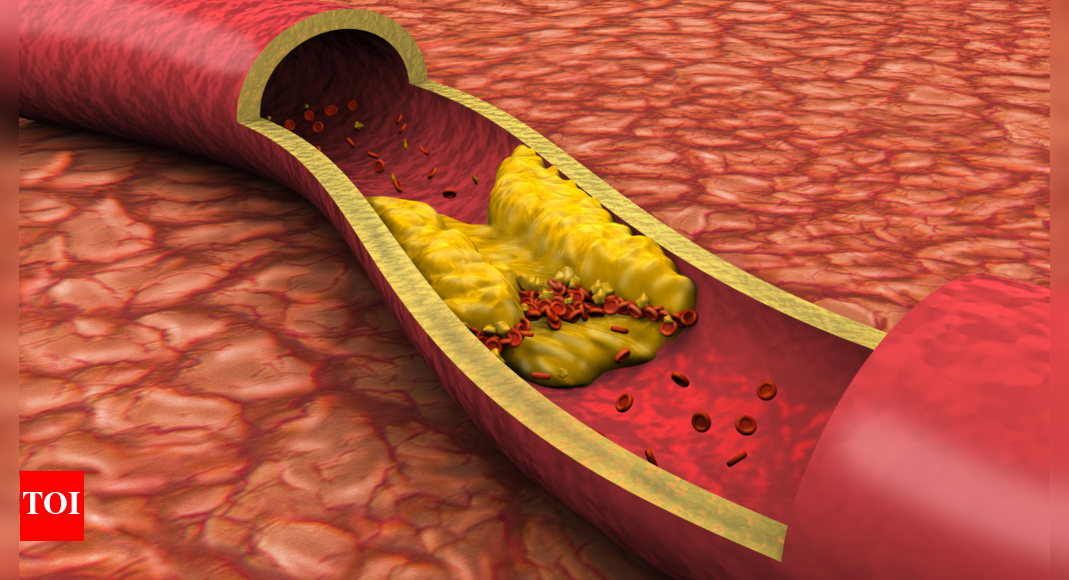
For heart health, one needs to be concerned with what we are eating as well as drinking. The arteries, that carry oxygen, promote blood circulation, can accumulate plaque over time, known as atherosclerosis. The accumulation of this…
Blog
-

LG Electronics Guides for Smaller-Than-Expected Earnings Setback — Update
By Kwanwoo Jun
LG Electronics guided for quarterly operating profit to fall 8.4%--a smaller decline than market consensus, thanks to its key affiliates' solid performance despite tough business conditions.
While challenges remain from higher U.S. tariffs and a delayed recovery in global demand, its home-appliance segment maintained its competitiveness and continued to be the market leader, while its vehicle-component segment achieved record profitability, the South Korean company said Monday.
The consumer-electronics giant said in a preliminary earnings report that its operating profit could come in at 688.90 billion won, equivalent to $481.9 million, for the July-September period, compared with 751.90 billion won a year earlier. The projection was above a FactSet-compiled consensus estimate of 618.79 billion won.
Revenue is expected to have fallen 1.4% to 21.875 trillion won, LG Electronics said, also beating analysts' estimate.
Shares of the company rose 2% after the better-than-expected guidance, trimming its year-to-date losses to below 4%.
The earnings projection came as LG Electronics recently raised $1.3 billion by selling a 15% stake in its Indian unit, LG Electronics India, in an initial public offering. The company said it expects the proceeds to provide significant funding to accelerate business structure improvements and future growth initiatives. The Indian unit will begin trading Tuesday.
LG Electronics said it would continue its push to grow new businesses, including its heating, ventilation and air-conditioning services as well as non-hardware platforms such as appliance subscriptions and online services.
Analysts at Daiwa Capital said in a recent note that LG Electronics is facing business uncertainties in the second half of the year, citing a larger-than-expected U.S. tariff impact and increasing competition in the television business. The Korean company on Monday said its media and entertainment segment, which includes its TV business, experienced higher marketing costs amid intensifying global competition.
The company is scheduled to release its full quarterly results later this month.
Separately, LG Energy Solution, an electric-vehicle battery maker affiliated with the parent LG Group conglomerate, earlier forecast a 34% increase in third-quarter operating profit, surpassing market expectations.
The battery unit's projection of 601.30 billion won, which includes an estimated 365.50 billion won U.S. tax credit, beat a FactSet-compiled consensus forecast of 518.29 billion won.
Write to Kwanwoo Jun at kwanwoo.jun@wsj.com
(END) Dow Jones Newswires
October 13, 2025 01:20 ET (05:20 GMT)
Copyright (c) 2025 Dow Jones & Company, Inc.
Continue Reading
-

Dermatological symptoms could signal higher risk in psychiatric patients
Scientists have discovered that mental health patients who have skin conditions may be more at risk of worse outcomes, including suicidality and depression. This work, which may aid in identifying at-risk patients and personalising…
Continue Reading
-
ASX00073 UNO SPE Shield shipped by Mouser
Compatible with the Arduino UNO form factor, it also supports SPI, UART, and I2C for interoperability with various devices.
Mouser writes:
“By incorporating RS485 connectivity, the ASX00073 UNO SPE…
Continue Reading
-

Detroit Lions HC Dan Campbell disappointed in SNF loss to Kansas City Chiefs
The Lions were riding pretty high heading into Sunday’s game with four straight wins and four straight contests in which their offense scored at least 34 points.
“Maybe we needed this,” Campbell said. “Maybe we needed to get kicked…
Continue Reading
-
Brain serotonin levels linked to sexual side effects from antidepressants
Researchers have discovered that the ability to have an erection or to orgasm is related to the levels of serotonin in the brain, but this relation only applies to depressed patients taking SSRI antidepressants. At the moment, there…
Continue Reading
-

2025 FIA GT World Cup gathers GT racing’s elite for Macau’s street racing showdown
2025 FIA GT World Cup gathers GT racing’s elite for Macau’s street racing showdown
The FIA GT World Cup returns to the streets of Macau from 13–16 November, 2025, with a 16-car grid…
Continue Reading
-

Solid Iron – How 60-Years of Japanese Investment in Western Australian Iron Ore Frames Future Investment Opportunities
A historical retrospective on Japan’s partnership in Western Australian iron ore projects, contextualising future investment opportunities between partners in emerging markets, technologies and industries.
To the unaware, you would not think there is much connecting Tokyo to a remote corner of the Australian continent 6,900 kilometres away. However, the ochre sands and red-black outcrops of Western Australia’s Pilbara region and the neon lights and steel skyscrapers of Tokyo are directly linked. While the contrast could not be greater, the locations are intrinsically paired – through iron ore. Pilbara iron ore is blasted, mined, crushed and screened at sites such as Mount Whaleback or Rhodes Ridge, transported by cargo train to ports on Western Australia’s coast, including Headland or Dampier, and shipped across the Indian and Pacific oceans to steel mills in Japan where it is blast-furnaced into steel to construct skyscrapers dotted across the Tokyo skyline and the infrastructure that connects it.
Today, Western Australian iron ore product comprises in excess of 50% of Japanese annual iron imports.EN1 But that does not reflect the whole story. The simple sale of iron ore from Western Australia’s natural resource-rich shores to the industry-rich, resource-poor islands of Japan has a long history and deep partnership underpinning it. From importing some of Australia’s earliest seaborn commodities, to navigating a twenty-year total embargo on iron ore export, and eventually underwriting and unlocking Western Australia’s largest iron ore projects, Japan is a constant partner in our iron ore. Japanese investment was, and remains, critical to Western Australia’s iron ore industry, silently founding the export market that continues to fuel the domestic economy today.
Read full insight to learn more.
Continue Reading
-

Evaluating the Role of Disease Duration in Systemic Therapy Response a
Introduction
Psoriasis is a chronic, immune-mediated inflammatory skin disease, with a global prevalence of approximately 2% to 3%. It is often associated with significant physical, psychological, and social burdens.1 It typically follows a course of remission and recurrence; many patients only experience mild rash flares, but some may have a longer disease duration before receiving more intensive treatment.2 The present treatment approach uses a step-up regimen—starting with topical drugs, progressing to phototherapy, and reserving systemic drugs for patients with poor control under conventional treatment.3,4 This method minimizes overtreatment of mild disease but often delays effective systemic intervention until the disease has persisted for a longer duration. This raises the question whether early systemic treatment could yield better outcomes?
In recent years, systemic therapy, including traditional drugs such as methotrexate and acitretin, as well as biologics targeting specific inflammatory pathways, have significantly improved patients’ symptoms.5–9 However, the response to systemic therapy varies greatly among individuals, influenced by multiple factors including disease severity, comorbidities, age of onset, treatment history, and family history.10–12 In other chronic immune-mediated inflammatory diseases, like Crohn’s disease and rheumatoid arthritis, researchers have reported the role of disease duration on treatment response, with early use of systemic treatments leading to better clinical outcomes.13,14 Similar to psoriasis, earlier systemic therapy may have greater advantages. However, there is still a lack of study data on the impact of disease duration on systemic therapy outcomes in psoriasis.
To our knowledge, large-scale, real-world studies specifically designed to investigate the influence of psoriasis disease duration on treatment outcomes are lacking. Previous studies have not addressed whether the duration of psoriasis affects treatment efficacy in clinical practice. Additionally, it is unclear whether the chronicity of the disease alters the efficacy of specific systemic therapies. This lack of evidence limits the development of personalized treatment strategies, particularly for patients with long-term disease.
To address this issue, this multicenter prospective observational study utilized data from the SPEECH registry to explore whether early systemic therapy truly improves clinical or patients reported outcomes. Patients with moderate-to-severe psoriasis were stratified into three groups based on disease duration at enrollment: short duration (<2 years), medium duration (2–10 years), and long duration (>10 years). Participants received various systemic therapies, including biologics, methotrexate, and acitretin. Although treatment switching may occur in clinical practice, our analyses focused on patients who maintained a single systemic therapy for at least six months, thereby ensuring reliable evaluation of treatment response. Furthermore, we examined potential contributors to disease progression, including treatment type, patient demographics, and clinical characteristics, to explore whether specific therapies were associated with greater disease stability or risk of deterioration. This study provides novel insights into the relationship between psoriasis disease course and systemic therapy efficacy in real clinical settings.
Material and Methods
Study Design
The SPEECH registry is a multicenter prospective observational study that records the clinical features of psoriasis in the Chinese population and the safety and efficacy of different treatment methods such as biologics, conventional systemic therapy, and phototherapy.15 The SPEECH registry is registered at seven dermatology centers in Shanghai, China. All data were prospectively collected at each visit using standardized case report forms and entered into a central electronic database by trained dermatology staff to ensure data completeness and accuracy. This study received ethical approval from the Institutional Review Board of Shanghai Dermatology Hospital (#2020-36), along with approvals from the ethics committees of all other participating centers.
Participants
All participants in this study are selected from the SPEECH cohort and met the following inclusion criteria: 1. Adults diagnosed with moderate-to-severe plaque psoriasis who were treated with biologic agents (such as guselkumab, ustekinumab, ixekizumab, secukinumab, or adalimumab), methotrexate, or acitretin; 2. Treatment was administered according to established protocols without modifications in dosage or treatment intervals. To ensure reliable evaluation of treatment response, only patients who remained on a single systemic therapy for at least six months were included in the analysis. Key exclusion criteria are the absence of baseline information on disease duration (Figure 1).
Figure 1 Study flowchart.
Data Collection and Outcome Measures
Demographic and clinical data were drawn from all participants at baseline, including age, gender, education level, disease duration, family history of psoriasis, BMI, lifestyle (smoking, drinking), early-onset psoriasis (age of onset <40 years), comorbidities (obesity, psoriatic arthritis, hyperlipidemia, and hypertension). To ensure consistency, treatment adherence and clinical assessments were regularly recorded and reviewed at each visit by om-site investigators.
Additionally, disease characteristics were assessed using measures such as Psoriasis Area and Severity Index (PASI), Body Surface Area (BSA), Dermatology Life Quality Index (DLQI), Physician Global Assessment (PGA), Patient Global Assessment (PtGA), Hospital Anxiety and Depression Scale – Anxiety (HADS-A) and Depression (HADS-D). Treatment efficacy was assessed at 3 months (12 weeks) and 6 months (28 weeks) after treatment, using criteria such as the PASI 75 (≥75% improvement in PASI), BSA <1/3 (clear to almost clear), PGA 0/1 (clear to almost clear), DLQI 0/1 (little to no impact on life), PtGA 0/1 (clear to almost clear), and HADS-A or HADS-D = 0 (complete resolution of anxiety or depression symptoms) at 3 months and 6 months post-treatment.
Statistical Analyses
The primary analysis used a modified intention-to-treat (mITT) dataset and employed multiple imputation to fill in the missing treatment efficacy data. By grouping patients according to disease duration (<2 years, 2~10 years, and ≥10 years). Continuous variable hypothesis Follow a normal distribution, represented by the mean (SD), and statistical comparisons are conducted using the Student’s t-test. Non-normally distributed continuous variables are represented as median (interquartile range) and compared using the Mann–Whitney U-test. Categorical variables are expressed as n (%), and analyzed using the χ2 test or Fisher’s exact probability method. Using the group with a disease duration of <2 years as a reference, logistic regression analysis was employed to evaluate the treatment response of patients with different disease durations. The adjusted odds ratio (aOR) and its 95% confidence interval (CI) were computed. To visualize response trends, line charts were generated, and intergroup differences were assessed using the Kruskal–Wallis and Dwass–Steel–Critchlow–Fligner (DSCF) tests. Additionally, subgroup analyses were performed to investigate potential interactions and factors. Sensitivity analysis was conducted based on the per-protocol (PP) dataset to further validate the robustness of the study findings. All statistical models were adjusted for potential confounders, such as gender, age, education level, early-onset psoriasis, family history of psoriasis, psoriatic arthritis (PsA), obese (BMI>28), baseline PASI, BSA score, different categories of treatment drugs, the hospital to which the patient belonged, and prior systemic therapy history. Statistical analyses were performed with R software version 4.2.2, and results with p-value <0.05 were deemed statistically significant.
Results
Clinical Characteristics According to Disease Duration
Among the initially registered 2470 patients, 1947 fulfilled the inclusion criteria for this analysis. Due to incomplete baseline information, 39 patients were excluded, leaving 1908 patients eligible for the final analysis (Figure 1). Participants were divided into three groups based on the duration of the disease: <2 years, 2~10 years, and ≥10 years. In the comparison of baseline characteristics across the three patient groups, it was noted that patients in the short disease duration group (<2 years) had more females (29.1% vs 18.3% vs 25.0%), higher education levels, more obesity (24.1% vs 19.0% vs 16.8%). In addition, patients in the short disease duration group had lower baseline PASI and BSA scores. Moreover, patients in the long disease duration group (≥10 years) were more likely to receive biologic therapy and had early-onset psoriasis (p <0.05). There were no significant differences in the remaining covariates (Table 1).

Table 1 Demographic and Patient Characteristics of the Study Cohort
Comparison of Treatment Efficacy
Using univariate logistic regression analysis to compare the efficacy outcomes among the three disease duration groups. In the unadjusted analysis, at 3 months, there were no significant differences in the proportions of the three different disease duration groups achieving BSA <1/3, PGA 0/1, PASI 75, DLQI 0/1, PtGA 0/1, HADS-A = 0, and HADS-D = 0. Even after adjusting for relevant covariates, these results remained non-significant (Table 2). Moreover, the results of the above at 6 months were similar, except that the PASI75 response rate was lower in the long disease duration group, but the adjusted OR showed no significant difference (Table 3).

Table 2 Comparison of Clinical Efficacy and Psychological Outcome of Systemic Therapy in Different Disease Duration at 3 Months

Table 3 Compare of Clinical Efficacy and Psychological Outcome of Systemic Therapy in Different Disease Duration at 6 Months
The Kruskal–Wallis and DSCF tests were used to assess intergroup differences, and line graphs were used to illustrate the changes of various treatment outcomes over time in the three groups (Figure 2). The results showed that, except for the baseline, there were almost no significant differences in the outcomes at each time point among the three groups. Moreover, all three groups exhibited downtrend of the outcomes over time, reinforcing the consistency of treatment efficacy irrespective of disease duration. This underscored the stability of systemic therapy outcomes across different disease durations.

Figure 2 Line graphs comparing treatment outcomes over time among three groups. (A) Line graphs of PSAI score and time; (B) Line graphs of BSA score and time; (C) Line graphs of DLQI score and time; (D) Line graphs of PGA score and time; (E) PASI, Line graphs of PtGA score and time. **, p<0.01; ***, p<0.001.
Abbreviations: PASI, Psoriasis Area and Severity Index; BSA, Body Surface Area; DLQI, Dermatology Life Quality Index; PGA, Physician’s Global Assessment. PtGA, Patient Global Assessment.
When using PASI75 as the primary efficacy endpoint, subgroup analyses showed no significant interaction between baseline variables and disease duration categories (p for interaction >0.05; Figures S1 and S2). Similarly, no significant interaction was observed between treatment type or prior systemic therapy history and disease duration in terms of treatment outcomes, indicating that the efficacy of systemic therapy is not affected by disease duration. These results support the robustness and consistency of our primary analysis.
Sensitivity Analysis
Sensitivity analysis was also performed to verify the reliability of our results using the PP dataset. Disease duration was categorized into two groups based on the median: <15 years and ≥15 years. Both univariate and multivariate logistic regression analyses showed no significant difference in efficacy between the two groups (Tables S1 and S2). Furthermore, we conducted a hierarchical analysis according to treatment type (traditional agents vs biologics) and prior systemic therapy exposure. As presented in Tables S3 and S4, the results showed no significant differences in PASI75 response among different disease duration groups within eachstratum. The Mantel-Haenszel pooled estimates further demonstrated no significant heterogeneity across strata. The results showed that disease duration did not affect the efficacy of systemic therapies, regardless of treatment type or prior systemic therapy, supporting the robustness and consistency of our primary analysis.
Discussion
This large-scale, prospective, multicenter study provides valuable evidence on psoriasis management and treatment patterns, with patients receiving systemic therapy in routine clinical settings at seven hospitals in Shanghai, China. This study provides valuable insights into how disease duration affects clinical features and treatment outcomes of systemic therapy in Chinese psoriasis patients. Patients were divided into three groups based on disease duration: <2 years, 2–10 years, and ≥10 years. A key finding of our study is that our study showed no significant correlation between disease duration and treatment response in terms of clinical efficacy (PASI75, PGA 0/1, BSA <3) and patients reported outcomes (DLQI 0/1, PtGA 0/1, HADS-A=0, HADS-D=0) at both 3 months and 6 months. This conclusion remained robust after adjusting for relevant covariates, and sensitivity analysis further verified the reliability of the results.
We observed that patients with a short disease duration (<2 years) had higher education levels, more female patients, more obese patients, and lower baseline PASI and BSA scores. However, these characteristics did not affect the treatment outcomes. Notably, patients with a longer disease duration were more likely to receive biological therapy and present with early-onset psoriasis, both of which usually associated with increased disease severity or longer treatment exposure. This is consistent with the findings from the British Association of Dermatologists Biologic Interventions Register (BADBIR), where longer disease duration was observed with biologics compared to traditional systemic therapy (23 vs 19 years, p <0.001).16
Our findings were consistent with prior clinical studies indicating that disease duration cannot independently predict the response to systemic or biological therapy. Most available studies have focused on biologics, consistently showing that treatment response is unaffected by disease duration. For instance, a prospective cohort study of 118 patients receiving etanercept found no significant difference in PASI improvement at week 24 between between patients with disease durations <20 years versus ≥20 years (p = 0.170).17 Similarly, in another retrospective cohort study involving 135 patients receiving guselkumab, Hung et al reported no correlation between PASI 75 response and disease duration at week 36 (OR: 0.99, 95% CI 0.94–1.05), with comparable mean durations among responders and non-responders (18.42 vs 18.91 years).18 Post-hoc analysis of large RCTs, including the NAVIGATE and VOYAGE trials (n = 1678), indicated that the disease duration (<15 years vs ≥15 years) was not significantly associated with the PASI 90 response at week 40 (OR: 1.13, 95% CI: 0.88–1.47).19 Furthermore, a recent meta-analysis including 4,649 patients found that disease duration was not significantly associated with biologic treatment response (OR 0.99, 95% CI 0.98–1.00, p=0.17), reinforcing that systemic therapy efficacy is generally independent of disease duration.20
Evidence regarding traditional systemic therapies is comparatively limited, but appears to suggest a similar trend. In our subgroup analyses, disease duration did not significantly influence treatment outcomes with methotrexate or acitretin. Although real-world evidence from prior studies has demonstrated the effectiveness of traditional systemic therapies in patients with moderate-to-severe psoriasis, they did not specifically evaluate whether disease duration influences treatment response. The BADBIR cohort identified predictors of reduced treatment effectiveness, including prior systemic exposure, male sex, comorbidities, and alcohol consumption, but disease duration was not among them.21 Similarly, a systematic review of traditional systemic therapies found no evidence that disease duration significantly modified treatment response.22 Additional analysis of treatment-switch patterns reported that disease duration did not affect the transition between traditional drugs and biologics.23 Recent data further suggest that prior use of traditional drugs such as methotrexate or acitretin does not compromise the efficacy or drug survival of subsequent biologic therapy.24 Collectively, these findings indicate that disease duration is not a major determinant of treatment outcomes for either traditional systemic agents or biologics. Importantly, prior exposure to traditional therapy does not diminish the effectiveness of subsequent biologics, thereby supporting the rationale for a step-up therapeutic strategy in clinical practice.
Although our research results indicated that early systemic therapy does not improve treatment outcomes in actual clinical settings, some studies report that early systemic treatment can actively control systemic inflammation to prevent or delay damage related to comorbidities, including psoriatic arthritis (PsA) and cardiovascular diseases.25–29 Two different cohort studies indicated that compared to patients receiving phototherapy or topical medication, those undergoing systemic treatment have a significantly reduced risk of developing PsA.25,26 Furthermore, new evidence suggested that biological therapy is beneficial in reversing the potential pathogenic processes of cardiovascular diseases, such as endothelial dysfunction and the progression of atherosclerotic plaques. In a large retrospective study, Song WJ et al found that compared to phototherapy, biologic therapy and non-biologic systemic therapy reduce the risk of new-onset MACE in psoriasis patients.27 In order to determine whether early systemic intervention has a protective effect on psoriatic arthritis, or cardiovascular diseases, as well as whether these potential benefits make it worthwhile to upgrade treatment earlier, more long-term longitudinal studies are necessary in the future.
This study indicated that the early effectiveness of systemic therapy for psoriasis remains consistent, regardless of the disease duration, which may be related to the ability of biologics to modulate chronic inflammatory pathways and resident memory T cells in long-standing disease.30,31 This suggests that even patients with long-standing psoriasis or delayed treatment initiation can achieve meaningful clinical responses, supporting the use of systemic therapy irrespective of disease duration.
Our research underscore that initiating systemic therapy early does not lead to better outcomes, and this observation supports the widely accepted step-up treatment strategy in current clinical practice.32 Using systemic therapy for patients with poor response to topical treatment and phototherapy reduces unnecessary systemic drug exposure and its associated costs and risks.4 In the absence of aggressive disease characteristics or rapid progression of joint involvement, systemic therapy may not need to be initiated immediately based solely on the disease duration. Conversely, the severity of the disease, the burden of symptoms, and the impairment of quality of life still be the main factors influencing clinical judgements. These findings provided clinical practice evidence, highlighting the importance of gradually and individually escalating systemic therapy regimens in the management of psoriasis.
It is important to recognize the limitations inherent in our study. First, like many observational studies, our analysis may be susceptible to various biases, including selection bias and unmeasured confounding factors. Second, the study cohort only included Chinese patients, which limits the generalizability of the results. Third, although a follow-up period of 6 months offers notable findings on early responses to treatment, it does not provide information on the long-term efficacy of systemic therapy or the potential effects of disease duration on outcomes such as comorbidities. Therefore, extended longitudinal follow-up is necessary to evaluate these crucial aspects.
Conclusion
Our research findings demonstrates that the short-term efficacy of systemic therapy is consistent across different disease durations, supporting the “step-up” treatment strategy in psoriasis management. This multicenter evidence adds new insights by comparing traditional agents and biologics, showing that disease duration does not alter systemic therapy response. However, emerging evidence suggests that early systemic therapy may provide long-term benefits in preventing psoriatic arthritis and major cardiovascular events. Future long-term prospective studies are needed to determine whether early systemic interventions have a protective effect on comorbidities and to refine personalized treatment plans to balance the benefits for skin and quality of life with the prevention of systemic comorbidities.
Data Sharing Statement
The dataset supporting this research can be obtained from the corresponding author upon reasonable request.
Ethics Statement
This study was approved by the medical ethics committees of the following institutions: Shanghai Skin Disease Hospital (approval No. 2020-36), Shanghai Sixth People’s Hospital (approval No.2020-KY-047K), Shanghai Changzheng Hospital (approval No.2020-27), and Shanghai Tenth People’s Hospital (approval No.20KT110). All participants provided written informed consent for the publication of their clinical data. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Author Contributions
Min Dai, Yuxiong Jiang, Yujing Xi and Lezhen Xu are co-first authors. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was sponsored by grants from the National Key Research and Development Program of China (2023YFC2508106), National Natural Science Foundation of China (No. 82430101, 82273510), Innovation Program of Shanghai Municipal Education Commission (No. 2025GDZKZD06), Shanghai Dermatology Research Center (2023ZZ02017), Clinical Research Plan of SHDC (No. SHDC22022302).
Disclosure
The authors declare no conflicts of interest.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
2. Ma LF. Inflammatory memory in psoriasis: from remission to recurrence. J Allergy Clin Immunol. 2024;154(1):1.
3. Gisondi P, Del Giglio M, Girolomoni G. Treatment Approaches to Moderate to Severe Psoriasis. Int J Mol Sci. 2017;18(11):2427. doi:10.3390/ijms18112427
4. Chinese Society of Dermatology, China Dermatologist Association, Dermatology & Venereology Specialized Committee of Chinese Association of Integrative Medicine. Guidelines for the treatment of psoriasis with biologics and small-molecule drugs in China (2024). Chin J Dermatol. 2024;57(11):976–997.
5. Sugumaran D, Yong ACH, Stanslas J. Advances in psoriasis research: from pathogenesis to therapeutics. Life Sci. 2024;355:122991. doi:10.1016/j.lfs.2024.122991
6. Lebwohl M. Advances in biologic therapy of psoriasis. J Eur Acad Dermatol Venereol. 2023;37(9):1689–1690. doi:10.1111/jdv.19287
7. Lee HJ, Kim M. Challenges and Future Trends in the Treatment of Psoriasis. Int J Mol Sci. 2023;24(17):13313. doi:10.3390/ijms241713313
8. Alabas OA, Mason KJ, Yiu ZZN, et al. Effectiveness and survival of methotrexate versus Adalimumab in patients with moderate-to-severe psoriasis: a cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Br J Dermatol. 2023;189(3):271–278. doi:10.1093/bjd/ljad179
9. Armstrong AW, Pathophysiology RC. Clinical Presentation, and Treatment of Psoriasis: a Review. JAMA. 2020;323(19):1945–1960. doi:10.1001/jama.2020.4006
10. Huang D, Zhong X, Jiang Y, et al. Insulin resistance impairs biologic agent response in moderate-to-severe plaque psoriasis: insights from a prospective cohort study in China. Br J Dermatol. 2024;191(4):616–623. doi:10.1093/bjd/ljae147
11. Jiang Y, Liu X, Ma R, et al. The Impact of Family History on Clinical Presentation and Biologic Treatment Response in Patients with Psoriasis: a Multicenter Prospective Cohort Study. Am J Clin Dermatol. 2025;26(2):291–300. doi:10.1007/s40257-025-00918-y
12. Jiang Y, Chen Y, Yu Q, Shi Y. Biologic and Small-Molecule Therapies for Moderate-to-Severe Psoriasis: focus on Psoriasis Comorbidities. BioDrugs. 2023;37(1):35–55. doi:10.1007/s40259-022-00569-z
13. Deane KD, Holers VM. Rheumatoid Arthritis Pathogenesis, Prediction, and Prevention: an Emerging Paradigm Shift. Arthritis Rheumatol. 2021;73(2):181–193. doi:10.1002/art.41417
14. Berg DR, Colombel JF, Ungaro R. The Role of Early Biologic Therapy in Inflammatory Bowel Disease. Inflamm Bowel Dis. 2019;25(12):1896–1905. doi:10.1093/ibd/izz059
15. Yu N, Peng C, Zhou J, et al. Measurement properties of the patient global assessment numerical rating scale in moderate-to-severe psoriasis. Br J Dermatol. 2023;189(4):437–446. doi:10.1093/bjd/ljad188
16. Iskandar IYK, Ashcroft DM, Warren RB, et al. Demographics and disease characteristics of patients with psoriasis enrolled in the British Association of Dermatologists Biologic Interventions Register. Br J Dermatol. 2015;173(2):510–518. doi:10.1111/bjd.13908
17. Antoniou C, Dessinioti C, Stratigos A, Avgerinou G, Stavropoulos P, Katsambas A. Etanercept in severe, recalcitrant psoriasis: clinical response, safety profile and predictors of response based on a single institution’s experience. J Eur Acad Dermatol Venereol. 2009;23(8):979–982. doi:10.1111/j.1468-3083.2009.03093.x
18. Hung YT, Lin YJ, Chiu HY, Huang YH. Impact of previous biologic use and body weight on the effectiveness of guselkumab in moderate-to-severe plaque psoriasis: a real-world practice. Ther Adv Chronic Dis. 2021;12:20406223211046685. doi:10.1177/20406223211046685
19. Diels J, Thilakarathne P, Cameron C, McElligott S, Schubert A, Puig L. Adjusted treatment COMPArisons between guSelkumab and uStekinumab for treatment of moderate-to-severe plaque psoriasis: the COMPASS analysis. Br J Dermatol. 2020;183(2):276–284. doi:10.1111/bjd.18634
20. Hjort G, Schwarz CW, Skov L, et al. Clinical characteristics associated with response to biologics in the treatment of psoriasis: a meta-analysis. JAMA Dermatol. 2024;160(8):830–837. doi:10.1001/jamadermatol.2024.1677
21. Warren RB, Smith CH, Yiu ZZN, et al. Effectiveness and persistence of Acitretin, ciclosporin, fumaric acid esters and methotrexate for patients with moderate-to-severe psoriasis: a cohort study from BADBIR. Br J Dermatol. 2015;172(2):337–346. doi:10.1111/bjd.13225
22. Iskandar IYK, Ashcroft DM, Warren RB, et al. Persistence and effectiveness of nonbiologic systemic therapies for moderate-to-severe psoriasis in adults: a systematic review. Br J Dermatol. 2016;174(3):606–617.
23. Tabolli S, Giannantoni P, Paradisi A, Abeni D. The ‘switcher’ patient profile in psoriasis treatment: from traditional to biological and from biological to traditional systemic drugs. Br J Dermatol. 2015;173(1):256–258. doi:10.1111/bjd.13560
24. Piaserico S, Cazzaniga S, Gisondi P, et al. “Full-naïve” patients: the impact of previous methotrexate, cyclosporine, and Acitretin on first-line biologics response in the treatment of moderate-to-severe psoriasis—a monocentric retrospective study. J Eur Acad Dermatol Venereol. 2021;35(5):e327–e330.
25. Gisondi P, Bellinato F, Targher G, Idolazzi L, Girolomoni G. Biological disease-modifying antirheumatic drugs may mitigate the risk of psoriatic arthritis in patients with chronic plaque psoriasis. Ann Rheum Dis. 2022;81(1):68–73. doi:10.1136/annrheumdis-2021-219961
26. Felquer MLA, LoGiudice L, Galimberti ML, Rosa J, Mazzuoccolo L, Soriano ER. Treating the skin with biologics in patients with psoriasis decreases the incidence of psoriatic arthritis. Ann Rheumatic Dis. 2022;81(1):74–79. doi:10.1136/annrheumdis-2021-220865
27. Rosenthal YS, Schwartz N, Sagy I, Pavlovsky L. Incidence of Psoriatic Arthritis Among Patients Receiving Biologic Treatments for Psoriasis: a Nested Case–Control Study. Arthritis Rheumatol. 2022;74(2):237–243. doi:10.1002/art.41946
28. Song WJ, Oh S, Yoon HS. Association between biologic and nonbiologic systemic therapy for psoriasis and psoriatic arthritis and the risk of new-onset and recurrent major adverse cardiovascular events: a retrospective cohort study. J Am Acad Dermatol. 2025;93(1):
S0190–9622(25)00524–9 . doi:10.1016/j.jaad.2025.03.05529. Reich K, Griffiths CEM, Gordon KB, et al. Maintenance of clinical response and consistent safety profile with up to 3 years of continuous treatment with guselkumab: results from the VOYAGE 1 and VOYAGE 2 trials. J Am Acad Dermatol. 2020;82(4):936–945. doi:10.1016/j.jaad.2019.11.040
30. Iversen L, Conrad C, Eidsmo L, et al. Secukinumab demonstrates superiority over narrow-band ultraviolet B phototherapy in new-onset moderate to severe plaque psoriasis patients: week 52 results from the STEPIn study. J Eur Acad Dermatol Venereol. 2023;37(5):1004–1016. doi:10.1111/jdv.18846
31. Schäkel K, Reich K, Asadullah K, et al. Early disease intervention with guselkumab in psoriasis leads to a higher rate of stable complete skin clearance (‘clinical super response’): week 28 results from the ongoing phase IIIb randomized, double-blind, parallel-group, GUIDE study. J Eur Acad Dermatol Venereol. 2023;37(10):2016–2027. doi:10.1111/jdv.19236
32. Committee on Psoriasis. Chinese Society of Dermatology. Guideline for the diagnosis and treatment of psoriasis in China (2023 edition). Chin Jl of Dermatology. 2023;56(7):573–625.
Continue Reading
