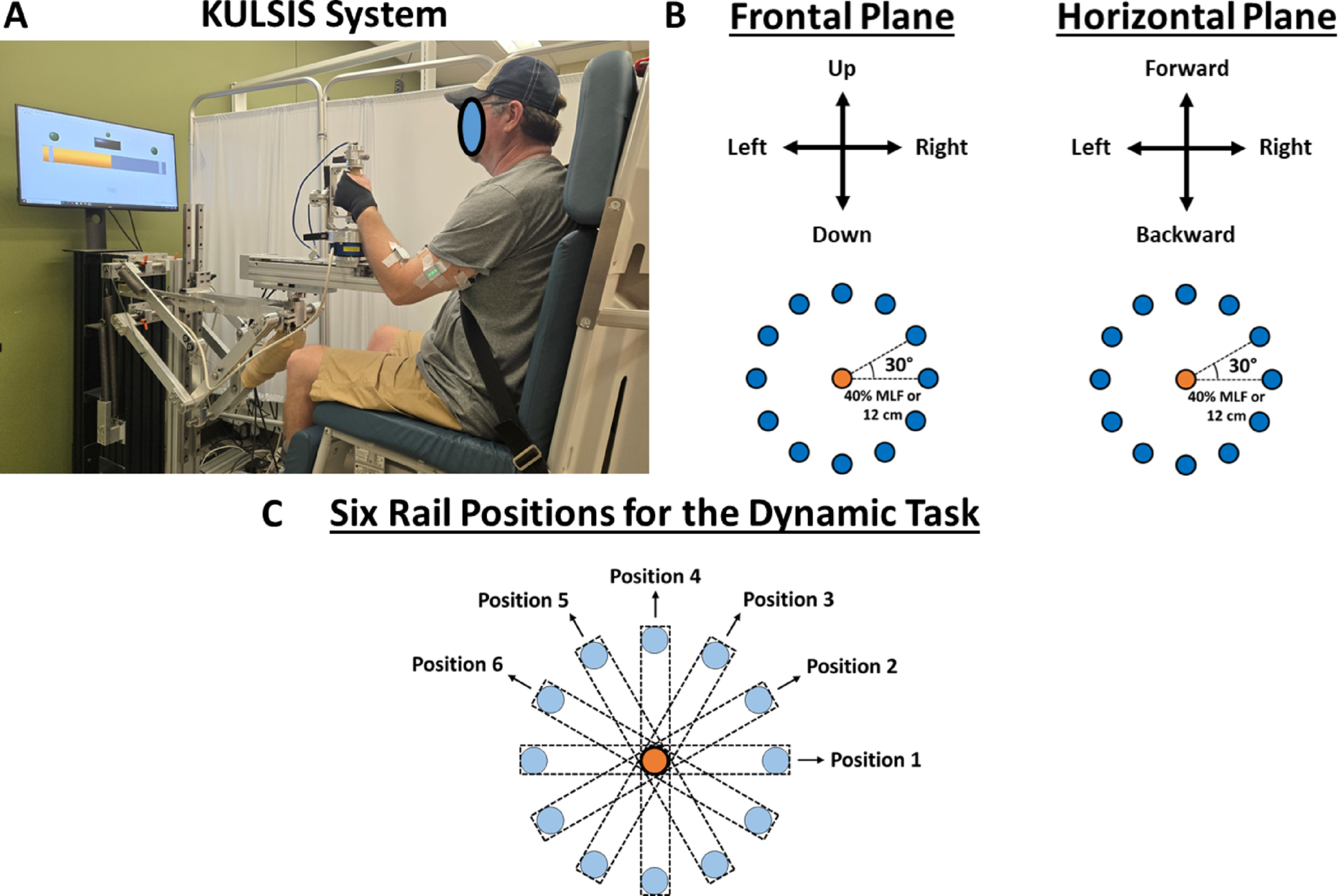
The primary aim of this study was to investigate the generalizability of muscle synergy characteristics between isometric force generation and dynamic reaching tasks after stroke. In the isometric task, the force load for the target-matching task was set at 40% of each participant’s MLF. MLF was significantly higher in healthy participants [40.13 ± 14.14 N (mean ± SD)] compared with stroke survivors (24.07 ± 12.03 N; p < 0.01). The mean isometric target-matching time for each participant, including the ramp and the one-second holding phases, was longer for stroke survivors (6.14 ± 1.91 s) than for healthy individuals (4.63 ± 0.93 s), although this difference was not statistically significant (p = 0.052). In the dynamic reaching task, the average of each participant’s time from the target-onset to the initial timing of a target match was significantly lower for healthy individuals (1.71 ± 0.16 s) compared with stroke survivors (2.02 ± 0.09 s; p < 0.01). For both tasks, healthy participants matched all the targets, while stroke survivors matched, on average, 85.81% and 96.6% of the targets for the isometric and dynamic reaching, respectively, mainly because of the difficulty in holding the target match for one second in the isometric task. The average experiment duration was 2.5 h and 3.5 h for healthy volunteers and stroke survivors, respectively.
EMG patterns of two-dimensional isometric force generation and dynamic reaching
The EMG signals recorded in neurologically intact volunteers and stroke survivors showed distinct muscle activity underlying isometric force generation and dynamic reaching. For instance, Fig. 2 shows the EMG patterns from two participants (a healthy, representative volunteer and a moderately impaired stroke survivor) performed during static and dynamic tasks in a medial direction target in the horizontal plane. The healthy volunteer mainly recruited AD, MD, and PEC during the isometric force generation trial (Fig. 2A), while BRD, BB, AD, and PEC were activated during the dynamic reaching (Fig. 2B). In contrast, the moderately impaired stroke participant mainly recruited BB and PEC during the static trial, while mainly PEC, with some activation of AD and BB, was recruited for the dynamic trial. Over time, the EMG signal magnitudes varied between the two tasks for both participants. Moreover, alterations in the EMG patterns were typically observed in stroke survivors, varying by individuals and depending on the level of motor impairment.
Optimal number of muscle synergies in isometric force generation and dynamic reaching tasks
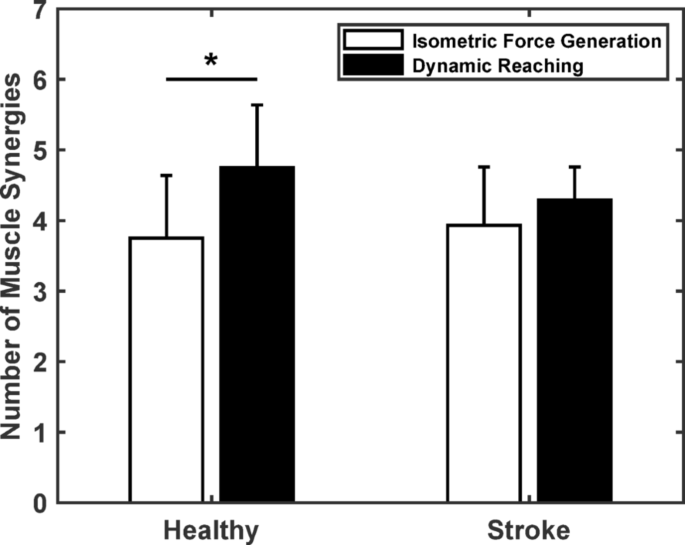
The number of muscle synergies required to explain EMG variance differed between tasks in healthy individuals but remained consistent in stroke survivors. Figure 3 shows the average number of muscle synergies for both groups across the two tasks. Based on the criteria described in the previous section (see Method section, Muscle Synergy Identification), on average, four synergies (3.75 ± 0.89; mean ± SD) were required to account for the variance of the EMG underling the isometric force generation in the healthy individuals (n = 8), while five synergies (4.75 ± 0.83) were required for the dynamic reaching task in the same group. Similarly, for the stroke survivors (n = 14), four synergies were typically required for both tasks, isometric force generation (3.93 ± 0.83) and dynamic reaching (4.29 ± 0.47). A significant difference was found in the optimal number of muscle synergies in the healthy group between tasks (paired t-test, p < 0.05), but not in the stroke population. Finally, no significant relationship or trend was observed between the number of synergies and the level of motor impairment after stroke in either task.
Muscle synergy patterns
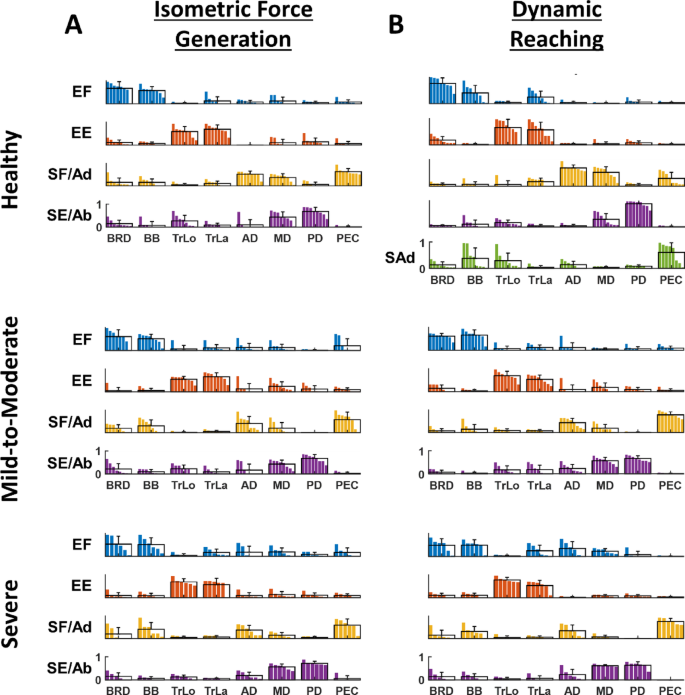
Muscle synergy patterns were consistent across both isometric force generation (Fig. 4A) and dynamic reaching (Fig. 4B) tasks within each subgroup, including healthy individuals, and the stroke subgroups with mild-to-moderate, and severe motor impairment. As a validation, a post hoc analysis was applied to a subset of the data collected (eight stroke survivors and four healthy individuals) to compare muscle synergy composition identified from the holding period only and from the ramp phase plus holding period. Consistent with our previous study in stroke [28], synergy patterns were similar between different phases during the isometric force generation task. The synergy patterns were named following the appropriate mechanical action of the muscles mainly activated within each synergy. The muscle synergies of the healthy participants activated during both isometric force generation and dynamic reaching tasks were as follows: elbow flexor (EF), elbow extensor (EE), shoulder flexor/adductor (SF/Ad), and shoulder extensor/abductor (SE/Ab). The fifth synergy of dynamic reaching was named shoulder adductor (SAd) because of its functional activation during the task performance. The EF synergy included the activation of the elbow flexor muscles (BRD and BB). The EE synergy consisted of the activation of the elbow extensor muscles (TrLo and TrLa). The SF/Ad consisted of the activation of AD, MD, and PEC. The SE/Ab synergy contained the activation of MD and PD. The SAd synergy contained the activation of PEC with some activation of BB.
Similarly, the muscle synergies from the two stroke subgroups (mild-to-moderate and severe) included: EF, EE, SF/Ad, and SE/Ab. However, systematic alterations were observed in stroke participants, especially in severely impaired subgroups. The EF synergies mainly consisted of BRD and BB, with some co-activation of TrLa, AD, and MD for the two tasks. In addition, SF/Ad synergies mainly consisted of PEC with an abnormal reduction of AD and MD, and an atypical co-activation with BB for the severely impaired subgroup.
Within-subject similarity of muscle synergy composition between isometric force generation and dynamic reaching tasks
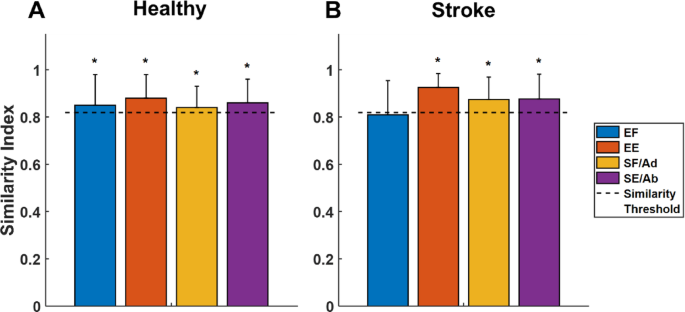
The majority of the synergies were statistically similar (threshold [r] = 0.819; p < 0.05) between isometric force generation and dynamic reaching within each individual of each subgroup (Fig. 5). In healthy individuals, all four muscle synergies were significantly similar between the two tasks. For instance, in the EF and EE synergies, the similarity indices [mean ± SD] were 0.85 ± 0.13 and 0.88 ± 0.10, respectively. Also, the similarity indices of the SF/Ad and SE/Ab synergies were 0.84 ± 0.09 and 0.86 ± 0.10, respectively. In addition, in the stroke group, three out of the four identified synergies were similar, including EE, SF/Ad, and SE/Ab synergies. The elbow flexor synergy was not statistically similar between the two tasks, mainly because of the greater variability in the muscle weights of the elbow flexor muscles (BRD and BB) with an elbow extensor (TrLa) and a shoulder adductor (AD) within the same participant across both tasks, particularly observed in severely impaired stroke survivors.
Altered, stroke-induced synergies explained as merging of synergies of healthy individuals
Altered, stroke-induced muscle synergies observed during both isometric force generation and dynamic reaching were explained as a linear combination of muscle synergies underlying dynamic reaches of healthy participants. The mean of muscle synergies underlying dynamic reaching in the healthy group formed the norm (model) synergies. The scalar products of the best-matched synergy pairs between the norm synergies and each stroke participant’s synergies underlying each motor task were calculated. Regarding the static task, 41 out of the 56 synergies (14 stroke survivors × 4 synergies per participant) of all the stroke participants were identified as preserved (i.e., the scalar product greater than the threshold (0.819); see Methods section, Calculating Muscle Synergy Similarities). Similarly, 42 out of the 56 synergies of the 14 stroke survivors were also identified as preserved during dynamic reaching. Moreover, by merging two norm (model) synergies observed from healthy individuals during the dynamic task, nine out of 13 altered, stroke-induced synergies in the isometric task, and 12 out of 14 altered synergies in the dynamic task were successfully reconstructed (i.e., the scalar products between the altered synergies and merged synergies were greater than the threshold). This finding indicates that merging or co-activation of synergies recruited during dynamic reaching in healthy conditions can largely account for abnormal synergy patterns observed after stroke across both static and dynamic motor tasks. In contrast, merging the model synergies underlying the isometric conditions could not reconstruct the same altered, stroke-induced synergies as much as merging the model synergies underlying the dynamic conditions (i.e., only less than half of the altered synergies were explained). This observation highlights that merging synergies underlying dynamic reaches of healthy individuals provides a better explanation of altered, stroke-induced muscle synergies than merging synergies underlying static tasks.
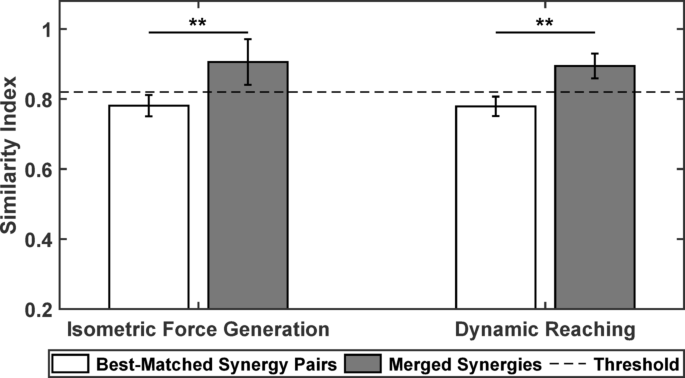
Finally, we assessed the impact of the merging on the similarity index and found that it consistently increased beyond the synergy similarity threshold (0.819), with values typically approaching 0.9. This increase in similarity was significant within each task, showing that merging dynamic synergies of healthy individuals closely resembled the altered muscle synergy patterns during both tasks (Fig. 6). Altered, stroke-induced synergies that could not be explained by merging as a linear combination of model synergies were not included in this analysis.
Differences in muscle synergy recruitment during isometric force generation and dynamic reaching
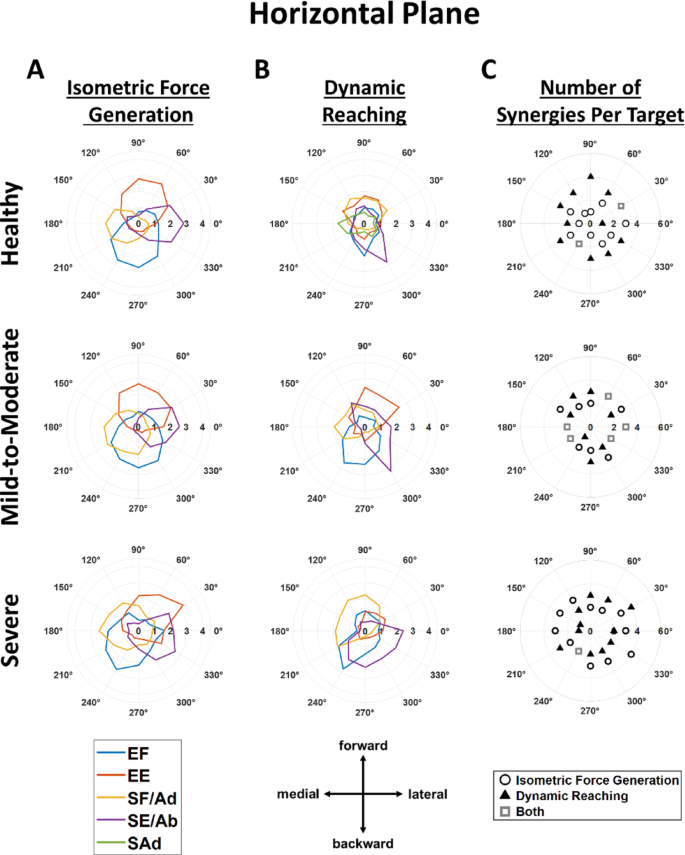
The static and dynamic tasks tended to adopt different muscle synergy recruitment strategies. These patterns were based on the averaged activation profiles within each subgroup, including healthy individuals, and mild-to-moderate and severe stroke subgroups. For visualization purposes, the 24 target directions were divided into two sets: one representing the 12 target directions from the horizontal plane (Fig. 7) and the other representing the 12 target directions from the frontal plane (Fig. 8). In the horizontal plane, synergy activation profiles appeared more directionally tuned during isometric force generation than during dynamic reaching across all subgroups, except for the severely impaired stroke subgroup (Fig. 7A vs. 7B). Furthermore, task-specific variations in synergy recruitment between isometric and dynamic motor control were reflected in terms of the number of synergies used per target direction. Healthy participants generally recruited one more muscle synergy per target direction in dynamic reaching than in isometric force generation in the horizontal plane; however, severely impaired stroke survivors generally recruited one more muscle synergy per target direction in isometric force generation than in dynamic reaching (Fig. 7C). No difference between the two tasks was observed in the stroke subgroup with mild-to-moderate motor impairment in the number of recruited synergies per target in the horizontal plane. For healthy individuals, the activation thresholds of isometric force generation (t_iso) and dynamic reaching (t_dyn) thresholds were t_iso_healthy = 1 and t_dyn_healthy = 0.88 in the healthy group, whereas for the stroke groups, they were t_iso_stroke = 0.88 and t_dyn_stroke = 0.85.
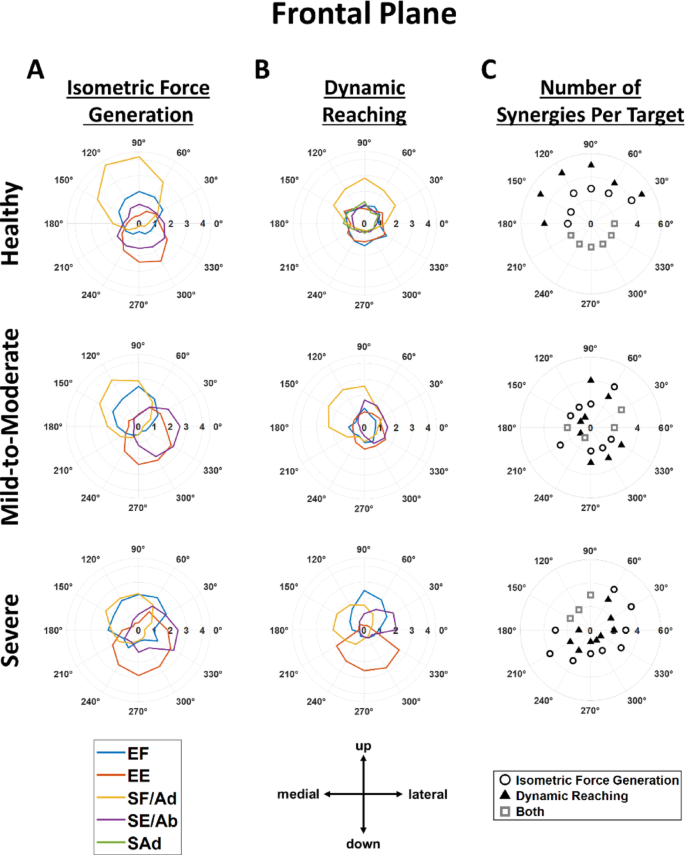
Similarly, Fig. 8 shows that the averaged activation profile of each muscle synergy was more tuned in the isometric force generation task (Fig. 8A) than in the dynamic reaching (Fig. 8B) in the frontal plane for healthy individuals, and stroke participants with mild-to-moderate impairment, but not for severely impaired stroke survivors. Meanwhile, during the dynamic reaching, several muscle synergies were activated per target direction for all subgroups, except for the severely impaired subgroup, suggesting that multiple synergies need to be activated to perform the desired point-to-point dynamic reaching in the healthy group as well as in the stroke subgroup with mild-to-moderate motor impairment. In addition, differences were observed in the number of muscle synergies significantly activated across the 12 target directions in the frontal plane. Healthy participants tended to recruit one more muscle synergy per target direction during the dynamic reaching than during the static task. Interestingly, severely impaired stroke survivors generally recruited one more muscle synergy per target direction during isometric force generation than during dynamic reaching (Fig. 8C). Consistent with the horizontal plane, no difference in the number of recruited synergies per target in the frontal plane was observed between the two tasks in the mild-to-moderate stroke subgroup.
Even though variability was observed across subgroups, the averaged synergy activation profiles as a function of the target force direction across both planes were generally aligned with the expected mechanical action of the muscles predominantly activated within each respective muscle synergy pattern. For instance, in the horizontal plane (Fig. 7A) during the isometric task across subgroups, the EF and EE synergies were mostly activated in the backward-medial and forward-lateral directions, respectively, whereas the SF/Ad and SE/Ab synergies were more active in the medial and lateral directions, respectively. Similarly, in the dynamic reaching, the activation of EF, EE, and SF/Ad in the healthy subgroup retained similar directional preferences, whereas the preferred activation of SE/Ab shifted toward a backward-lateral direction in the horizontal plane (Fig. 7B).
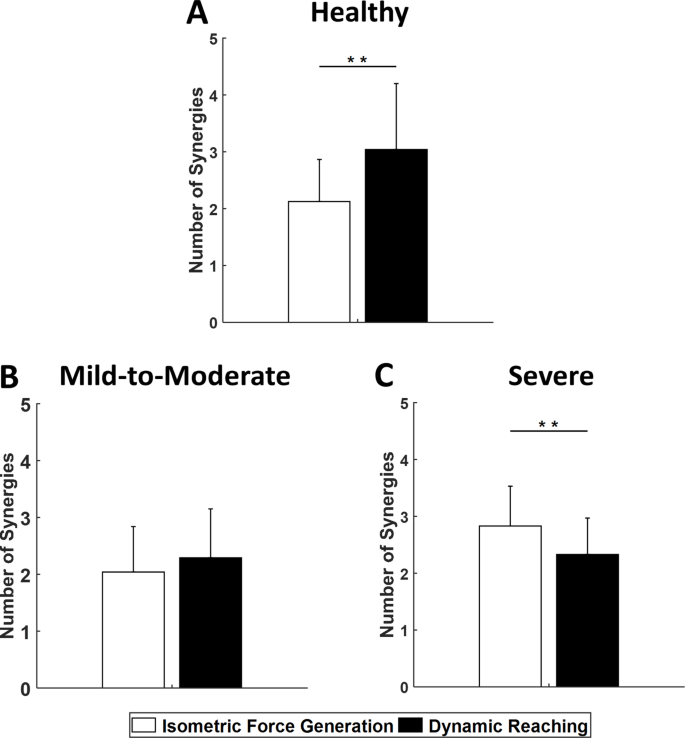
The number of average muscle synergies significantly activated per target direction, with both planes combined, varied between isometric force generation and dynamic tasks in healthy individuals and severely impaired stroke survivors. Figure 9 shows the number of synergies activated and averaged across the 24 targets (12 horizontal and 12 frontal) for the three subgroups. The Wilcoxon signed-rank test between corresponding subgroups across the two tasks showed a significant difference in the number of synergies activated across the 24 target directions in the healthy individuals, suggesting that the reaching task was more complex. Interestingly, for the severe stroke subgroup, a significant difference was also found, with the isometric task typically requiring one more synergy significantly activated per target direction than the dynamic task, suggesting abnormal muscle synergy recruitment strategies in the neuromuscular coordination of motor tasks in severely impaired stroke survivors. Finally, a post-hoc power analysis was conducted to assess the reliability of these within-subgroup comparisons between the two tasks, indicating a statistical power exceeding the standard 80% threshold.
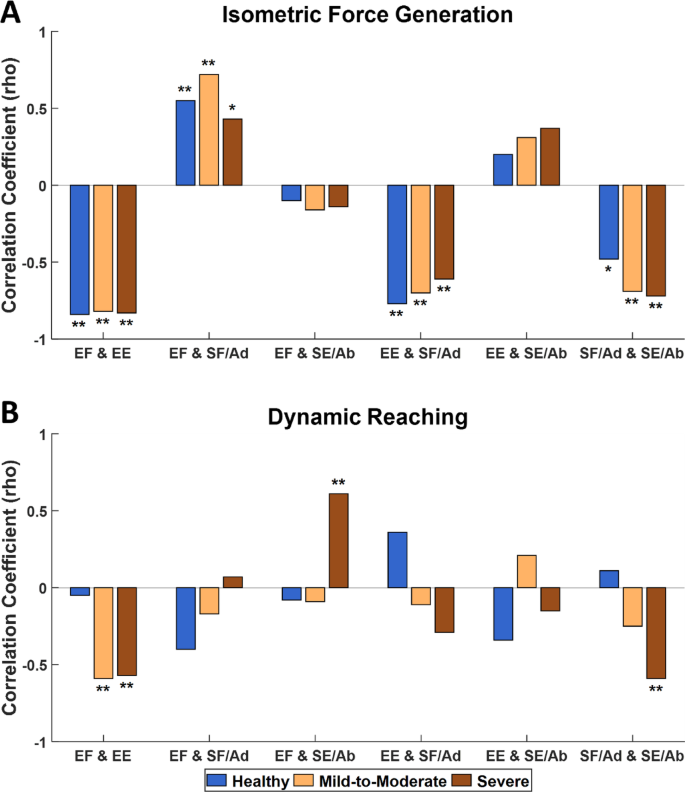
Correlation of a pair of synergy activation profiles
The trend in the correlation of any possible pairs of averaged synergy activation profiles was different between isometric force generation (Fig. 10A) and dynamic reaching (Fig. 10B) (Spearman’s rank correlation, p < 0.05). During the isometric task, the elbow flexor and extensor synergy activations were negatively correlated in healthy individuals (rho = − 0.84, p < 0.01) as well as in all two-stroke subgroups (rho = − 0.82, p < 0.01, mild-to-moderate; and rho = − 0.83, p < 0.01, severe). Additionally, the preservation of a negative correlation even after stroke was observed between the shoulder antagonistic synergies (SF/Ad and SE/Ab) for the healthy individuals (rho = − 0.48, p < 0.05) and the two-stroke subgroups (rho = − 0.69, p < 0.01, mild-to-moderate; and rho = − 0.72, p < 0.01, severe). Additionally, positive correlations between agonistic synergies across both arm joints (EF and SF/Ad) were consistently maintained for healthy individuals (rho = 0.55, p < 0.01) and the two stroke subgroups (rho = 0.72, p < 0.01, mild-to-moderate; and rho = 0.43, p < 0.05, severe). Finally, the negative correlations between antagonistic synergies across both arm joints (EE and SF/Ad) were found to be kept in the healthy group (rho = − 0.77, p < 0.01), and the two stroke subgroups (rho = − 0.70, p < 0.01, mild-to-moderate; and rho = − 0.61, p < 0.01, severe). These results suggest that the correlation between any possible pairs of the averaged synergy activation profiles within each subgroup remains preserved mainly in the isometric condition, even after stroke.
In contrast, in the dynamic condition, a significant negative correlation between elbow flexor and extensor synergy activations was not observed in the healthy individuals (rho = − 0.05, p = 0.82), but in the mild-to-moderate (rho = − 0.59, p < 0.01) and severe impaired (rho = − 0.57, p < 0.01) stroke subgroups. Similarly, the shoulder antagonistic synergies (SF/Ad and SE/Ab) did not exhibit a significant correlation for healthy (rho = 0.11, p = 0.59) and stroke survivors with mild-to-moderate impairment (rho = − 0.25, p = 0.25), but they did for severely impaired subgroups (rho = − 0.59, p < 0.01). Interestingly, in participants with severe motor impairment, positive coupling was identified between the elbow flexor and shoulder extensor/abductor synergies (rho = 0.61, p < 0.01).