one patient had a lower percent of predicted FEV1/FVC (20%, n = 1), one had no change (20%, n = 1), and three had an increased (60%, n = 3). The mean at follow-up was 108.2% ± 7.7% (0.92 ± 0.05 L).
CPET
In this study, CPET was performed at baseline and at one follow-up visit, with a mean follow-up time of 5.2 months. Five patients performed CPET in our cohort (56%, n = 5) at baseline and at one follow-up, for a total of 10 visits. Our cohort had a baseline mean VO2 max of 17.2 ± 4.4 ml/kg/min (percent of predicted of 39.0 ± 9.0%) (Table 6; Fig. 6a, Supplementary Table 6). After a mean follow-up time of 5.2 months, three patients had a lower VO2 max (60%, n = 3). At last follow-up, the mean VO2 max was 17.6 ± 5.6 ml/kg/min (percent of predicted of 42.6 ± 13.0%). Out of the 10 total visits, six assessments reached an RQ of ≥ 1.0 (60%, n = 6). The baseline mean for ventilatory efficiency (VE/VCO2 slope) was 28.4 ± 2.5 (Table 6; Fig. 6b, Supplementary Table 6). After the mean follow-up time, two patients had a smaller VE/VCO2 slope (40%, n = 2). At last follow-up, the mean VE/VCO2 slope was 29.5 ± 3.2.
Table 6 Summary of CPET parameters and results of the 6MWT Fig. 6 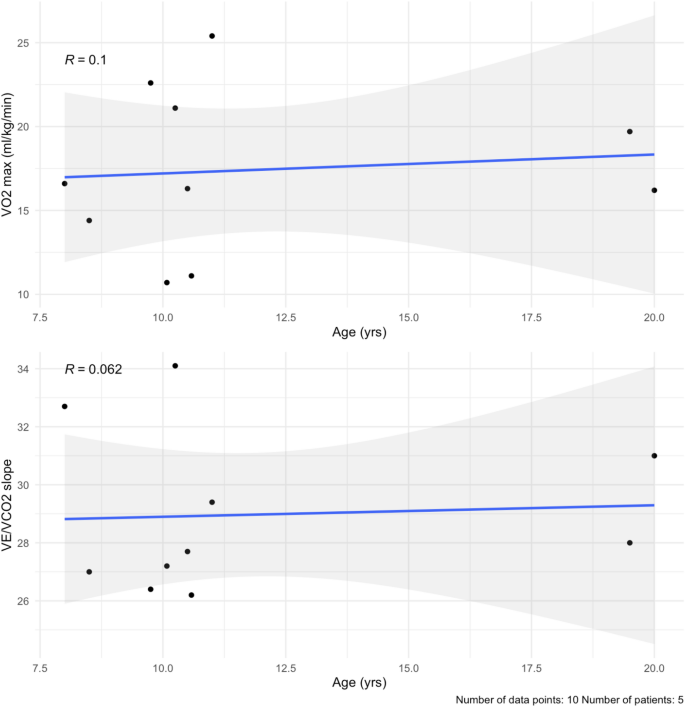
(a) VO2 max by age. There is a small positive correlation with age (blue line), likely due to lung maturity during puberty. (b) VE/VCO2 slope values plotted over time in the cohort. They remain stable over the 6 months. The mean follow-up time was 5.2 months
Neuromuscular assessment
Seven patients (78%) in our cohort reported neuromuscular symptoms at baseline: delay in motor milestones (67%, n = 6), difficulty running (67%, n = 6), difficulty walking (67%, n = 6), fatigue (67%, n = 6), weakness (67%, n = 6), joint pain (33%, n = 3), difficulty sitting (11%, n = 1), hypotonia (11%, n = 1), loss of range of motion (11%, n = 1), and abnormal gait (11%, n = 1). All limbs were found to be affected across the cohort: lower proximal limb (78%, n = 7), lower distal limb (67%, n = 6), upper proximal limb (56%, n = 5), upper distal limb (44%, n = 4).
For the 6MWT, all patients had baseline testing (100%, n = 9), but only seven patients had follow-up testing (78%, n = 7). At baseline, our cohort averaged 448.7 ± 64.7 m (Table 6; Fig. 7, Supplementary Table 7). After a mean follow-up time of 23.3 months, four patients walked shorter distances (57%, n = 4). The mean distance at last follow-up was 405.9 ± 136.1 m, with an average paired difference of -25.9 m.
Fig. 7 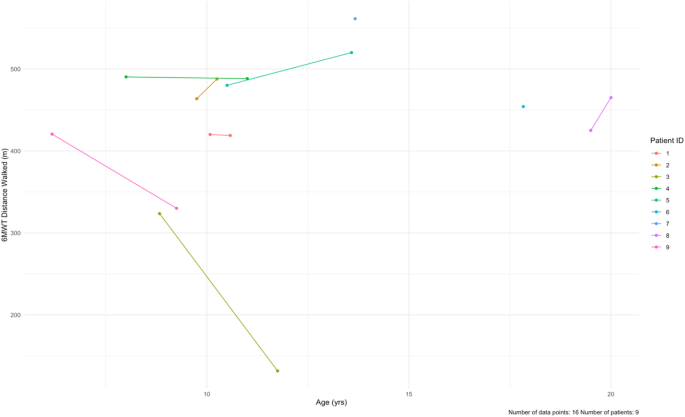
Longitudinal data for the 6-minute walk test (6MWT) at baseline and at follow-up for each patient in the cohort. The data is distance walked (meters) by age. Patients 6 and 7 only had baseline data. The mean follow-up time was 23.3 months
The results for the NSAA, 10MWT, time to rise from floor, and 4SC tests are shown in Fig. 8. For the NSAA, all patients completed the test at baseline (100%, n = 9). Seven patients completed follow-up visits (78%, n = 7), with a mean follow-up time of 23.1 months. The average NSAA total score at baseline was 28 ± 9 out of a max total of 34. After the follow-up time, one patient had a worse NSAA total score (14%, n = 1) and two patients had better scores (29%, n = 2) (Supplementary Table 8, Supplementary Fig. 4a). Out of the seven patients who had follow-up data, four (57%, n = 4) had no changes over 6-, 12-, 24-, and 36-month follow-ups. One of our patients, Patient 3, had markedly worse NSAA total score and 10MWT and 4SC times. Notably this patient had difficulty following instructions, which may have impacted these scores (Supplementary Fig. 4).
Fig. 8 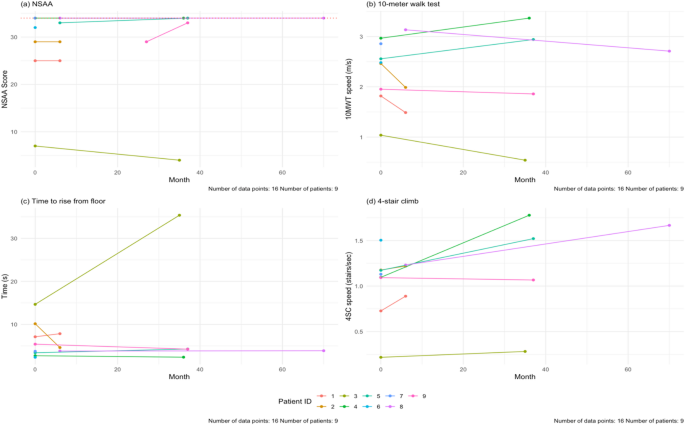
(a) Baseline and last follow-up NSAA scores for the patients in the cohort. The maximum score is 34 (dashed line). The NSAA trended up with age (blue line). (b) Baseline and last follow-up speed during the 10MWT for our cohort. There is a positive correlation with age. (c) Baseline and last follow-up speed during the 4SC in our cohort. There is a positive correlation with age. The mean follow-up time for all these tests is 23.1 months. NSAA = North Star Ambulatory Assessment, 10MWT = 10-meter walk test, 4SC = 4-stair climb test
For the 10MWT, all nine patients (100%, n = 9) completed the test at baseline, but only seven (78%, n = 7) patients had follow-up testing done. The mean follow-up time was 19.4 months. In our cohort, ages 6–20, the baseline average speed was at 2.4 ± 0.6 m/s. At the end of study, two patients were slower (29%, n = 2). The average speed at follow-up was 2.2 ± 1.0 m/s.
For the time to rise from floor test, nine patients completed the test at baseline (100%, n = 9) and seven patients completed follow-up testing (78%, n = 7). The mean follow-up time was 23.3 months. The average time taken at baseline was 5.9 ± 4.1 s. At the end of the study, three patients took longer to rise from the floor (43%, n = 3). The mean time at last follow-up was 8.9 ± 11.8 s.
For the 4SC, we had nine patients complete the test at baseline (100%, n = 9), and seven patients with follow-up visits (78%, n = 7). The average speed at baseline was 1.1 ± 0.4 stairs/sec. After the mean follow-up time of 19.4 months, two patients were slower (29%, n = 2) (Fig. 8d).
Laboratory parameters
All patients completed the baseline laboratory measurements and follow-up with a mean follow-up time of 18.6 months. Of note, cardiac biomarkers including N-terminal pro brain natriuretic peptide (NT-proBNP) and high sensitivity cardiac troponin T (hs-cTnT) were elevated at both baseline and follow-up. Similarly, skeletal biomarkers including CPK and aldolase were similarly elevated at baseline and follow-up, as were AST, ALT and LDH (Table 7). Figure 9 shows the values for NT-proBNP and hs-cTnT for all patients at baseline and follow-up only, where mean paired difference was 971.3 pg/mL and 37.3 respectively, which based on Wilcoxon signed-rank test was a significant increase in NT-proBNP, but not hs-cTnT; Supplementary Fig. 5 shows the values at all visits.
Table 7 Lab values for the cohort, summarized at baseline and at last follow-up Fig. 9 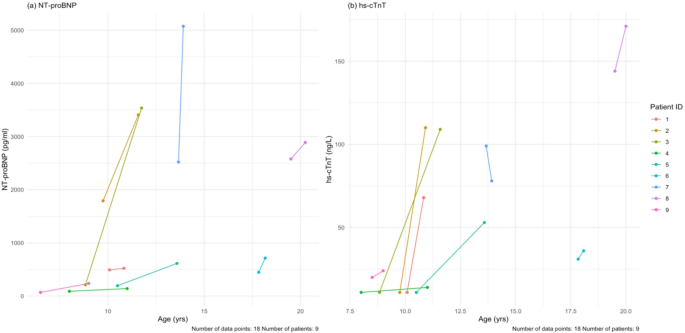
(a) Baseline and last follow-up NT-proBNP values for each patient. (b) Baseline and last follow-up hs-cTnT values for each patient. The mean follow-up time for all these tests is 18.7 months. NT-proBNP = N-terminal pro brain natriuretic peptide, hs-cTnT = high sensitivity cardiac troponin T
Continue Reading
-
MiR-877, an exosomal miRNA from mechanical stretch induced adipose derived stromal cells, enhances fracture healing in nonunion rats with type 2 diabetes mellitus | Stem Cell Research & Therapy
Establishment of T2DM rats fracture model and rats treatments
The work has been reported in line with the ARRIVE guidelines 2.0.
After adapting to feeding for three days, the Sprague Dawley (SD) rats were weighed and classified by cage (3 rats/cage), and 60 male SD rats of 3 weeks old were randomly distributed into 2 groups. Many studies have shown the procedures of establishing high-fat fed (HFD) and streptozotocin (STZ)-induced diabetic rat model which are a model of T2DM. According to the procedures of induction of the T2DM rat model in the existing study, after 3 weeks of feeding HFD (containing 60% fat), rats in the T2DM group were injected with STZ (40 mg/kg in citrate buffer). The control group fed with a normal pelleted diet received an equal volume of citrate buffer [21, 22].
The blood glucose (BG) levels were evaluated consecutively, and blood samples were collected from the tail vein. According to the procedures, rats with randomly blood glucose (RBG) samples > 16.7 mmol/L more than three times were identified to have T2DM after 7 weeks. During diabetes induction, animals were given free access to their original diets (received the high-fat or control diet and water ad libitum) for 12 weeks.
To assess the T2DM model, we measured the metabolic index, including body weight, food intake, water consumption and volume of excreted urine at several time points, including before being fed the HFD and 12 weeks after STZ injection. In addition, RBG was observed at several special time points, which included before fed HFD, before STZ injection, one week after STZ injection, 6 weeks after STZ injection and 12 weeks after STZ injection. At the end of the observation, IPGTT and ITT were evaluated. In detail, to execute IPGTT, animals were fasted for 12 h and injected with 1.5 g/kg glucose. BG was measured at 0, 30, 60 and 120 min after glucose injection. While ITT was carried out by injecting the rats with 0.75 IU/kg insulin, and then BG was obtained at 0, 30, 60 and 120 min after insulin administration. Animals with an RBG below 10 mmol/L at any time points were regarded as nondiabetic, and those with an RBG between 10 and 16.7 mmol/L were excluded. At 12 weeks after STZ injection, rats remaining in the T2DM group were evaluated as diabetic rats in a model of T2DM [23, 24].
After 15 weeks of treatment, all the successfully induced T2DM rats received general anesthesia with pentobarbital sodium intraperitoneal injection before surgery. A lateral incision was made along the proximal femur, followed by longitudinal dissection of the skin, subcutaneous tissue, and muscle along the femoral axis. The surrounding soft tissues were gently separated to expose the femur. A transverse osteotomy of the mid-diaphysis of the femur was performed by an oscillating mini-saw to establish a transverse femur shaft fracture model. The knee was bent 90 degrees, the lateral patellar incision was made, and the Kirschner needle was inserted femur intramedullary through the femoral intercondylar groove. The tip of the Kirschner needle was inserted through the top of the femoral greater trochanter to stabilize the fracture. Finally, all the incisions were closed using a 4-0 nylon suture. All the rats were kept in individual cages. Unprotected weight bearing was allowed immediately after the operation. After surgery, all the animals were given food and water ad libitum. At the end of the experiments, a sodium pentobarbital solution was administered intraperitoneally at a dose of 200 mg/kg. Following administration, animals were carefully monitored until the complete cessation of respiration and heartbeat, and a secondary physical method was applied when necessary to confirm death. All procedures were performed by personnel trained in rodent euthanasia.
Based on X-ray examinations, the fracture sites in the rats were located and marked on their skin. Then, 600 µL of ADSC-exosomes induced by mechanical stretch at a concentration of 200 µg/mL, as well as an equal volume of PBS, were locally injected into the fracture site every three days after surgery, with 200 µL administered each time. Finally, X-ray examination, micro-CT examination, histochemistry analysis, and Western blot analysis of the fractured femurs were performed 28 days after the operation.
Cells obtaining and culture
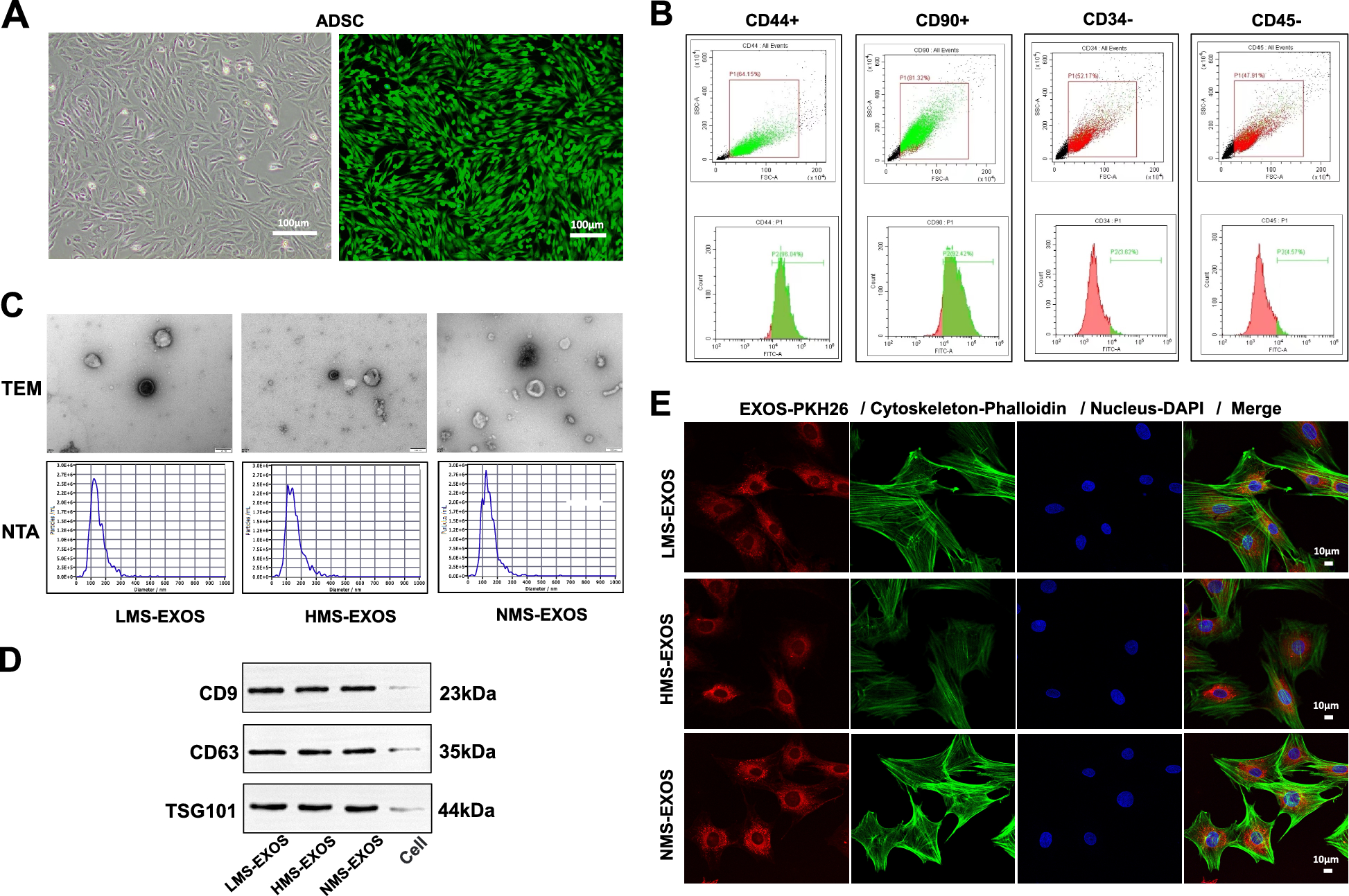
To obtain ADSCs, the subcutaneous fat in the groin of 3 weeks old male rats was cut into pieces as small as possible and centrifuged at 1500 rpm for 10 min to extract the sediment and glue enzyme was added in to digest at 37 °C for 40 min, then added the medium to terminate the reaction, and the mixture was filtered with a 70 μm filter. After centrifugating at 1500 rpm for 8 min, the cells were suspended in the medium and cultured in vitro for about 8 days. ADSCs (CD44+ CD90+ CD34-CD45-) were collected and certified by flow cytometry and the activity of ADSCs was determined by Calcein Acetoxymethyl Ester (Calcein AM) (Beyotime Biotechnology, Shanghai, China) staining assay.
Bone marrow cells were extracted from the femur and tibia of 3-week-old male rats, then isolated and cultured for 3 generations. BMSCs (CD44+ , CD34-) were identified by flow cytometry, and the cellular bioactivity of BMSCs was determined by Calcein AM staining assay.
The HUVECs (PUMC-HUVEC-T1; Cat NO: CL-0675) used in our experiments were originally purchased from a commercial vendor (Wuhan Pricella Biotechnology Co., Ltd.). To mimic the true condition and environment of Type 2 Diabetes Mellitus. All cells used in cellular function experiments were cultured with a complete culture medium consisting of high-concentration glucose (30 mM).
Tensile strain treatments of cells
Cell’s mechanical stimulation device has become a well-established method to apply mechanical strain to cultured cells; numerous similar devices for cell stimulation have been developed. In this study, external tensile strain was applied to ADSCs using a cell tension culture system. The special elastic membrane or well of the cell tension culture system was precoated with Matrigel (Corning, Bedford, MA, USA), incubated overnight, and kept moist with PBS for later use. ADSCs were cultured on the coated membrane or well. Cyclic tensile strain was applied using a uniaxial elongation model either 24 h post-seeding or upon reaching 90–100% confluence to simulate mechanical stimulation. In the selected uniaxial elongation model, cyclic sinusoidal tensile strain at a fixed frequency was applied to the cells according to a predefined protocol. All the ADSCs were divided into 3 groups, in which ADSCs were given of 1.0 Hz 6% (lower magnitude mechanical stretch ADSCs, LMS), 1.0 Hz 18% (higher magnitude mechanical stretch ADSCs, HMS) tensile strain, 2 h per day separately, and a total of 3 days. In the non-stress group (non-mechanical stretch ADSCs, NMS), 0% tensile strain was applied to ADSCs for 3 days in succession [25,26,27].
Isolation and identification of ADSC exosomes
After exposure to the corresponding tensile strain, ADSCs were washed three times with PBS and then cultured in exosome-free, FBS-free basal medium for an additional 24 h. Exosomes were isolated using the technique of differential centrifugation. In detail, the supernatant was collected and centrifuged at 1000×g at 4 °C for 10 min, 2000×g at 4 °C for 10 min, then centrifuged at 10000×g at 4 °C for 30 min, and centrifuged at 140000×g at 4 °C for 90 min in turn using a Beckman Coulter ultracentrifuge (Beckman Coulter, USA). Discard supernatant PBS washing sample, 140000×g centrifuge for 90 min at 4 °C. The precipitated exosomes were collected and re-suspended in 0.5 mL PBS and conserved at − 80 °C [28]. Then the volume of exosomes was concentrated to 200 μL. The morphology of exosomes was observed by transmission electron microscope (TEM; HITACHI, HT7700, JAPAN) and the diameter distribution was analyzed by Nanoparticles Tracking Analysis (NTA; ZetaView, Particle Metrix, Meerbusch, Germany). Western blot analysis identified its specific biomarkers (CD9, CD63, TSG101).
Flow cytometry (FCM) assay
ADSCs were analyzed by flow cytometry. ADSCs were detected with specific biomarker antibodies CD44 (Affinity), CD90 (Abcam), CD34, and CD45 (Abcam). BMSCs were certified by specific biomarkers CD44 (Affinity) and CD34 (Abcam). Results were analyzed using Flowjo software (version 10.0; BD Biosciences).
Exosome uptake assay
Based mainly on the manufacturer’s standard procedure, PKH26 was used as a dye to label the exosomes in the exosome uptake assay. In short, exosomes were obtained with differential centrifugation (140,000×g, 20 min, 4 °C) dyed with PKH26 (mixed solution was incubated for 20 min at room temperature). While BMSCs were seeded onto a 35 mm confocal dish at the proper density and labeled with DAPI dye. Then, exosomes labeled with PKH26 were mixed and co-cultured with BMSCs labeled with DAPI for 12 h and finally observed via a confocal laser scanning microscopy (CLSM, Leica Microsystems, Germany).
ALP activity and mineralization assessment of osteogenic differentiation
Following three passages of culture, BMSCs were seeded into 6-well plates (2 × 105 cells per well) that had been pre-coated with a 0.1% gelatin solution. The plates were then incubated for 14 days using a specific osteogenic induction medium (Cyagen Biosciences). To evaluate the effect of ADSCs-Exos on osteogenic differentiation, 200 µL of ADSCs-Exos (LMS-Exos, NMS-Exos, HMS-Exos derived from ADSCs) with a concentration of 200 µg/mL and equal volumes of PBS were added into every well severally with the osteogenic induction medium, and the medium was refreshed every three days. To evaluate the level of osteogenic differentiation, the cells were stained with alizarin red staining (ARS) dye and alkaline phosphatase (ALP) staining, and were collected for Western Blotting analysis on day 14. In detail, BMSCs were osteogenic induced for 14 days with different treatments, then cells were washed two times via PBS, then fixed with 4% paraformaldehyde for 30 min at room temperature prepare for ALP and ARS staining. A BCIP/NBT ALP kit (Beyotime, China) was used for ALP staining. After the stained cells were washed using PBS three times, the BCIP/NBT substrate was utilized to stain osteogenic-induced BMSCs. The results were observed and imaged via optical microscopy and then calculated and evaluated by the Image J software processing system (NIH, USA), and GraphPad Prism 10.0 (GraphPad Software, CA, USA) was used for the data analysis.
Tube formation assay of ADSC-Exos
HUVECs were cultured in Matrigel (Corning, USA) precoated 24-well plates (1 × 105 cells per well). 200 µL of ADSCs-Exos (LMS-Exos, NMS-Exos, HMS-Exos derived from ADSCs) with a concentration of 200 µg/mL and equal volumes of PBS were added into every well with the medium, respectively. 6 h later, tube formation was observed with a fluorescence microscope. The Image J software processing system (NIH, USA) and GraphPad Prism 10.0 (GraphPad Software, CA, USA) were used for quantification and data analysis.
Scratch test and migration test
HUVECs were cultured in 6-well plates (2 × 105 cells per well). 200 µL of ADSCs-Exos (LMS-Exos, NMS-Exos, HMS-Exos derived from ADSCs) with a concentration of 200 µg/mL and equal volumes of PBS were added into every well with the medium without serum. 24 h later when cultured HUVEC cells reached 100% confluence, a straight scratch was made with a 200 µL pipette in every well. 0 h, scratched wounds were observed with a fluorescence microscope and recorded. 12 h later, Scratch wound healing results were observed with a fluorescence microscope and photos were taken. Before observation, all samples were stained with calcein AM dye (Beyotime Biotechnology, Shanghai, China). The Image J software processing system (NIH, USA) and GraphPad Prism 10.0 (GraphPad Software, CA, USA) were used for quantification and data analysis.
Transwell assay
HUVECs treated with 200 µL of ADSCs-Exos (LMS-Exos, NMS-Exos, HMS-Exos derived from ADSCs) with a concentration of 200 µg/mL and equal volumes of PBS were seeded into 24-well transwell of 8 µm pore diameter cell culture plate (Corning, USA). 12 h later, HUVECs were stained with crystal violet for 20 min, and then observed by an optical microscope. The Image J software processing system (NIH, USA) and GraphPad Prism 10.0 (GraphPad Software, CA, USA) were used for quantification and the data analysis.
Cell alive/dead assays
All cells, including ADSCs, HUVECs, and BMSCs, were stained before use via calcein AM and Propidium iodide (PI) dye (Beyotime Biotechnology, Shanghai, China) to evaluate cell vitality.
Western blot analysis
Western blotting was performed following previously described protocols. First, after the concentrations of protein were measured via BCA (Aspen), the protein was separated into equal amounts via SDS-PAGE (Beyotime, China), transferred into the PVDF membrane (Millipore, Burlington, MA, USA) and then incubated with 5% bovine serum albumin for 1 h at 25 °C. Next, the membranes were incubated overnight with primary antibodies specific for CD9 (Abcam), CD63 (Abcam), TSG101 (Abcam), Runx2 (Abcam), OCN (Santa), and GAPDH (Abcam). HRP-labeled secondary antibody (Abcam, USA) was added, and then, the membrane was visualized using a T5200 Multi Chemiluminescence Detection System (Tanon, China) as recommended of the manufacturer. The membranes were incubated with Immobilon ECL reagent (Thermo Fisher Scientific, Waltham, MA, USA), and the bands were quantified via Image J software (NIH, USA). GAPDH protein level was used as an internal control for MACF1. The Image J software processing system (NIH, USA) and GraphPad Prism 10.0 (GraphPad Software, CA, USA) were used for quantification of protein level and the data analysis. The significance level was set to a 95% confidence interval, and statistical significance was declared as * p < 0.05, ** p < 0.01, *** p < 0.001, **** p < 0.0001 and ns p > 0.05.
Micro-CT analysis
The animals were euthanized 4 weeks postoperatively, the internal fixations were removed and their femurs were fixed in 4% paraformaldehyde for 24 h at 4 °C. Then, tissue specimens were scanned via a micro-CT system (SkyScan1276, Bruker, Belgium) at a resolution of 9.054604 μm with 85 kV and 200 µA. After scanning, 3D structures of femurs were performed (Reconstruction was accomplished by NRecon (version 1.7.4.2)), and the new bone volume/total volume (BV/TV) were calculated to assess bone regeneration in the fracture site to assess the morphology of the reconstructed femurs (3D and 2D analysis were performed using software CT Analyser (version 1.20.3.0)).
qRT‑PCR analysis
Total RNA was isolated from exosomes using TRIZOL Extraction Reagent (G3013, Servicebio). The cDNA was reverse transcribed using RevertAid First Strand cDNA Synthesis Kit (Invitrogen, CA, USA) following the manufacturer’s instructions. And the qRT-PCR for mRNAs was performed on a StepOne™ Real-Time PCR System (Life technologies) using EnTurboSYBR Green PCR SuperMix (EQ001, ELK Biotechnology) or HieffTM qPCR SYBR™ Green Master Mix (No Rox Plus) (11201ES, Shanghai Yeasen BioTechnologies). The relative expression levels of mRNA or miRNA were normalized to those of GAPDH or U6 and evaluated using the 2−ΔΔCT method. The primers used for qRT-PCR are listed in Table 1.
Table 1 The sequences of primers used for PCR studies Transfection
Following manufacturer’s protocols, miR-877 mimics or inhibitors and their NCs (Generalbiol, HeFei, China) were transfected into BMSCs and HUVECs to evaluate miR-877 function. After 48 h of transfection, the expression level of miR-877 was measured by qRT-PCR.
RNA sequencing and bioinformatics analysis
All the samples were processed as description previously. All the experiment procedures were according manufacture’s protocols and recommendations. Briefly, Total RNA was extracted from exosomes using TRIzol reagent (Invitrogen, CA, USA) according to the manufacturer’s protocol. Purity, concentration and integrity of RNA sample were examined by NanoDrop, Qubit 2.0, Agilent 2100, etc. RNA concentration and purity was measured using NanoDrop 2000 (Thermo Fisher Scientific, Wilmington, DE). RNA integrity was assessed using the RNA Nano 6000 Assay Kit of the Agilent Bioanalyzer 2100 system (Agilent Technologies, CA, USA). Only RNA with good quality could move on to following procedures. Total RNA from each sample was used to prepare miRNA library using NEB Next Ultra small RNA Sample Library Prep Kit (NEB, Boston, MA, USA) according to the Illumina small RNA sample preparation protocol. Sequencing was then performed on the Illumina novaseq6000 platform (Illumina, San Diego, CA). A total amount of 1.5 μg RNA per sample was used as input material for the RNA sample preparations. Briefly, first of all, ligated the 3′SR Adaptor. Mixed 3′SR Adaptor for Illumina, RNA and Nuclease-Free Water, after mixture system incubation for 2 min at 70 °C in a preheated thermal cycler, the Tube was transfer to ice. Then, add 3′ Ligation Reaction Buffer (2X) and 3′Ligation Enzyme Mix ligate the 3′SR Adaptor. Incubated for 1 h at 25 °C in a thermal cycler. To prevent adaptor-dimer formation, the SR RT Primer hybridizes to the excess of 3′SR Adaptor (that remains free after the 3′ligation reaction) and transforms the single stranded DNA adaptor into a double-stranded DNA molecule. And dsDNAs are not substrates for ligation mediated. The second, ligated the 5′SR Adaptor. Then, reverse transcription synthetic first chain. Last, PCR amplification and Size Selection. PAGE gel was used for electrophoresis fragment screening purposes, rubber cutting recycling as the pieces to get small RNA libraries. At last, PCR products were purified (AMPure XP system) and library quality was assessed on the Agilent Bioanalyzer 2100 system. The clustering of the index-coded samples was performed on a cBot Cluster Generation System using TruSeq PE Cluster Kit v4-cBot-HS (Illumia) according to the manufacturer’s instructions. After cluster generation, the library preparations were sequenced on an Illumina Hiseq 2500 platform and paired-end reads were generated. Raw data (raw reads) of fastq format were firstly processed through in-house perl scripts. In this step, clean data (clean reads) were obtained by removing reads containing adapter, ploy-N and low-quality reads from raw data. And reads were trimmed and cleaned by removing the sequences smaller than 18 nt or longer than 30 nt. Differential expression analysis of two groups was performed using the DESeq R package (1.10.1). DESeq provide statistical routines for determining differential expression in digital miRNA expression data using a model based on the negative binomial distribution. The resulting P values were adjusted using the Benjamini and Hochberg’s approach for controlling the false discovery rate. miRNA with an adjusted p < 0.05 found by DESeq were assigned as differentially expressed. Target gene function was annotated based on the following databases:Nr (NCBI non-redundant protein sequences); Nt (NCBI non-redundant nucleotide sequences); Pfam (Protein family); KOG/COG (Clusters of Orthologous Groups of proteins); Swiss-Prot (A manually annotated and reviewed protein sequence database); KO (KEGG Ortholog database); GO (Gene Ontology).
Histological and immunofluorescence analysis
The collected femurs of rats from different groups were fixed in 4% paraformaldehyde solution for 48 h, decalcified with 20% EDTA at 25 °C for 28 days, embedded in paraffin, and sectioned along the longitudinal axis. Sections from the fracture region were stained with hematoxylin and eosin (H&E), safranin O-fast green, Masson, RUNX2, OCN for immunohistochemical analysis. Immunofluorescence staining with α-SMA, CD31, RUNX2, OCN for immunofluorescence analysis. The sections were imaged and observed by a microscope.
Statistical analysis
All the experiments were performed at least three replicates per group. Values were presented as mean ± SD, and were analyzed with GraphPad Prism 10.0 (Graph-Pad Software, CA, USA). Variances between groups were assessed by the two-sided Student’s t-test (for two-group comparisons) or the one-way analysis of variance (ANOVA) with Tukey’s test (for more than two-group comparisons). And statistical significance was declared as* p < 0.05; ** p < 0.01; *** p < 0.001; **** p < 0.0001; ns p > 0.05, not significant.
Continue Reading
-

Pakistan’s seafood exports to China grow 25% in Q1 2025
Pakistan’s seafood exports to China reached $153 million in the first quarter of 2025, up from $121.93 million in the same period in 2024, according to…
Continue Reading
-

Glasgow refuses to rush George Square opening for Commonwealth Games
 Getty Images
Getty ImagesGeorge Square was a hub for visitors during the Commonwealth Games in 2014 Work to redevelop Glasgow’s George Square will not be “accelerated” to get it ready for the Commonwealth Games next year, the council has said.
The square is…
Continue Reading
-

Infectious diseases are killing deer and risking rural US economies: ‘You smell the dead everywhere’ | US news
When landowner and hunter James Barkhurst went scouting his property about a month ago to assess the local deer population ahead of the fall hunting season, he was left in shock.
“I’ve seen about 14 dead in less than a mile stretch. There’s…
Continue Reading

