Engineers at the University of Massachusetts Amherst have developed an artificial neuron whose electrical activity closely matches that of natural brain cells. The innovation builds on the team’s earlier research using protein nanowires made from…
Blog
-

Silent killer: 60% of global deaths are now tied to chronic inflammation
Chronic inflammation is now being viewed as a sneaky culprit that affects up to half of adults globally. Modern science shows 60 % of global deaths are attributed to diseases linked with chronic inflammation, and people silently suffer from…
Continue Reading
-
Mom’s voice boosts language-center development in preemies’ brains, study finds
The researchers recorded mothers reading a chapter of Paddington Bear, a children’s book that has been translated into many languages. Each mother made a recording for her baby in her native language.
The babies were…
Continue Reading
-
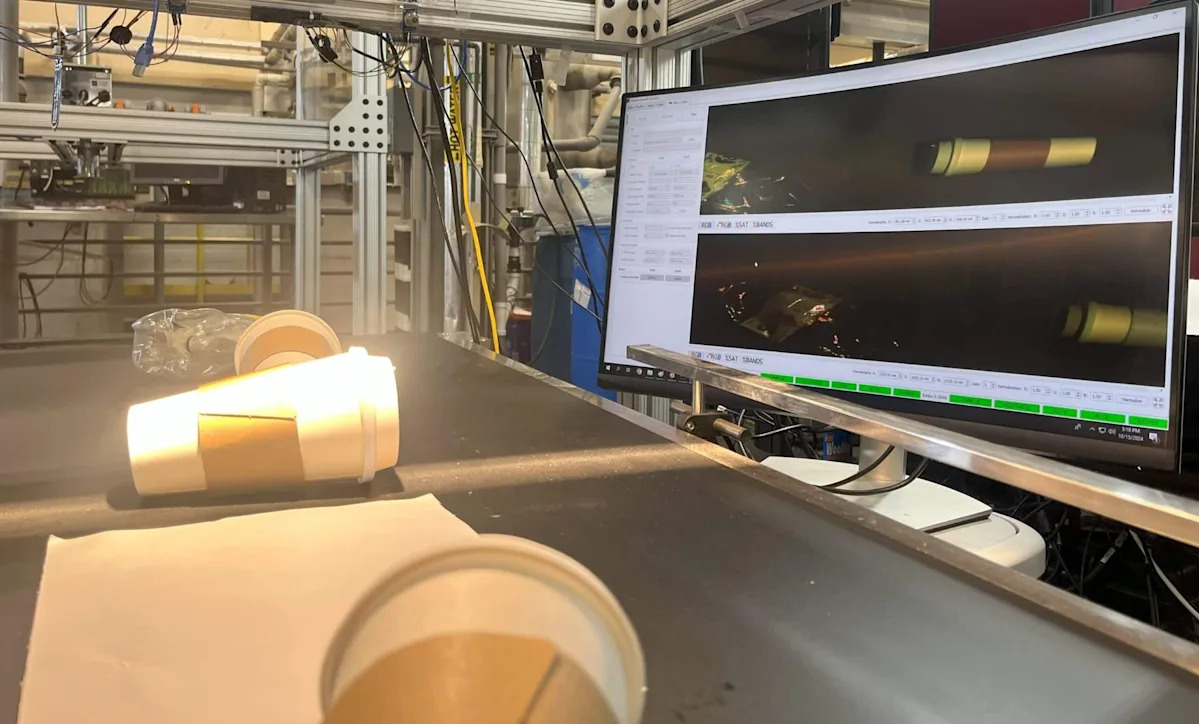
‘Allows us to see what human eyes … can’t’
Researchers at North Carolina State University have published an inquiry into advanced hyperspectral imaging technology as a potential jumping-off point for sorting municipal waste.
The study, published in the journal Matter, discusses the…
Continue Reading
-

Phakic Intraocular Lenses for Presbyopia Correction: Objective Evaluat
Introduction
Presbyopia – the reduced ability of the natural lens to accommodate – affects almost all individuals by the age of 50, leaving them with decreased near visual acuity (VA). In 2011 alone, it is estimated that from a total of 244 million cases of uncorrected or under-corrected presbyopia in people aged less than 50 years, there was an approximate worldwide $11.023 billion loss in potential productivity.1 One novel way to manage presbyopia is by the implantation of phakic intraocular lenses (IOLs) – IOLs that are placed over the natural lens rather than replacing it. These lenses refract light either via distinct regions with various radii of curvature, or diffractively by inducing add powers through Fresnel zones, which refract the light differently than their lens-base.2 Phakic IOLs allow for patients to maintain their residual ability to accommodate, receive a refractive intraocular lens if needed, and avoid an increased risk of retinal detachment during this procedure if they are highly myopic.3–6 Previous studies have extensively reported positive outcomes on various phakic IOLs in refractive surgery,3,7–9 however few studies have explored their outcomes in presbyopia management.10–13
In 2020, Schmid and Luedtke established promising results for the use of phakic IOLs in correcting presbyopia, where 8 patients undergoing presbyopia correction with a diffractive posterior chamber phakic IOL reached a median uncorrected distance VA of at least 0.1logMAR with no need for reading glasses at one-month post-operation.14 Four prospective studies by Stodulka et al, Takahashi et al, Bianchi et al, and Güel et al have found patients undergoing presbyopic phakic IOL correction to have significantly improved VA at follow-ups.15–18 While such studies have reported positive outcomes for phakic IOL use in presbyopia management, they are limited in numbers and no previous study has yet directly compared a refractive and a diffractive phakic IOL for presbyopia management.
In this study, we evaluated and compared the optical quality of a diffractive phakic IOL – the IPCL with +2.5 diopters (D) add power (Care Group) – and a recently introduced refractive phakic model designed for presbyopia correction – the Artiplus (Ophtec). By measuring their optical-quality metrics and simulating postoperative VA at various aperture sizes and near, intermediate, and far distances, we aimed to provide comprehensive information on the optical properties of both approaches in the same study, allowing for better direct comparison of the models and a more personalized selection of phakic IOL based on patients’ needs.
Methods
Phakic IOLs
The Artiplus Model 470 (Artiplus) is a polysiloxane iris-fixated refractive phakic IOL (Ophtec, Groningen, the Netherlands),19 which has recently obtained a CE-marking. Its multi-segmented optic using the continuous transitional focus technology allows for improved VA at near, intermediate, and far distances (Figure 1). Its refractive index is 1.43, with dioptric powers ranging from +2.0 to −15.0D in 0.5D increments. Artiplus has an overall diameter of 8.5mm with a 6.0mm convex-concave body. We used an Artiplus IOL with a power of −3D.
Figure 1 Artiplus phakic intraocular lens (photo courtesy with permission from Ophtec, the Netherlands).19
The IPCL V2.0 is a hybrid hydrophilic acrylic phakic IOL with a refractive index of 1.465. It features a central hole to allow aqueous flow and six haptic pads to ensure its stability in the ciliary sulcus (Care Group, Gujarat, India).20 It has an optic diameter of 6.60mm that can be customized up to 7.25mm with sizes ranging from 11.00 to 14.00mm (0.25mm step).21 The IPCL is available in the broad power range of −30.0D to +15.0D in 0.5D increments. The added power can also be customized by offering +1.5D, 2D, 2.5D, 3D, and 3.5D secondary foci. In the current study, we used an IPCL with a power of −3D and an add power of +2.5D, aligning with the range of the Artiplus model.
In our experiments, the optical power of the natural lens was modeled with a 23D Precizon Monofocal (Ophtec, Groningen, the Netherlands), with no spherical aberration. When assembling the 23D monofocal and phakic IOL with one another, the overall corneal aberration (0.27 µm) was similar to the mean of 0.280 µm (±0.086 µm) reported in the literature.22
Optical Setup
The 23D monofocal and phakic IOLs were assembled into a custom-made and 3D-printed insert with the 23D monofocal placed posterior to the phakic IOL to simulate the in-vivo condition of the natural lens being posterior to a phakic IOL (Supplemental Figure 1). An estimated distance between the two lenses was 0.5mm, determined based on the IOL geometry and a dedicated spacer incorporated into the 3D-printed holder, which had a designed gap of 1.2 mm. The printing accuracy was approximately ±0.1mm. This resulting distance was comparable to the separation found between phakic IOLs and the crystalline lens (0.609±0.165mm) in the literature.23
The optical quality of the phakic IOLs was evaluated with the Laboratory’s OptiSpheric IOL PRO2 (Trioptics GmbH, Wedel, Germany), with its design adhering to ISO 11979-2.24,25 Two samples of each phakic IOL were tested for all experiments after placing them in a balanced salt solution (BSS, Bausch+Lomb, United States). Two samples sufficed for the experiments given the OptiSpheric’s accuracy against a reference lens (2% for MTF testing)26 and the lab’s previous studies indicating high reproducibility27,28 and repeatability29 of the optical quality of IOLs, regardless of type or refractive power, using the laboratory’s OptiSpheric. Measurements were conducted with a photopic filter, and 3.0- and 4.5-mm apertures. A corneal model with 0.27µm of spherical aberration at 5.15mm was used representing the average value reported in the normal population,22,28–31 and simulations were performed in polychromatic light to more closely mimic natural viewing conditions.
Image Quality Metrics
Variables measured with the setup included modulation transfer function (MTF). In addition to comparing the phakic IOLs’ MTF curves, the area under the curve of the MTFs (MTFa) up to 50 lp/mm with the simulated VA conversion was calculated using the methods outlined elsewhere.32 The through-focus MTF (TF MTF) was compared at 25, 50, and 100 lp/mm. Lastly, the 1951 USAF resolution test images were recorded. The results were graphed and analyzed with custom-made software (MATLAB, MathWorks, USA).
Results
Figure 2 shows the MTF levels of the IPCL and Artiplus phakic IOLs for a 3mm pupil measured at far, intermediate, and near focus. At this aperture, the lenses showed close MTF values at all distances.
Supplemental Figure 2 shows the TF MTF of the tested phakic IOLs for a 3mm pupil at 25, 50, and 100 lp/mm at a defocus range of 1 to −3D at the spectacle plane. At all tested frequencies, both the IPCL and Artiplus IOLs had a primary peak at 0D. At approximately −1.9D, IPCL had a higher secondary peak compared to Artiplus, but at the expense of a lower contrast at the intermediate range with a steep decline from the primary to the secondary focus. Given IPCL being a diffractive phakic IOL, such a bimodal shape of the TF MTF curve is expected.

Figure 2 Modulation transfer function curves of the tested lenses at three foci for a 3mm aperture. The tested foci included best far, intermediate, and near focus. The dotted lines show the values of each lens separately; the solid lines refer to the average of two lenses.
Abbreviation: MTF, modulation transfer function.
Figure 3 presents the MTFa and simulated VA (logMAR) for the two lenses at a 3mm aperture. The two lenses had a similar primary peak at 0D, but IPCL had a second primary peak at approximately −1.9D. At an intermediate defocus of −1D, Artiplus showed a higher MTFa (0.32 versus 0.25) and better simulated VA (0.05 versus 0.13logMAR) than the IPCL.

Figure 3 The area under MTF curve and simulated VA of the tested lenses at 3mm aperture. The MTFa and simVA are graphed as a function of spectacle defocus. The dotted lines show the values of each lens separately; the solid lines refer to the average of two lenses.
Abbreviations: MTFa, area under the modulation transfer function; simVA, simulated visual acuity.
At a 4.5mm aperture as shown in Figure 4, the MTF level of lenses at far, intermediate, and near focuses showed decreased values compared to the 3.0mm aperture, due to the presence of corneal spherical aberration. Notably at the near focus, IPCL had a lower MTF at all spatial frequencies compared to the Artiplus lens with the 4.5mm aperture, indicating a deficiency in near performance at higher apertures.
With the 4.5mm aperture, TF MTF values of the lenses at 25, 50, and 100 lp/mm decreased for all lenses compared to the 3.0mm aperture (Supplemental Figure 3). Still, both models preserved their multifocal properties extending the depth of focus at 4.5mm.

Figure 4 Modulation transfer function curves of the lenses at three foci for a 4.5mm aperture. The tested foci included best far, intermediate, and near focus. The dotted lines show the values of each lens separately; the solid lines refer to the average of two IOLs.
Abbreviaton: MTF, modulation transfer function.
Nevertheless, the IPCL’s tolerance to hyperopic and negative defocus appeared further reduced at the extreme ends of the MTFa and simulated VA presented in Figure 5, demonstrating a steeper decline in its optical quality. Artiplus demonstrated a bimodal simulated VA with peaks of 0.05logMAR at −0.5D and 0.13logMAR at −2.4D. In contrast to the Artiplus, IPCL demonstrated a narrower simulated VA curve with a primary peak of 0.05logMAR at −0.25D. Testing with larger apertures also revealed that the optical performance of both the IPCL and the Artiplus was comparable in the intermediate range, with the two curves overlapping at −1.0D, which contrasts with the lens IPCL performance measured at 3mm.

Figure 5 The area under MTF curve and simulated VA of the tested lenses at 4.5mm aperture. The MTFa and simVA are graphed as a function of spectacle defocus. The dotted lines show the values of each lens separately; the solid lines refer to the average of two lenses.
Abbreviations: MTFa, area under the modulation transfer function; simVA, simulated visual acuity.
The USAF resolution target images presented in Figure 6 confirmed the MTFa results. At −1.0D, Artiplus has better image resolution than IPCL with the 3.0mm aperture, while its resolution became more similar to IPCL at the 4.5mm aperture. At −2.0D with the 3.0mm aperture, IPCL had a better image resolution than the Artiplus, but at the same defocus value with the 4.5mm aperture, IPCL had a worse contrast than the Artiplus. Overall, at both pupil sizes, especially the 4.5mm size, Artiplus had an improved image quality at the ends of the defocus range, compared to the IPCL.

Figure 6 The United States Air Force target images for tested lenses across defocus range. The defocus range included +1.0D to −3.0D, at 0.5D increments at 3-mm and 4.5-mm apertures.
Discussion
Given phakic IOL’s recent introduction to presbyopia treatment, the literature on laboratory studies evaluating such lenses is still limited. Our study tested and compared the optical performance of refractive versus diffractive phakic IOLs – IPCL (+2.5D add) and Artiplus – at 3.0 and 4.5mm apertures for surgical management of presbyopia. We demonstrated good optical quality of the two models across the studied focus range, with the Artiplus providing a flatter simulated defocus curve. While expected differences in VA between the two approaches were minimal, they may become more pronounced in patients with larger pupils.
Our study’s MTF values of the IPCL with +2.5D added power at the 3.0mm aperture decreased with spatial frequency, and the curves decreased to lower MTF values with an increased aperture size of 4.5mm. The IPCL phakic IOL for presbyopia has been studied in a laboratory by Yu et al with additional powers of 2D and 4D at a 3.0mm aperture.33 Yu et al found the MTF values at 100 cycles/mm to be 27% and 24% with the 2D and 4D add powers respectively, compared to our study with MTF values closer to 11% at 100 cycles/mm. The reason for this discrepancy and the lower MTF value reported in our study results from differences in the optical setups applied in both studies. The primary factor limiting the IOL performance using our approach is the presence of corneal spherical aberration. In contrast, the corneal lens used by Yu et al was designed to minimize spherical aberration, as inferred from its resemblance to the corneal model outlined in the ISO standard. Another contributing factor is the use of polychromatic light in our evaluation of IOL performance. By contrast, the optical bench used by Yu et al employed a 546 nm light source, which is free of chromatic aberration effects and may therefore yield higher objective quality metrics.28 However, in agreement with our study, they found that the IPCL MTF levels gradually worsen with increasing apertures. This change was also seen in a prospective cohort study by Stodulka et al where highly myopic patients undergoing presbyopic treatment with IPCL had difficulty seeing under dim light conditions.17 They found the mean uncorrected distance visual acuity (UDVA) to be 0.11logMAR, with uncorrected near visual acuity (UNVA) improving to J1 for 15 of 17 eyes as the other 2 eyes were J1 at baseline. Schmid and Luedtke retrospectively studied the use of IPCL for presbyopia treatment in 16 eyes of 8 patients and found 9 out of 16 to be emmetropic with UDVA of at least 0.1logMAR with no need for reading glasses at one-month post-operation.14 Similarly, in our study, with apertures of 3.0 and 4.5mm, we respectively found the simulated VA to be −0.01logMAR and 0.07logMAR at distance. At the near focus, ie, at −2D, we found simulated VA to be 0.03 and 0.16logMAR for the two apertures respectively, which may show a lack of need for reading glasses. Overall, based on our and other studies, we can conclude that IPCL for the treatment of presbyopia can result in significantly improved near and far distances, but the len’s design appears to be susceptible to pupil-size changes.
The Artiplus lens studied is currently being clinically investigated by Güel et al as part of a prospective non-controlled multicenter clinical trial.18 The one-year clinical trial has shown that at 6 months post-operation, mean monocular UDVA, uncorrected intermediate VA (UIVA) at 80cm, and UNVA at 40cm were 0.01±0.08, 0.03±0.08, and 0.07±0.09logMAR respectively, with binocular UDVA, UIVA, and UNVA being −0.06±0.08, −0.01±0.07, and 0.02±0.08logMAR respectively.34 The results of this study appear to agree with ours for far and intermediate, but not fully for near distance. With the 3mm aperture, we found the simulated VA to be approximately −0.02, 0.06, and 0.12 logMAR at far, intermediate, and near focuses (respectively 0, −1.25, and −2.5 defocus values). It is important to note; however, that our results simulate the scenario of complete accommodation loss, which can differ from real-world clinical cases. In practice, the loss of accommodation is a gradual process, and patients receiving such lenses often retain some ability to accommodate.35 Laboratory studies thus can predict the maximum lens-related depth-of-focus improvement that patients may experience at various distances, with possibly better outcomes for those whose lenses may still have residual accommodation.
Lastly, our work did not study the EVO Visian Implantable Collamer Lens by STAAR Surgical (Monrovia, California, USA). This lens is a collagen and poly-hydroxyethyl methacrylate iris-fixated refractive phakic IOL with dioptric powers ranging from −0.5 to –18.0D.36 It has a plate-haptic design with a central convex/concave optical zone ranging from 4.9 to 5.8mm diameter and a 0.36mm diameter central port allowing aqueous flow.36,37 The STAAR phakic IOL for the treatment of presbyopia has been studied prospectively by Rateb et al showing uncorrected VA improving from 1.3±0.06logMAR to 0.76±0.2logMAR post-operatively.38 Alfonso et al studied the STAAR lens to correct moderate to high myopia and presbyopia and found postoperative UDVA and corrected DVA (CDVA) values of 0.09 ± 0.19 and 0.02 ± 0.03logMAR, following bilateral implantation in 40 patients.39 To be able to offer a comprehensive review of phakic IOL options available for patients with presbyopia, future studies comparing the STAAR phakic IOL to the Artiplus and IPCL phakic IOLs can be significantly beneficial.
In addition to the range of vision, which typically distinguishes presbyopia-correcting IOL solutions, another key differentiating factor is the occurrence and severity of photic phenomena. These unwanted light effects involve the perception of glare, halos, or starbursts when looking at light sources, such as streetlights or headlights of cars at night.40 In studying presbyopia-correcting IOLs, literature has found photic phenomena to greatly vary between lens types, and to be one of the most common complaints of patients undergoing IOL procedures – as high in 32.9% of eyes found by de Vries et al.40,41 Generally, a lower incidence of photic phenomena has been associated with the refractive rather than the diffractive principle in the context of multifocal IOLs implanted into the capsular bag.42 It is of interest to confirm whether this can also be observed in the context of phakic multifocal IOLs. Therefore, by studying photic phenomena rates with phakic IOLs and their comparison to other methods of presbyopia treatment, we can gather more information on the rate of side effects associated with phakic IOLs, which warrants further clinical and laboratory investigations. Additionally, due to the limitation of the OptiSpheric setup, this study did not evaluate the effects of IOL decentration or tilt on the IOL performance– factors that have been shown to impact visual outcomes resulting in symptoms such as glare or visual halos.43,44 Future studies on the impact of tilt and decentration on phakic IOL outcomes may add insights into the side effects of such IOLs.
Conclusion
Our study evaluated and contrasted the optical quality of diffractive versus refractive phakic IOL models – IPCL with added power of 2.5D and Artiplus – for the management of presbyopia at near, intermediate, and far distances simulating various pupil sizes. We found that both IPCL and Artiplus can effectively expand the range of vision, potentially alleviating visual symptoms in presbyopic patients and restoring vision at intermediate and near distances. Although the optical quality of both models was comparable at a 3mm pupil size, an increase to 4.5mm led to reduced defocus tolerance, with the IPCL model appearing more affected. While our study aids in directly comparing the two models and choosing a phakic IOL more appropriate based on patients’ individualized needs, it still needs to be considered that lens performance may differ under in vivo conditions due to the interaction between the IOL optics and the eye’s intrinsic aberrations and residual accommodation. Future studies evaluating the impact of these aspects and the perception of photic phenomena in presbyopic patients undergoing phakic IOL implantation can provide physicians and patients with a more comprehensive understanding of their treatment options.
Abbreviations
BSS, balanced salt solution; CDVA, corrected distance visual acuity; D, diopters; IPCL, implantable phakic contact lens; IOL, intraocular lens; MTF, modulation transfer function; MTFa, area under the modulation transfer function; TF MTF, through-focus modulation transfer function; UDVA, uncorrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected near visual acuity; VA, visual acuity.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by a research grant from OPHTEC BV, Groningen, The Netherlands. The David J Apple Laboratory receives support from the Klaus Tschira Foundation, Heidelberg, Germany.
Disclosure
GU Auffarth reports grants, personal fees, non-financial support and consulting fees from Afidera, Johnson&Johnson and Alcon, grants, personal fees, and non-financial support from Carl Zeiss Meditec, Hoya, Kowa, Oculentis/Teleon, Rayner, Santen, Sifi, Ursapharm, grants, and personal fees from Biotech, Oculus, EyeYon grants from Acufocus, Anew, Contamac, Glaukos, Physiol, Rheacell, outside the submitted work. The University of Heidelberg holds a patent application (No. WO2024/023230) entitled “Lens with extended depth of focus by inducing an excess of longitudinal chromatic aberration,” with GU Auffarth and G Łabuz as inventors. G Łabuz reports non-financial support from Contamac outside the submitted work. R Khoramnia reports grants, personal fees, and non-financial support from Alcon, Johnson&Johnson, Hoya, Physiol, Rayner, personal fees, and non-financial support from Kowa, Ophtec, Oculentis/Teleon, Santen, Staar, 1stQ, BVI, Zeiss, SIFI, and Acufocus, outside the submitted work. The remaining authors have nothing to disclose.
References
1. Frick KD, Joy SM, Wilson DA, Naidoo KS, Holden BA. The global burden of potential productivity loss from uncorrected presbyopia. Ophthalmology. 2015;122(8):1706–1710. doi:10.1016/j.ophtha.2015.04.014
2. Schwiegerling J. Refractive and diffractive principles in presbyopia-correcting IOLs – an optical lesson. Available from: https://us.alconscience.com/sites/g/files/rbvwei1736/files/pdf/Refractive-and-Diffractive-Principles-in-Presbyopia-Correcting-IOLs-An-Optical-Lesson-US-REF-1900001.pdf.
Accessed .August 14 , 20253. Namdev V, Kaur M, Sharma VK, Mulay A, Raj R, Titiyal JS. Current paradigms in refractive surgery. Med J Armed Forces India. 2024;80(5):497–504. doi:10.1016/j.mjafi.2024.08.003
4. Kumar K, Kohli P, Babu N, Khare G, Ramasamy K. Incidence and management of rhegmatogenous retinal detachment after pars plana vitrectomy and sutureless scleral-fixated intraocular lens. Indian J Ophthalmol. 2020;68(7):1432–1435. doi:10.4103/ijo.IJO_1974_19
5. Jafarinasab M, Kalantarion M, Hooshmandi S, et al. Indications and outcomes of intraocular lens exchange among pseudophakic eyes in a Tertiary Referral Center. BMC Ophthalmol. 2023;23(1):127. doi:10.1186/s12886-023-02871-y
6. Rodríguez-calvo-de-mora M, Rocha-de-lossada C, Rodríguez-Vallejo M, Zamora-de-la-cruz D, Fernández J. Retinal detachment after refractive lens exchange: a narrative review. Archivos de la Sociedad Española de Oftalmología. 2023;98(9):507–520. doi:10.1016/j.oftale.2023.06.013
7. Vasavada V, Srivastava S, Vasavada SA, Sudhalkar A, Vasavada AR, Vasavada VA. Safety and efficacy of a new phakic posterior chamber IOL for correction of myopia: 3 years of follow-up. J Refract Surg. 2018;34(12):817–823. doi:10.3928/1081597X-20181105-01
8. Kamiya K, Shimizu K, Igarashi A, et al. Posterior chamber phakic intraocular lens implantation: comparative, multicentre study in 351 eyes with low-to-moderate or high myopia. Br J Ophthalmol. 2018;102(2):177–181. doi:10.1136/bjophthalmol-2017-310164
9. Sachdev GS, Singh S, Ramamurthy S, Rajpal N, Dandapani R. Comparative analysis of clinical outcomes between two types of posterior chamber phakic intraocular lenses for correction of myopia and myopic astigmatism. Indian J Ophthalmol. 2019;67(7):1061–1065. doi:10.4103/ijo.IJO_1501_18
10. Pérez-Vives C, Ferrer-Blasco T, Cerviño-Expósito A, Madrid-Costa D, Montés-Micó R. Simulated prototype of posterior chamber phakic intraocular lens for presbyopia correction. J Cataract Refract Surg. 2015;41(10):2266–2273. doi:10.1016/j.jcrs.2015.10.050
11. Ferraz CA, Allemann N, Chamon W. Phakic intraocular lens for presbyopia correction. Arq Bras Oftalmol. 2007;70(4):603–608. doi:10.1590/s0004-27492007000400009
12. Alió JL, Mulet ME. Presbyopia correction with an anterior chamber phakic multifocal intraocular lens. Ophthalmology. 2005;112(8):1368–1374. doi:10.1016/j.ophtha.2005.02.029
13. Baïkoff G, Matach G, Fontaine A, Ferraz C, Spera C. Correction of presbyopia with refractive multifocal phakic intraocular lenses. J Cataract Refract Surg. 2004;30(7):1454–1460. doi:10.1016/j.jcrs.2003.12.051
14. Schmid R, Luedtke H. A novel concept of correcting presbyopia: first clinical results with a phakic diffractive intraocular lens. Clin Ophthalmol. 2020;14:2011–2019. doi:10.2147/OPTH.S255613
15. Bianchi GR, Paredes A, Puccio B, Parra-Hernández A. Implantable phakic contact lens: vault evaluation 5 years postoperatively. J Cataract Refract Surg. 2024;50(10):1000–1005. doi:10.1097/j.jcrs.0000000000001496
16. Takahashi M, Kamiya K, Shoji N, Kato S, Igarashi A, Shimizu K. Intentional undercorrection by implantation of posterior chamber phakic intraocular lens with a central hole (Hole ICL) for early presbyopia. Biomed Res Int. 2018;2018:6158520. doi:10.1155/2018/6158520
17. Stodulka P, Slovak M, Sramka M, Polisensky J, Liska K. Posterior chamber phakic intraocular lens for the correction of presbyopia in highly myopic patients. J Cataract Refract Surg. 2020;46(1):40–44. doi:10.1097/j.jcrs.0000000000000033
18. Truong D. Ophtec’s artiplus shows promising one-year clinical results. CAKE. 2024. Available from: https://cakemagazine.org/ophtecs-artiplus-shows-promising-one-year-clinical-results/.
Accessed .November 1 , 202419. Artiplus. Available from: https://www.ophtec.com/product-overview/artiplus.
Accessed .November 2 , 202420. Care Group. Available from: https://caregroupiol.com/products/phakic-lenses/ipcl/.
Accessed .November 2 , 202421. Spectrum Ophthalmics. IPCL – the customised refractive solution. Available from: https://www.spectrumophthalmics.uk/app/uploads/2022/08/IPCL-Presbyopic-Surgeons-Brochure.pdf.
Accessed .August 14 , 202522. Wang L, Dai E, Koch DD, Nathoo A. Optical aberrations of the human anterior cornea. J Cataract Refract Surg. 2003;29(8):1514–1521. doi:10.1016/s0886-3350(03)00467-x
23. Du C, Wang J, Wang X, Dong Y, Gu Y, Shen Y. Ultrasound biomicroscopy of anterior segment accommodative changes with posterior chamber phakic intraocular lens in high myopia. Ophthalmology. 2012;119(1):99–105. doi:10.1016/j.ophtha.2011.07.001
24. Łabuz G, Yan W, Baur ID, Khoramnia R, Auffarth GU. Chromatic aberration and spectral dependency of extended-range-of-vision intraocular lens technology. Sci Rep. 2023;13(1):14781. doi:10.1038/s41598-023-41634-z
25. ISO 11979-2:2014. ISO. Available from: https://www.iso.org/standard/55682.html.
Accessed .October 10 , 202426. TRIOPTICS GmbH. Technische Daten OptiSpheric® AF 500. INV; 2019. Available from: www.trioptics.com.
Accessed .August 14 , 202527. Son HS, Tandogan T, Liebing S, et al. In vitro optical quality measurements of three intraocular lens models having identical platform. BMC Ophthalmol. 2017;17:108. doi:10.1186/s12886-017-0460-0
28. Lee Y, Łabuz G, Son HS, Yildirim TM, Khoramnia R, Auffarth GU. Assessment of the image quality of extended depth-of-focus intraocular lens models in polychromatic light. J Cataract Refract Surg. 2020;46(1):108–115. doi:10.1097/j.jcrs.0000000000000037
29. Łabuz G, Papadatou E, Khoramnia R, Auffarth GU. Longitudinal chromatic aberration and polychromatic image quality metrics of intraocular lenses. J Refract Surg. 2018;34(12):832–838. doi:10.3928/1081597X-20181108-01
30. Łabuz G, Auffarth GU, Knorz MC, Son HS, Yildirim TM, Khoramnia R. Trifocality achieved through polypseudophakia: optical quality and light loss compared with a single trifocal intraocular lens. J Refract Surg. 2020;36(9):570–577. doi:10.3928/1081597X-20200715-01
31. Łabuz G, Son HS, Naujokaitis T, Yildirim TM, Khoramnia R, Auffarth GU. Laboratory Investigation of Preclinical Visual-Quality Metrics and Halo-Size in Enhanced Monofocal Intraocular Lenses. Ophthalmol Ther. 2021;10(4):1093–1104. doi:10.1007/s40123-021-00411-9
32. Alarcon A, Canovas C, Rosen R, et al. Preclinical metrics to predict through-focus visual acuity for pseudophakic patients. Biomed Opt Express. 2016;7(5):1877–1888. doi:10.1364/BOE.7.001877
33. Yu C, Kamiya K, Kawamorita T. Modulation transfer function of implantable phakic intraocular contact lens (IPCL) for myopia and presbyopia. Graefes Arch Clin Exp Ophthalmol. 2024;262(10):3201–3206. doi:10.1007/s00417-024-06539-1
34. Ophtec. Artiplus Model 470. Available from: https://www.ophtec.com/product-overview/artiplus.
Accessed .October 30 , 202435. Pérez-Prados R, Piñero DP, Pérez-Cambrodí RJ, Madrid-Costa D. Soft multifocal simultaneous image contact lenses: a review. Clin Exp Optometry. 2017;100(2):107–127. doi:10.1111/cxo.12488
36. STAAR Surgical. EVO Visian Implantable Collamer Lens; 2021. Available from: https://edfu.staar.com/edfu/5c784538fd5dd20001d67c89/ICL%20eDFU’s/eDFU-0016_Rev_01_EVO%20Visian%20ICL.pdf.
Accessed .August 14 , 202537. Packer M. Evaluation of the EVO/EVO+ sphere and toric visian ICL: six month results from the United States Food and Drug Administration Clinical Trial. Clin Ophthalmol. 2022;16:1541–1553. doi:10.2147/OPTH.S369467
38. Rateb M, Gad AAM, Tohamy D, Elmohamady MN. A prospective comparative study between implantable phakic intraocular contact lens and implantable Collamer lens in treatment of myopia in adults. J Ophthalmol. 2022;2022:9212253. doi:10.1155/2022/9212253
39. Alfonso JF, Fernández-Vega-Cueto L, Lisa C, Alfonso-Bartolozzi B, Palacios A, Madrid-Costa D. Clinical and aberrometric outcomes of a new implantable Collamer lens for myopia and presbyopia correction in phakic patients. J Refract Surg. 2023;39(9):589–596. doi:10.3928/1081597X-20230726-02
40. Ukai Y, Okemoto H, Seki Y, et al. Quantitative assessment of photic phenomena in the presbyopia-correcting intraocular lens. PLoS One. 2021;16(12):e0260406. doi:10.1371/journal.pone.0260406
41. de Vries NE, Webers CAB, Touwslager WRH, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859–865. doi:10.1016/j.jcrs.2010.11.032
42. Łabuz G, Khoramnia R, Naujokaitis T, Auffarth GU. Optical benchtop evaluation of special intraocular lens optics. Ophthalmologie. 2024;121(9):698–705. doi:10.1007/s00347-024-02064-y
43. Ashena Z, Maqsood S, Ahmed SN, Nanavaty MA. Effect of intraocular lens tilt and decentration on visual acuity, dysphotopsia and wavefront aberrations. Vision. 2020;4(3):41. doi:10.3390/vision4030041
44. Chen XY, Wang YC, Zhao TY, et al. Tilt and decentration with various intraocular lenses: a narrative review. World J Clin Cases. 2022;10(12):3639–3646. doi:10.12998/wjcc.v10.i12.3639
Continue Reading
-
Pakistan hits back at India’s ‘recycled lies’ on Kashmir at UN – samaa tv
- Pakistan hits back at India’s ‘recycled lies’ on Kashmir at UN samaa tv
- ‘Worst violator’: India slams ‘highly hypocritical’ Pakistan at UN; calls out killings in Afghanistan Times of India
- Fountainhead Of Terror: Why India Blasts Pakistan…
Continue Reading
-

Saudi national team ready for Iraq in Final Group B AFC playoff qualifying match
– Advertisement –
– Advertisement –
– Advertisement –
Jeddah, Oct 14 (SPA/APP): The Saudi national football team held its final training on Monday ahead of Tuesday’s match against Iraq at King Abdullah Sports City in Jeddah, the final Group…
Continue Reading
-
Ancient microbes thawed from Alaskan permafrost after 40,000 years – Mid-day
- Ancient microbes thawed from Alaskan permafrost after 40,000 years Mid-day
- Scientists ‘reawaken’ ancient microbes from permafrost — and discover they start churning out CO2 soon after Live Science
- Ancient Alaska microbes’ thaw helps…
Continue Reading
-

World’s first IVF baby backs fertility mission as global birth rates fall
Sammy JenkinsWest of England
 Leon Neal/Getty Images
Leon Neal/Getty ImagesLouise Brown was the first to be born via IVF in 1978 The world’s first IVF baby has given her backing to an international fertility care campaign.
Louise Brown, 47, from Bristol, was the first in the world to be born via in vitro fertilisation (IVF) at Oldham General Hospital on 25 July 1978.
Ms Brown is now working with the International Federation of Fertility Societies (IFFS) on their More Joy campaign, a movement pushing for affordable, fair and accessible fertility care globally.
“In my school days, sex education lessons were all about avoiding pregnancy. This initiative is teaching people how to build healthy families and protect their fertility,” Ms Brown said.
Ms Brown said she was “really proud” to be supporting the campaign and her experience of travelling to reproductive health conferences internationally has allowed her to see “first hand” how fertility treatments can “make a real difference” to falling birth rates”.
In June, Dr Natalia Kanem, head of the United Nations Population Fund (UNFPA), said world fertility rates were in an “unprecedented decline”, due to a number of factors, including the prohibitive cost of parenthood.
Surveying 14,000 people in 14 countries about their fertility intentions, the UNFPA found one in five people haven’t had or expect they won’t have their desired number of children.
In total, 12% cited infertility – or difficulty conceiving – as a reason for not having the number of children they wanted.
However, the figure was higher in some countries including Thailand (19%), the US (16%), South Africa (15%), Nigeria (14%) and India (13%).
Meanwhile, In 2024, figures from the Office for National Statistics showed the lowest fertility rate on record in England and Wales, with women having on average of 1.44 children between 2022 and 2023.
‘Support they need’
IFFS president Marcos Horton said the organisation, which was established in 1968 and brings together fertility specialists worldwide, said while “fertility is a fundamental part of human health”, many “face barriers in accessing care”.
He said the campaign aims to “make fertility care more accessible and equitable, while also educating people about infertility prevention and healthy family planning”.
“With ambassadors like Louise, we can raise awareness internationally, influence policy, and ensure that more people have the support they need to start a family when they are ready,” he added.
Continue Reading
-

Diver thought to have identified wreck of steamship lost in 1869
 DeepWreckDiver/Youtube
DeepWreckDiver/YoutubeDominic Robinson explored the wreck last September A deep-sea diver believes he has solved the mystery of a cargo vessel which disappeared more than 150 years ago.
Dominic Robinson, from Plymouth, said he discovered crockery…
Continue Reading