
Apple’s foldable iPhone, long rumored and eagerly awaited, could now arrive in 2027 pushing back expectations by a year. While whispers of delays have been around for some time, the latest reports point to hinge and design challenges as the…
Blog
-
Variations in initiation of first antenatal care among women of reproductive age in sub-Saharan Africa: an event history analysis approach | Reproductive Health
Data
The data for this study were sourced from the most recent Demographic and Health Survey (DHS) conducted in thirty-six (36) sub-Saharan African countries. The DHS is a nationally representative sample survey that collects data on demographic and health indicators, including measures of reproductive health such as ANC attendance among women of reproductive age (15–49 years). The data for the current study were drawn from DHS surveys conducted between 2007 and 2019 in the thirty-six countries involved in the study. The data were downloaded from the MEASURE DHS website at http://dhsprogram.com/data/available-datasets.cfm on February 1st, 2021. The list of countries by sub-region and the respective survey years and corresponding sample sizes are presented in Appendix 1 as part of the supplementary results.
Study sample and management of missing cases
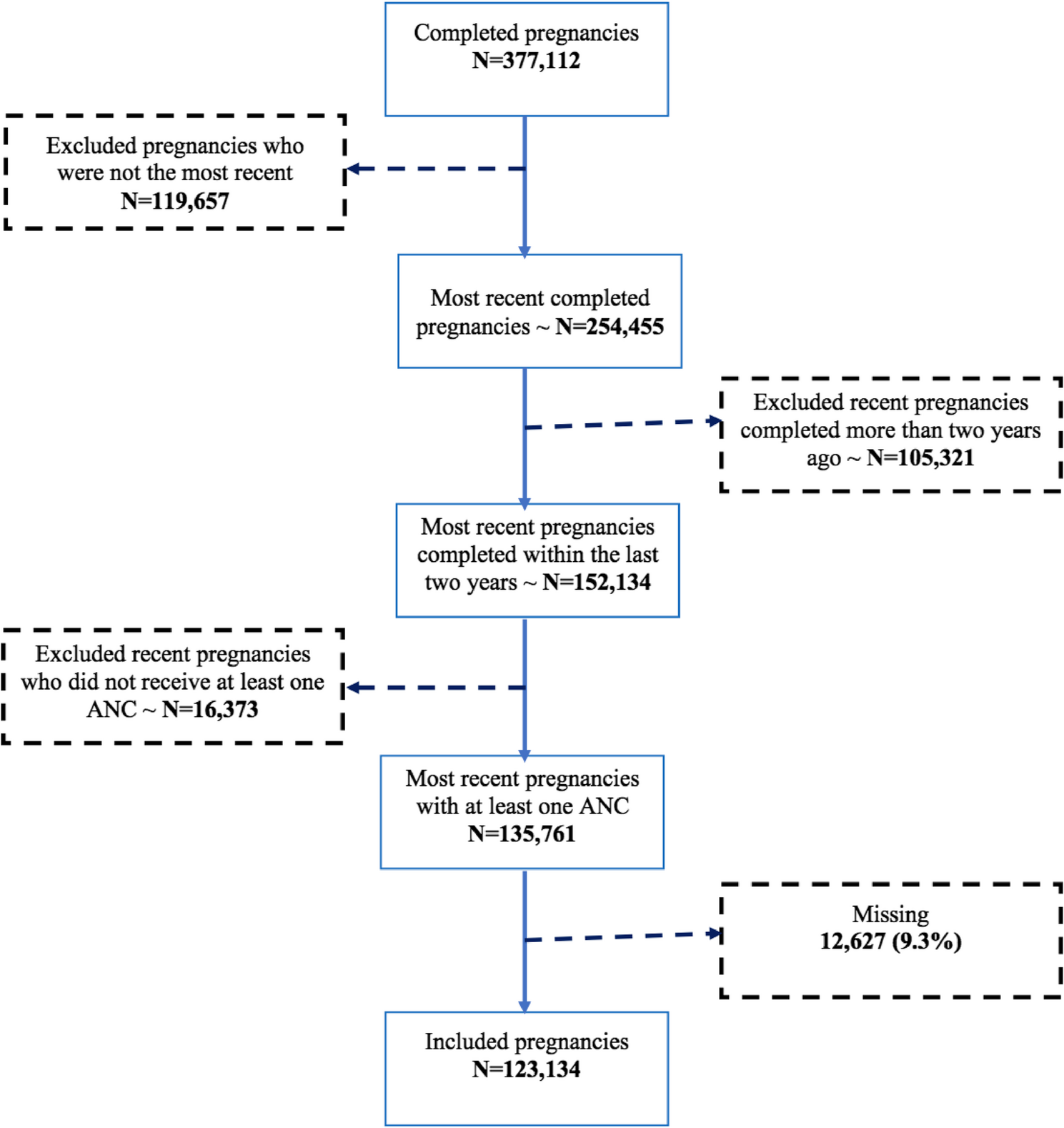
The sample for this study was based on the last pregnancies completed by women aged 15–49 years within the 2 years preceding the DHS survey and who made at least one ANC visit during this index pregnancy. After pooling the data for the most recent surveys in the thirty-six countries, 377,112 pregnancies were identified within the preceding five years of the survey. Among them, 119,657 pregnancies that were not the most recent were excluded. Approximately 105,321 such pregnancies were completed more than two years before the survey and were excluded from the analysis as shown in Fig. 1.
Fig. 1 Flow diagram showing the inclusion and exclusion criteria for selecting the study sample
A total of 152,134 pregnancies were completed within the last two years, among which 16,373 pregnancies that did not receive any ANC were excluded. The percentage of missing data on related variables for the current study is low (less than 6% on single variable and less than 10% for the whole data set). The analyses were thus limited to cases with complete data employing listwise or case wise deletions. Excluding missing cases from the final sample does not pose a challenge for the analysis because it is generally accepted that if the presence of missing data on related variables are unrelated to any other variable, then the data are missing completely at random, and data missing completely at random with a small amount of missing data (less than 10% as in the case of the current study) still provide reliable and valid results as analysis of all cases with complete data [18, 19]. Thus, the final analysis was based on 123,134 completed pregnancies with valid data on all the variables included in the analysis. A table showing the percentage of missing cases per variable has been presented in the supplementary materials (see Appendix 2 in the supplementary materials).
Variables
Dependent variable
The outcome variable for this study was a time variable measured for each pregnancy (pregnant woman) subject to the risk of ANC initiation. The dependent variable equals the duration before the event of the first ANC attendance. The duration of the dependent variable was measured in months and ranged from 1 to 9 months.
Independent variables
The predictor variables for this study included factors associated with ANC according to the literature and available in the data sets. Previous studies have identified the factors associated with the utilization of ANC services in LMICs to include household wealth quintiles [12, 13, 17, 20,21,22,23,24,25], place of residence [9, 12, 24,25,26], female education [9, 12, 13, 22,23,24,25], desire for pregnancy [8, 12, 13, 23, 25], female occupation [9, 23], age [12, 24,25,26,27], pregnancy rank/parity [9, 23, 25, 26], mass media exposure [12, 23, 25], number of children under five [8, 9], sociocultural norms and practices [20, 25], women’s autonomy [9, 25], marital status [25], and husbands’ education [9]. Additionally, some studies provide evidence that the odds of ANC coverage are lower among women from households belonging to the poor wealth quintile, women who have no formal education or who are less educated [17, 20, 21, 25] and women living in rural areas [12, 20, 25, 26]. There is also empirical evidence showing the link between family/community involvement and utilization of ANC services [5], while others have noted the role of sociocultural factors [21, 25]. For example, in Ghana, women in predominantly Muslim areas appear to be more limited in their ability to participate in reproductive health decision-making [21]. Additionally, other factors, such as exposure to mass media, especially locally driven mass media, have been shown to strongly impact health service utilization [28]. Furthermore, there has been extensive research on barriers to ANC utilization in SSA. A systematic review of outcome measures and determinants of unmet reproductive health needs revealed that economic constraints, long-distance travel to access services and low education are among the key predictors of ANC utilization among women in some West African countries [22]. Again, the results of a systematic review and meta-analysis in Ethiopia showed that improving female education and women’s empowerment could reduce the magnitude of delayed ANC uptake [9]. The results of other studies also indicate that women with wanted pregnancies are more likely to receive antenatal care [8, 13, 23]. The results regarding place of residence show that while some studies [9, 20, 26] have found a strong relationship between ANC uptake and place of residence, others [13] have reported weak or no significant associations. Additionally, while some studies have shown a negative relationship between female age and ANC uptake [26], another study [13] has shown no such association.
The present study investigates variations in the first initiation of ANC over time during pregnancy and examines the influence of associated risk factors at the global SSA, controlling for covariates identified from previous research. Drawing on an adaptation of the Andersen behavioral model (1995), the various factors controlled for in this study were grouped into four categories consisting of environmental factors, predisposing characteristics, enabling factors and need factors, as shown in Fig. 2. The environmental/external factors included place of residence (urban or rural), country (all 36 countries included in the study) and sub-region (eastern, middle, southern or western Africa). Predisposing characteristics include respondent’s age at the birth of the child (in five-year age groups), highest level of education, type of occupation, marital status, mass media exposure (ranking variable from “very low” to “very high”)Footnote 1, and partner’s level of education. The enabling factors considered were household wealth quintile and women’s participation in the household’s decision-making processFootnote 2 (coded as involved in 0 – no decision; 1–1 decision; 2–2 decisions; 3–3 decisions; 4–4 decisions). Need factors included desire for pregnancy (wanted then, wanted later, wanted no more), number of births and ever had a pregnancy terminated. The list of independent variables and their categorization are shown in Table 1.
Table 1 Percentage distribution of study population by selected characteristics Fig. 2 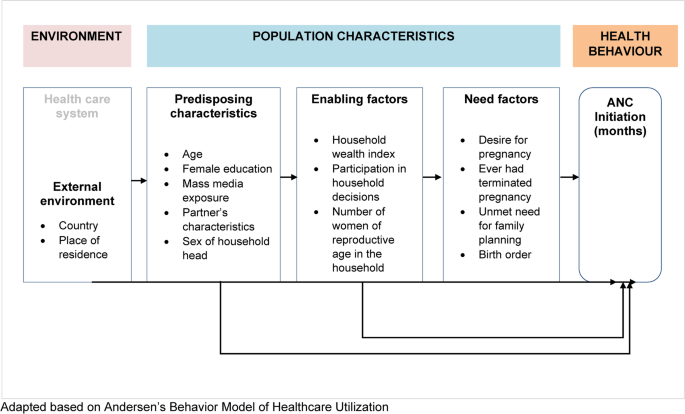
Conceptual Model Showing Factors Associated with initiation of antenatal care visits among women of reproductive age in sub-Saharan Africa
To ensure the reliability and accuracy of the regression models, a comprehensive multicollinearity test was conducted to assess correlation between all independent variables. Variables found to be highly correlated were systematically excluded. These variables were language, sub-region, and year of interview which were highly correlated with country of residence. However, due to the importance of these variables in the understanding of the context and to assess the variations in the chances of ANC initiation across the various sub-Saharan African regions, an alternative model excluding country was implemented. The alternate model accommodated the categorization of countries by sub-region and controlled for survey year. The results of the alternate model are included as supplementary results (see Appendix 4). These adjustments were made to enhance the clarity and interpretability of the models while addressing multicollinearity concerns.
Analytical strategy
The characteristics of the study sample were described using percentage distributions. All the independent variables, including survey year, were coded as categorical variables. The association between the timing of the first ANC visit and each independent variable was assessed using cross-tabulation with the Pearson chi-square test. Kaplan-Meier survivor curves were generated to examine the extent to which ANC initiation occurred over time according to the selected covariates. The Kaplan-Meier curves were generated to explore temporal trends in ANC initiation and to construct survival curves for participants stratified according to the selected covariates. The log-rank test was used to determine the significance of differences in survival distributions. At the multivariate level, a number of modeling techniques were explored, and model diagnostics and fitness tests were used to determine the best fit model for the data. The first modeling approach that was explored was multilevel modeling considering the nesting of respondents in countries, clusters and households. The intraclass coefficient (ICC) from the null model showed that only 0.6% (ICC = 0.0063) of the variation in ANC initiation was explained by between-cluster differences, indicating that a conventional one-level regression model fits the data better than a multilevel model [29]. After ruling out multilevel modeling, event history analysis was explored given the nature of the dependent variable. Discrete–time logit models were specified to examine the unadjusted and adjusted effects of each covariate on the dependent variable. The discrete-time survival analysis employed does not require an assumption of proportional hazards as piecewise exponentials [30]. In conducting the statistical analysis, the data were weighted to make the findings generalizable to women of reproductive age (15–49 years) within each country, and differences were tested for significance at the 5% level. All the statistical analyses were performed in R [31]. The analyses employed many R packages including survival [32], dplyr [33], knitr [34], haven [35], survey [36], gtools [37], numDervi [38], car [39], vim [40], summarytools [41], discsurv [42], survminer [43], flextable [44], officer [45], jtools [46], and finalfit [47].
Continue Reading
-

Brevundimonas vesicularis sepsis in a 2-month-old infant in rural Gambia: a case report | Journal of Medical Case Reports
Brevundimonas vesicularis is a non-lactose fermenter, Gram-negative bacillus, and is usually isolated from clinical and environmental samples. It is an opportunistic pathogen that affects children and adults. Most cases may be due to underlying…
Continue Reading
-
New moon likely to be sighted on October 21 :SUPARCO
– Advertisement –
ISLAMABAD, Oct 21 (APP):The Space and Upper Atmosphere Research Commission (SUPARCO) has announced that the new moon of Jamadi ul awwal, 1447 AH, is expected to be born on October 21 at 17:25 PST.
At the time of sunset on…
Continue Reading
-
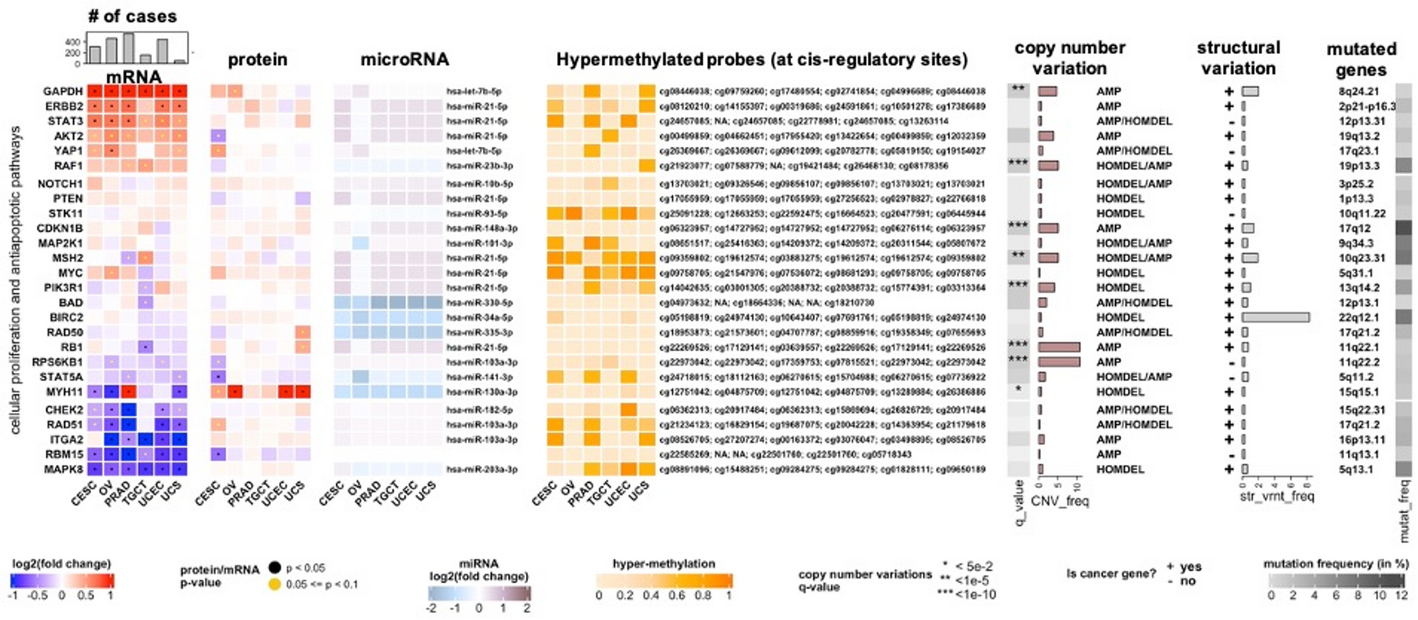
MultiModalGraphics: an R package for graphical integration of multi-omics datasets | BMC Bioinformatics
MultiModalGraphics is an R/Bioconductor package that leverages object-oriented S4 classes to visualize multimodal biological data with embedded statistical annotations. Originally developed for collaborative multi-omics studies [23,24,25], the…
Continue Reading
-
Sean ‘Diddy’ Combs files to appeal his conviction and sentence | Ents & Arts News
Sean ‘Diddy’ Combs is appealing the conviction handed down to him earlier this year over prostitution charges relating to his former girlfriends and male sex workers.
The music mogul was given a 50-month sentence and a $500,000 fine…
Continue Reading
-
Differences in swallowing efficacy of disease modifying treatment between infants receiving pre-symptomatic and symptomatic administration | Orphanet Journal of Rare Diseases
Sample demographics and characteristics
Sixty-nine infants (49% female) meeting eligibility criteria were identified and included in the investigation. The majority received treatment after symptom onset (N = 52, 75%) and had two copies of SMN2 (pre-symptomatic N = 17, 100%; symptomatic N = 48, 92%) with others having three copies. All infants were treated with available disease modifying therapies (Risdiplam [Evrysdi®], Nusinersen [Spinraza®],Onasemnogene-abeparvovec [Zolgensma®]), with nearly half having received a combination of treatments (pre-symptomatic N = 10, 59%; symptomatic N = 28, 54%). Interestingly, ten (19%) of the infants who received treatment after symptom onset were identified as having SMA following SMA screening without symptoms triggering a referral and diagnosis. Upon initial neurology evaluation eight of those infants (80%) already exhibited clear symptoms of SMA (ex. Loss of reflexes) which were identified at an average age of 16 days. The other two did not exhibit symptoms at the time of their initial neurology consultation, though developed symptoms before their treatment was administered an average of 7 days later.
Infants treated pre-symptomatically received treatment at a younger age (median = 0.50, IQR 0.44 months), than those treated after symptom onset (2.81, IQR 3.56 months, t = 17.67, p < 0.001, δ = 0.89). Nine infants (13%) were born prematurely, with all but one being born in the late preterm period (median 36 weeks). Other comorbidities included laryngo or tracheomalacia (N = 3, 4%), biliary atresia (N = 1, 1%), craniosynostosis (N = 1, 1%), extralobar sequestration (N = 1, 1%), paraesophageal hernia (N = 1, 1%), and milk protein allergy (N = 1, 1%).
Median age of infants at the time of their last VFSS was 7.92 months (IQR 4.83), with infants who received pre-symptomatic treatment younger at the time of their last exam (6.8 IQR 5.77 months) than those who received treatment after symptoms (8.35, IQR 4.71; t = 2.96, p = 0.04, δ = 0.33). Although the majority (80%, N = 55) of infants underwent swallow studies due to clinical symptoms, 20% (N = 14) underwent the exam without symptoms as part of a routine, high-risk workup. Significantly more infants who received pre-symptomatic treatment underwent a routine, high-risk VFSS (59%, N = 10) than did those who received symptomatic treatment (8%, N = 4, p < 0.001, OR 0.06). Nearly all infants (86%, N = 59) were evaluated while consuming thin liquids, with other consistencies observed including mildly thick (43%, N = 30), moderately thick (22%, N = 15).
At the time of last VFSS, 50% (N = 26) of symptomatic treated infants were receiving noninvasive ventilation or mechanical ventilation via tracheostomy (22/26, 85% strictly nocturnal), while only one of those treated pre-symptomatic required these supports (strictly nocturnal) (χ2 = 9.43, p = 0.002, OR 17.28). CHOP INTEND scores were available for 66% of infants, with a median score of 46 [16] out of 64. Table 1 provides a full listing of infant demographics and clinical characteristics.
Table 1 Sample demographics and characteristics (N = 69) Swallow biomechanics
Raters achieved scores corresponding to a Landis-Koch category of moderate or greater (kappa > 0.55) agreement in their reliability of analyzing all BabyVFSSImP© and ICCs of ≥ 0.72 for the Swallowtail components. While profound impairments in BabyVFSSImP© swallowing biomechanics were rare among infants who received pre-symptomatic treatment, they were common among infants treated after symptom onset. This was reflected in significantly worse (higher) scores in four BabyVFSSImP© domains (ts > 3.25, ps ≤ 0.01, δ > 0.42): Palatal-Pharyngeal Approximation, Airway Invasion/Laryngeal Closure, Aspiration, and Pharyngeal Transport and Clearance (Table 2). Specifications of the oropharyngeal swallowing biomechanics underlying these differences across treatment groups are outlined below, with a full listing of BabyVFSSImP© component scores provided in supplemental Table 2.
Table 2 Swallowing Biomechanics by Treatment Group (N = 69) Bolus Extraction: Though the majority (76%, N = 13) of infants who received pre-symptomatic treatment promptly initiated sucking when presented with the nipple, all but one had to suck > 3 times to express sufficient bolus to swallow. Prompt initiation of sucking tended to be less common in infants treated after symptom onset (40%, N = 21), with 55% (N = 28) of these infants not initiating sucking at all (χ2(1) = 3.59, p = 0.06, OR 0.28).
Bolus Clearance: Infants who received pre-symptomatic treatment rarely exhibited profound impairments in the ability to clear the ingested liquid from their pharynx, with no infants exhibiting profound impairments in pharyngeal constriction ratio (PCR > 0.2cm2), tongue base retraction, or pharyngeal residue, and only one infant exhibiting profound reductions in soft palate elevation (6%, N = 1) and pharyngoesophageal segment opening (6%, N = 1). Clinical specifications of those pre-symptomatic infants with profound impairments are outlined in Table 3. This was in contrast to infants treated after symptom onset, for whom a significantly higher proportion of infants (23–43%) exhibited profound impairments in these processes (BabyVFSSImP©, χ2(1) > 4.45, p ≤ 0.03, OR > 9.21; SwallowTail pharyngeal constriction ratio, fisher’s exact p = 0.03, OR = 0). These deficits in the propulsion of the bolus through the pharynx among infants treated after symptom onset were reflected in elevated Swallowtail pharyngeal constriction ratio values (symptomatic m = 0.15, sd = 0.16; pre-symptomatic m = 0.03, sd = 0.02; t (53.80) = 5.10, p < 0.001, d = 0.88). No differences were observed between groups in pharyngoesophageal segment opening duration (symptomatic m = 0.24, sd = 0.09; pre-symptomatic m = 0.22, sd = 0.06); t(40.04) = 0.84, p = 0.41, d = 0.20).
Table 3 Clinical Characteristics of Pre-Sympomatic Infants with Profound Swallowing Impairments Airway Protection: Penetration occurred in almost all infants in both pre-symptomatic (95%, N = 16) and symptomatic (90%, N = 47) treatment groups (p = 1). Although aspiration occurred less frequently, it was still commonly observed; occurring more frequently in infants treated after symptom onset (71%, N = 36) than pre-symptomatic (35%. N = 6, χ2(1) = 5.31, p = 0.02, OR 4.4). Interestingly, among those infants who aspirated, 17% (N = 7) were not reported to be exhibiting feeding difficulties, with VFSS’ done as part of high-risk referral (pre-symptomatic 67%, N = 4; symptomatic 8%, N = 3).
Swallow function
Although all pre-symptomatic treated infants were managing secretions without suctioning, and nearly all were consuming full age-appropriate nutrition (N = 15, 88%), similar to biomechanics, some pre-symptomatic treated infants did exhibit profound functional impairments. Clinical deficits among those pre-symptomatic treated infants who required alternative nutrition appeared 11 days following treatment, with the reason for tube provision ranging from swallowing deficits impeding safe oral nutrition to impairments in consuming sufficient oral nutrition to meet caloric requirements. Table 3 provides further specifications pertaining to the clinical conditions of those pre-symptomatic infants who exhibited profound impairments. Significantly more infants treated after symptom onset required suctioning for secretion management (38% vs 0%; fisher’s p = 0.002, OR 0) and were not consuming age-appropriate oral nutrition (50% vs. 12%; χ2 (1) = 17.33, p < 0.001, OR 20.35) than those treated pre-symptomatic. Table 4 provides a full listing of CEDAS scores.
Table 4 Children’s Eating and Drinking Activity Scale (CEDAS) Swallow biomechanics were associated with swallowing function, with the odds of an infant requiring suctioning for secretion management increasing significantly with increases in BabyVFSSImP© domain V: pharyngeal transport and bolus clearance scores (β = 0.30, z = 2.76, p = 0.006) and Swallowtail pharyngeal constriction ratio (β = 3.76, z = 1.83, p = 0.047). Among those domain V components, pharyngeal stripping wave was particularly predictive of suctioning needs (fisher’s exact p = 0.001, OR = 9.78). In contrast, the odds of an infant not achieving age-appropriate nutrition or hydration was significantly predicted by increases in domain I: lingual motion/swallow initiation (β = 0.26, z = 2.49, p = 0.013).
Continue Reading
-
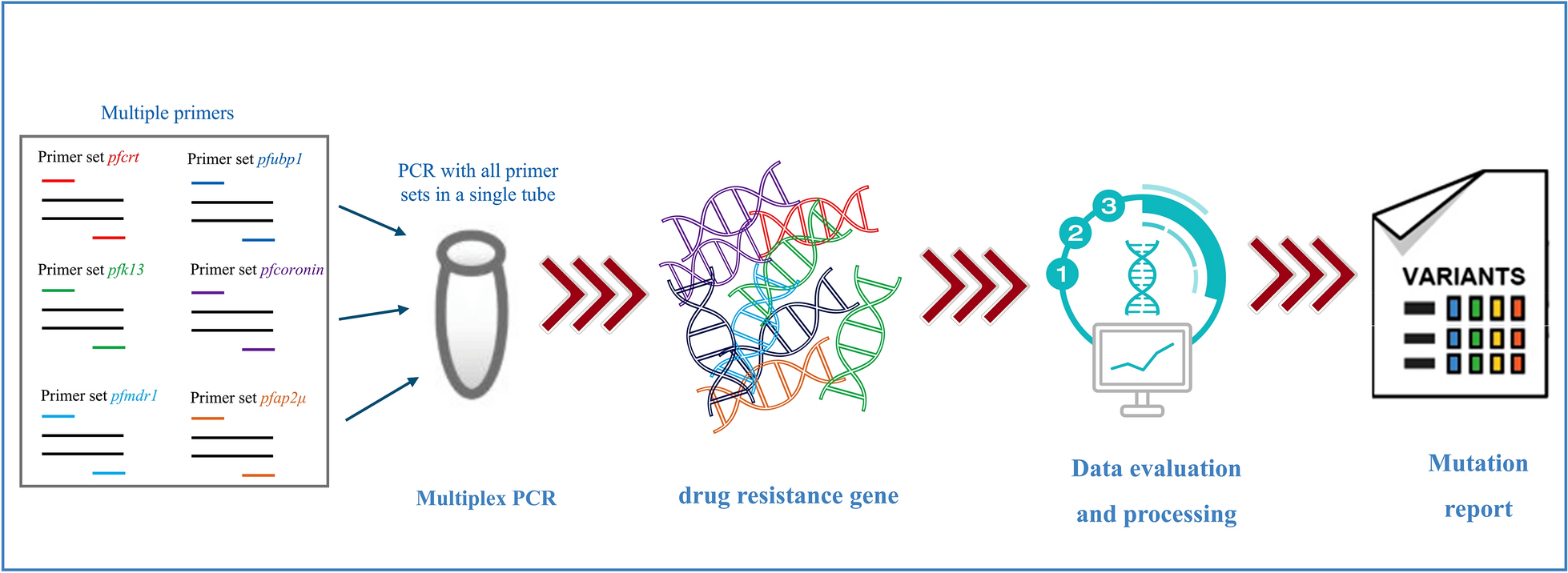
Multiplex long-amplicon sequencing for comprehensive molecular surveillance of Plasmodium falciparum resistance to artemisinin and partner drugs in artemisinin-based combination therapies (ACTs) | Parasites & Vectors
World Health O. World malaria report 2024: addressing inequity in the global malaria response. Geneva: World Health Organization; 2024.
Nosten F, White NJ. Artemisinin-based combination…
Continue Reading
-

Joke’s on you, fleshbag! Channel 4’s first AI presenter is dizzyingly grim on so many levels | Television
Last night’s Dispatches was called Will AI Take My Job? Usually when something like this employs a question mark in the title, it’s because the answer is no. Not this time, though, because the sheer overwhelming inevitability of AI taking our…
Continue Reading
-
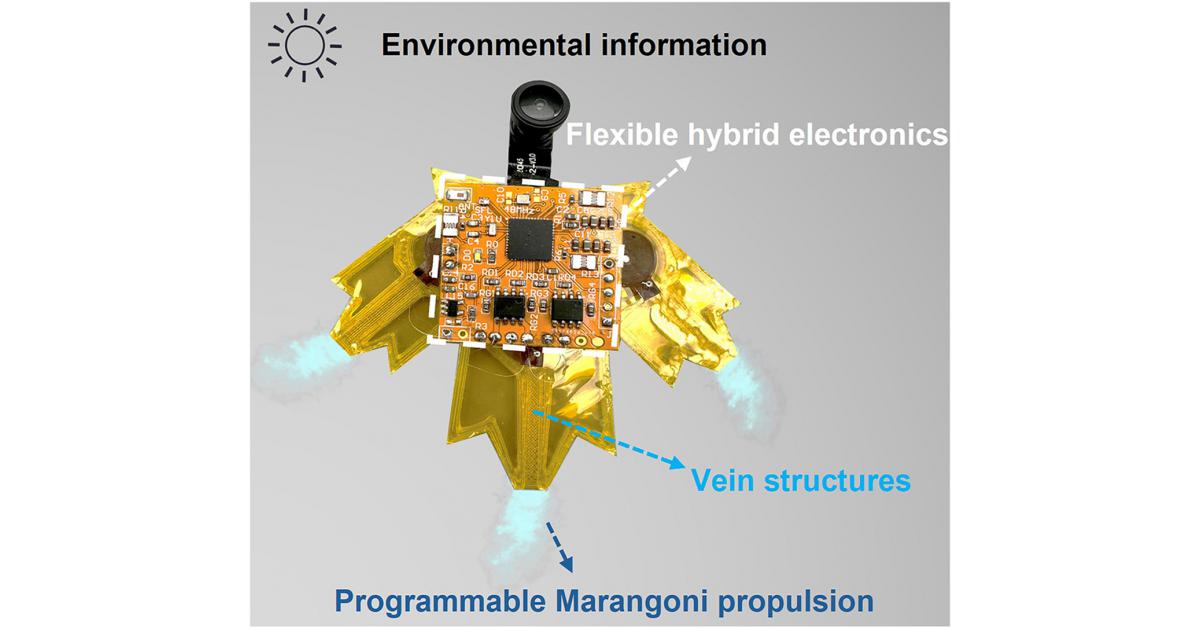
Smart aquabots bring camouflage and environmental sensing to life
Leaf-inspired aquabot with programmable propulsion and sensing.
GA, UNITED STATES, October 21, 2025 /EINPresswire.com/ — Small-scale robots designed to operate on water surfaces face challenges in mobility, adaptability, and…
Continue Reading