- Over 70% of key bacteria resist standard treatments in Africa
- WHO urges urgent action to prevent global health crisis
Antibiotic resistance now affects one in five infections across Africa, surpassing the global average, where one in…

Antibiotic resistance now affects one in five infections across Africa, surpassing the global average, where one in…
Adjuvant therapy can feasibly yield circulating tumor DNA (ctDNA) clearance in a portion of patients with colorectal cancer (CRC) and postoperative ctDNA positivity, with clearance correlating with superior disease-free survival (DFS) outcomes, according to findings from the INTERCEPT CRC study presented at the
ctDNA dynamics data after the time of surgery or ablation revealed that 69% of patients had ctDNA negativity on all tests, while 18% had positive results on all tests. Additionally, 3.1% had ctDNA clearance on at least 2 tests, 2.4% had clearance on 1 test, and 8% converted from ctDNA negativity to positivity. Furthermore, adjuvant therapy resulted in ctDNA clearance among 26% (n = 20/77) of patients with ctDNA-positive results after surgery, with 13 (17%) having clearance on at least 2 tests.
From the time of first ctDNA-positive test result in the stage I to III CRC population, DFS outcomes were significantly improved among those with clearance on at least 2 tests (P <.0001). Data revealed similarly significant outcomes among patients with stage IV disease (P <.0001).
Following adjuvant therapy, 70% of patients had ctDNA negativity on all tests, while 19% had positive results on all tests. Other data showed that 1.5% had ctDNA negativity on at least 2 tests, 1.4% had clearance on 1 test, and 9% converted from ctDNA negativity to positivity.
The study population included 403 patients who had ctDNA-positive results at any time after surgery and adjuvant treatment, with 4.2% showing at least 1 subsequent negative reading without any intervention. Furthermore, 2.1% of this population had ctDNA-negative results on at least 2 sequential tests without any intervention, and 1.7% had no recurrences at the time of follow-up. Among patients with spontaneous ctDNA clearance, the median duration of clearance was 11.2 months, and the mean tumor molecules per milliliter was 0.06 (range, 0.02-1.89).
“Adjuvant treatment can clear a quarter of the patients [who] are ctDNA positive postoperatively. Those with ctDNA clearance had superior DFS,” presenting author Emerik Osterlund, MD, PhD, a postdoctoral fellow in Gastrointestinal Medical Oncology at The University of Texas MD Anderson Cancer Center, stated in the presentation.1 “The rate and durability of [spontaneous] ctDNA clearance was very low.”
According to Osterlund, previous studies have demonstrated how ctDNA can be employed to monitor minimal residual disease, with ctDNA positivity representing a strong risk factor for disease recurrence following procedures administered with curative intent.2 However, he noted limited findings on the rates and durability of spontaneous ctDNA clearance, the process of transitioning from ctDNA positivity to negativity without any intervention. Consequently, Osterlund and colleagues aimed to evaluate the behavior and clearance of ctDNA following procedures with curative intent among patients with stage I to IV CRC.
As part of the INTERCEPT program, 1301 patients with newly diagnosed or previously treated resectable stage I to IV CRC enrolled on the study, with 53% having stage I to III disease and 47% having stage IV disease. Patients received standard-of-care therapy—surgical resection with or without neoadjuvant and adjuvant treatment—and underwent tissue collection and testing via ctDNA assays in the postoperative setting and/or following therapy. Investigators then conducted routine surveillance via imaging & labs, with ctDNA assay testing occurring approximately every 3 months at each surveillance visit.
“ctDNA clearance is useful for seeing potential benefit in novel therapeutic studies,” Osterlund concluded.1

Sucker Punch has released a new patch for Ghost of Yōtei with numerous bug and crash fixes, including one that could rarely occur when using ray tracing.
Those who purchased the Digital Deluxe Edition but didn’t receive the Black Ghost Mask…
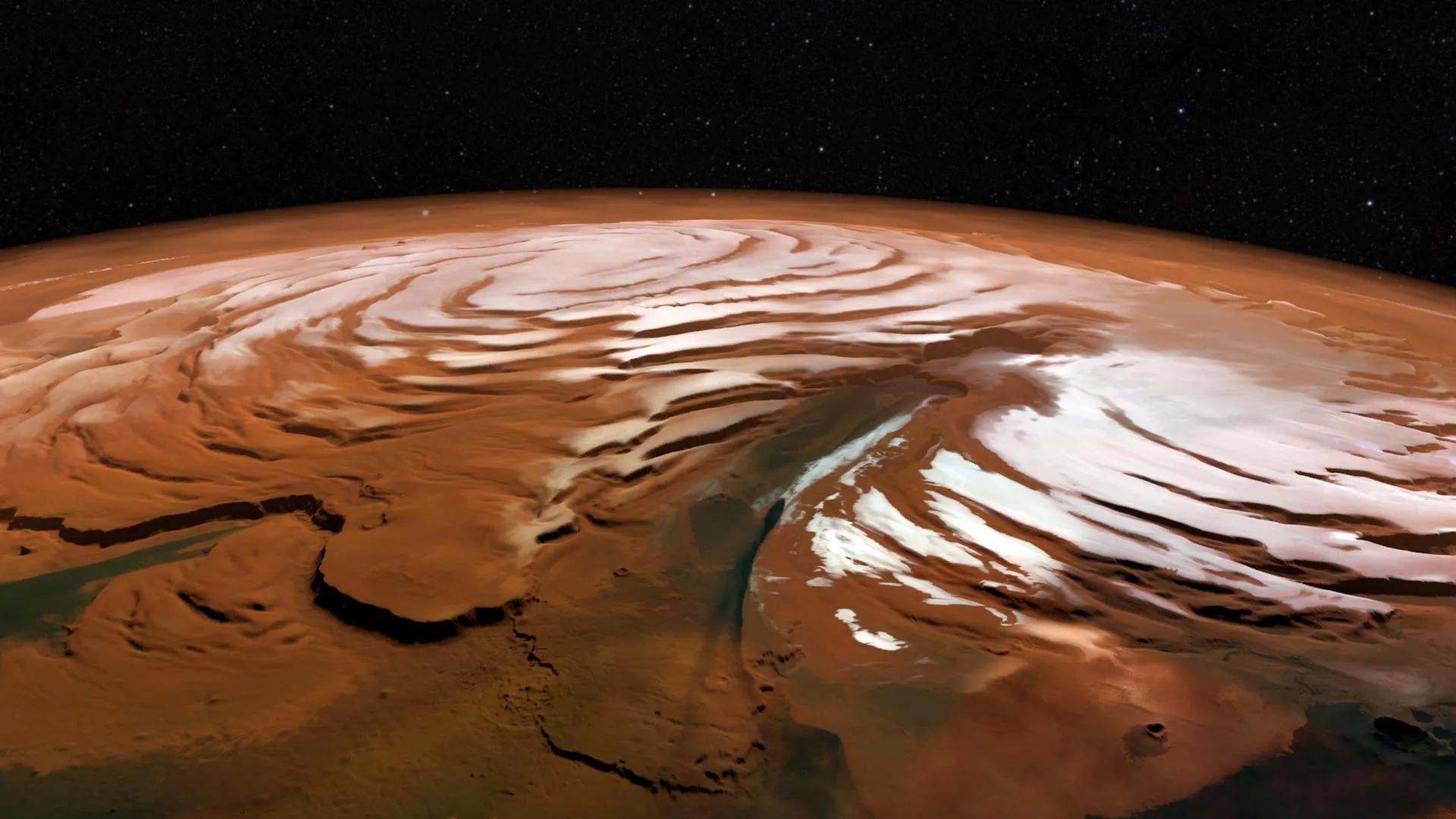
Scientists have recently captured a rare look at the harsh winter conditions swirling above Mars’ north pole. Inside the planet’s polar vortex, temperatures drop dramatically — much colder than the air outside — and the continuous darkness of…
If you wish you could live in the world of Fallout: New Vegas, then you may need Doc Mitchell to take a look at your brain.
However, if the allure of life on the irradiated New Vegas Strip appeals to you that much, you can get a little taste (this…

Relacorilant plus nab-paclitaxel (Abraxane) produced a progression-free survival (PFS) benefit vs nab-paclitaxel alone in a subgroup of patients with platinum-resistant ovarian cancer (PROC) who had received prior PARP inhibitor treatment, including those who had progressed during PARP inhibitor treatment, according to findings from a pre-planned subgroup analysis of the phase 3 ROSELLA trial (NCT05257408), which were presented at the
In the subgroup of patients who had prior exposure to a PARP inhibitor, relacorilant plus nab-paclitaxel (n = 114) elicited a median blinded independent central review (BICR)–assessed PFS of 7.36 months (95% CI, 5.59-8.18) vs 4.63 months (95% CI, 3.55-5.72) with nab-paclitaxel alone (n = 120; HR, 0.60; 95% CI, 0.42-0.85; nominal P = .0035). The investigator-assessed overall response rates (ORRs) in these respective groups were 39.5% and 30.8%.
Furthermore, in the subgroup of patients who had progressed on a prior PARP inhibitor, the BICR-assessed median PFS with relacorilant plus nab-paclitaxel (n = 86) was 7.36 months (95% CI, 5.39-8.44) vs 3.94 months (95% CI, 3.32-5.72) with nab-paclitaxel alone (n = 97; HR, 0.56; 95% CI, 0.37-0.84; nominal P = .0046). The investigator-assessed ORRs in these respective groups were 34.9% and 26.8%.
“Consistent benefit was reported in this subgroup analysis in PARP [inhibitor]–pretreated patients [with] relacorilant plus nab-paclitaxel,” presenting author Domenica Lorusso, MD, PhD, said.
Lorusso is director of the Gynaecological Oncology Unit at Humanitas Hospital San Pio X, as well as a full professor of obstetrics and gynecology at Humanitas University, Rozzano, in Milan, Italy.
Ovarian cancers harbor glucocorticoid receptor expression, which is a marker of poor prognosis. Relacorilant is a novel, selective glucocorticoid receptor antagonist that restores cancer sensitivity to cytotoxic chemotherapy.
ROSELLA enrolled patients with epithelial ovarian, primary peritoneal, or fallopian tube cancer who had an ECOG performance status of 0 or 1, had progressed less than 6 months after their last dose of platinum therapy, and had received 1 to 3 prior lines of therapy, including prior bevacizumab. Patients were randomly assigned 1:1 to receive nab-paclitaxel at 80 mg/m2 on days 1, 8, 15 of each 28-day cycle, in combination with relacorilant at 150 mg on the day before, the day of, and the day after nab-paclitaxel infusion; or nab-paclitaxel monotherapy at 100 mg/m2 on the same nab-paclitaxel dosing schedule.
PFS by BICR and overall survival (OS) served as the dual primary end points. Secondary end points included investigator-assessed PFS, ORR, duration of response, clinical benefit rate, and safety.
Previously, data presented at the
The addition of relacorilant to nab-paclitaxel also showed a trend toward improved OS among patients who had received a prior PARP inhibitor, although these data were only at 50% maturity at the time of this interim analysis.1 The median OS was 15.61 months (95% CI, 12.02-not reached) with relacorilant plus nab-paclitaxel vs 12.58 months (95% CI, 10.09-15.18) with nab-paclitaxel alone (HR, 0.77; 95% CI, 0.53-1.13; nominal P = .1834).
Lorusso noted that relacorilant plus nab-paclitaxel continued to be well tolerated in the prior PARP inhibitor subgroup. Any treatment-emergent adverse effects (TEAEs) were observed in all patients in this subgroup. Among safety-evaluable patients with prior PARP inhibitor exposure who received relacorilant plus nab-paclitaxel, grade 3 or higher TEAEs were seen in 71.1%, and serious AEs were reported in 31.6%. TEAE-related dose reductions of relacorilant (7.0%), dose reductions of nab-paclitaxel (46.5%), treatment interruptions (72.8%), and treatment discontinuations (8.8%) were also observed.
Among safety-evaluable patients with prior PARP inhibitor exposure who received nab-paclitaxel alone (n = 117), grade 3 or higher TEAEs were seen in 64.1%, and serious AEs were reported in 21.4%. TEAE-related dose reductions of nab-paclitaxel (29.1%), treatment interruptions (58.1%), and treatment discontinuations (6.8%) were also observed.
“The safety profile in the trial subgroup was very similar to that [seen in] the overall population,” Lorusso concluded.
Disclosures: Lorusso reported receiving grants from or having contracts with AstraZeneca, Clovis, Genmab, GSK, Immunogen, Incyte, MSD, Novartis, PharmaMar, Seagen, and Roche; receiving consulting fees from AstraZeneca, Clovis Oncology, Genmab, GSK, Immunogen, MSD, PharmaMar, Seagen, and Novartis; receiving payment or honoraria from AstraZeneca, Clovis, Corcept, Genmab, GSK, Immunogen, MSD, Oncoinvest, PharmaMar, Seagen, and Sutro; receiving support for attending meetings and/or travel from GSK, AstraZeneca, Clovis, and MSD; and participating on Data Safety Monitoring or Advisory Boards for AstraZeneca, Clovis, Corcept, Genmab, GSK, Immunogen, MSD, Oncoinvest, PharmaMar, Seagen, and Sutro.

First Fergana Peace Forum was organized from 15 to 16 October 2025 at Fergana university. More than 300 participants from Central Asia, the CIS, Europe, Asia and the America gathered to discuss under the title “Uniting efforts for peace…
HONG KONG, Oct. 19, 2025 /PRNewswire/ — On October 19, 2025, Akeso (9926.HK) announced the final analysis results from the COMPASSION-15/AK104-302 study at the 2025 European Society of Medical Oncology Congress (ESMO 2025) . COMPASSION-15 is a Phase III clinical trial evaluating cadonilimab, Akeso’s first-in-class PD-1/CTLA-4 bispecific antibody, in combination with oxaliplatin and capecitabine as first-line treatment for unresectable, locally advanced, recurrent, or metastatic gastric or gastroesophageal junction (G/GEJ) adenocarcinoma. Professor Shen Lin, principal investigator from Peking University Cancer Hospital, presented the findings in an oral session at ESMO 2025.
In this final analysis presented at ESMO 2025 (median follow-up: 33.9 months), the cadonilimab regimen demonstrated enhanced long-term survival benefits in first-line advanced G/GEJ adenocarcinoma. With the extended follow-up period and more mature data, the cadonilimab treatment regimen showed a further reduction in the risk of death compared to the control group. This consistent benefit was observed across all PD-L1 expression subgroups.
The interim analysis of COMPASSION-15, with a median follow-up of 18.7 months, was previously published in Nature Medicine in January 2025. The data presented at ESMO 2025 were analyzed using the same statistical methodology.
COMPASSION-15 2025 ESMO Data
In the intent-to-treat (ITT) population:
In the COMPASSION-15 study, patients with PD-L1 CPS <5 (low expression) and CPS <1 (negative expression) are 49.8% and 23%, respectively, of the ITT population. This represents a higher proportion of PD-L1 low and negative patient population in COMPASSION-15 compared to previous Phase III trials of other immune checkpoint inhibitors used in the treatment of first-line gastric cancer. Previous studies have shown limited responses to PD-1/L1 inhibitors in PD-L1 low-expression or negative patients.
Cadonilimab was approved by the NMPA in September 2024 for the first-line treatment for advanced gastric cancer, offering a new and effective immunotherapy option. Cadonilimab has been included in the 2025 CSCO Gastric Cancer Guidelines as the only Category I recommendation (Level 1A evidence) for first-line immunotherapy, regardless of PD-L1 expression, and is currently widely used in clinical practice.
Forward-Looking Statement of Akeso, Inc.
This announcement by Akeso, Inc. (9926.HK, “Akeso”) contains “forward-looking statements”. These statements reflect the current beliefs and expectations of Akeso’s management and are subject to significant risks and uncertainties. These statements are not intended to form the basis of any investment decision or any decision to purchase securities of Akeso. There can be no assurance that the drug candidate(s) indicated in this announcement or Akeso’s other pipeline candidates will obtain the required regulatory approvals or achieve commercial success. If underlying assumptions prove inaccurate or risks or uncertainties materialize, actual results may differ materially from those set forth in the forward-looking statements.
Risks and uncertainties include but are not limited to, general industry conditions and competition; general economic factors, including interest rate and currency exchange rate fluctuations; the impact of pharmaceutical industry regulation and health care legislation in P.R.China, the United States and internationally; global trends toward health care cost containment; technological advances, new products and patents attained by competitors; challenges inherent in new product development, including obtaining regulatory approval; Akeso’s ability to accurately predict future market conditions; manufacturing difficulties or delays; financial instability of international economies and sovereign risk; dependence on the effectiveness of the Akeso’s patents and other protections for innovative products; and the exposure to litigation, including patent litigation, and/or regulatory actions.
Akeso does not undertake any obligation to publicly revise these forward-looking statements to reflect events or circumstances after the date hereof, except as required by law.
About Akeso
Akeso (HKEX: 9926.HK) is a leading biopharmaceutical company committed to the research, development, manufacturing and commercialization of the world’s first or best-in-class innovative biological medicines. Founded in 2012, the company has created a unique integrated R&D innovation system with the comprehensive end-to-end drug development platform (ACE Platform) and bi-specific antibody drug development technology (Tetrabody) as the core, a GMP-compliant manufacturing system and a commercialization system with an advanced operation mode, and has gradually developed into a globally competitive biopharmaceutical company focused on innovative solutions. With fully integrated multi-functional platform, Akeso is internally working on a robust pipeline of over 50 innovative assets in the fields of cancer, autoimmune disease, inflammation, metabolic disease and other major diseases. Among them, 24 candidates have entered clinical trials (including 15 bispecific/multispecific antibodies and bispecific ADCs. Additionally, 7 new drugs are commercially available. Through efficient and breakthrough R&D innovation, Akeso always integrates superior global resources, develops the first-in-class and best-in-class new drugs, provides affordable therapeutic antibodies for patients worldwide, and continuously creates more commercial and social values to become a global leading biopharmaceutical enterprise.
For more information, please visit https://www.akesobio.com/en/about-us/corporate-profile/ and follow us on Linkedin.
SOURCE Akeso, Inc.


After a final warm-up, the factory team turned its attentions to the Superpole race. Having qualified eighth, Vierge was straight up into fifth with his CBR1000RR-R. Passing Lowes for fourth on lap two, the home rider was lapping faster than…