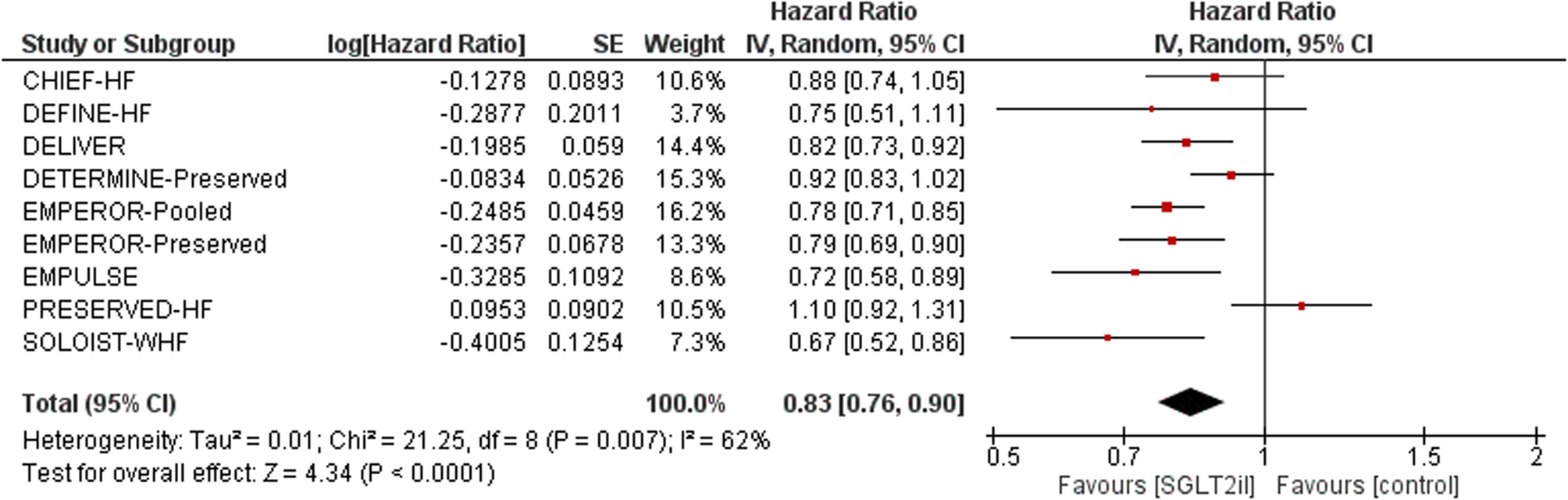
This meta-analysis demonstrates that SGLT2 inhibitors confer significant benefit in patients with HFpEF by reducing the composite outcome of cardiovascular death or hospitalization for heart failure. These findings align with major trials such as EMPEROR-Preserved and DELIVER [5, 8]. The reduction in HF hospitalization is particularly meaningful, reflecting an important improvement in morbidity for this complex patient population.
The lack of a statistically significant effect on all-cause mortality, despite a favorable trend, merits careful interpretation. This observation likely reflects the heterogeneity of HFpEF phenotypes and the limited modulation of natriuretic peptides observed in this subgroup, as noted in recent evidence.¹⁷ Even in advanced HFrEF, where stronger mortality signals have been observed, SGLT2 inhibitors may exert their benefits predominantly through metabolic and renal pathways rather than direct hemodynamic effects. This underscores the complexity in translating mechanistic improvements into mortality reductions, particularly in HFpEF [20, 21].
The use of an LVEF > 40% threshold in our inclusion criteria, though broader than the conventional ≥ 50% definition, was deliberately chosen to reflect contemporary trial designs and clinical practice patterns. This approach facilitates methodological consistency with EMPEROR-Preserved and DELIVER [5, 8]. and ensures that our findings are applicable to both HFpEF and the adjacent HFmrEF population; a clinically relevant spectrum where therapeutic options have historically been limited.
Recent meta-analytic data further illuminate the potential role of SGLT2 inhibitors in promoting favorable cardiac remodeling. Fan and Guo demonstrated that SGLT2i therapy significantly reduced left ventricular mass index, left atrial volume index, and E/e′ ratio, while modestly improving LVEF and lowering NT-proBNP levels [22]. Additional studies by Moras et al. and Alcidi et al. reinforce these findings, suggesting improvements in global longitudinal strain, myocardial mechanics, and diastolic function [21, 23]. While these surrogate endpoints do not directly translate into mortality reductions, they provide compelling mechanistic support for the clinical utility of SGLT2 inhibitors [21].
The modest improvement in KCCQ scores observed in our analysis complements the reduction in HF hospitalization risk and highlights the multidimensional benefit profile of SGLT2 inhibitors. The pooled mean difference of approximately + 1.8 points, while small, suggests a consistent effect on patient-reported symptoms and function, reinforcing their therapeutic relevance beyond hard clinical endpoints [2,3,4].
Our findings must be interpreted in the context of several limitations. We did not perform formal subgroup or sensitivity analyses by diabetes status, type of SGLT2 inhibitor, geographic region, or baseline patient characteristics, as stratified data were inconsistently reported across trials. This limitation reflects the inherent constraints of study-level meta-analysis and highlights the need for future patient-level meta-analytic approaches to assess potential treatment effect heterogeneity. Additionally, variability in baseline patient characteristics and trial inclusion criteria may have contributed to moderate statistical heterogeneity observed for the primary composite outcome.
In terms of potential bias, most included trials were methodologically rigorous with adequate randomization and allocation concealment. The principal sources of potential bias included incomplete outcome data from loss to follow-up and lack of blinding of outcome assessors, though these risks were generally low or moderate.
The absence of a significant effect on all-cause mortality contrasts with the substantial mortality reductions observed in large HFrEF trials such as DAPA-HF and EMPEROR-Reduced [4, 5], further underscoring differences in disease biology and therapeutic responsiveness between HF phenotypes. The benefits observed in these HFrEF trials, including reductions in cardiovascular death and HF hospitalization and improvements in KCCQ scores, provide important context for interpreting the more modest-but still clinically meaningful; effects seen in HFpEF [18].







