Osaka –
The first episode of “Future Kid Takara,” a new series of anime shorts, opens with the thrilling scene of a boy named Takara and a scientist named Dr. Amory…

The first episode of “Future Kid Takara,” a new series of anime shorts, opens with the thrilling scene of a boy named Takara and a scientist named Dr. Amory…
For most of us, Visual Studio Code is a text editor, a place to write code, preview Markdown, or maybe debug a script or two. But that perception barely scratches the surface. Over the last few years, VS Code has quietly evolved from being a…

In 10 days, voters will head to the polls on Election Day for a bevy of elections around the country, including key gubernatorial and mayoral races. In New York City, Democratic mayoral candidate Zohran Mamdani has been busy hitting the…

Arguably one of the most coveted (and charitable) nights of Halloween is none other than Bette Midler’s New York Restoration Project (NYRP) annual Hulaween—a spellbinding affair held in support of the city’s green spaces.
Last night marked…
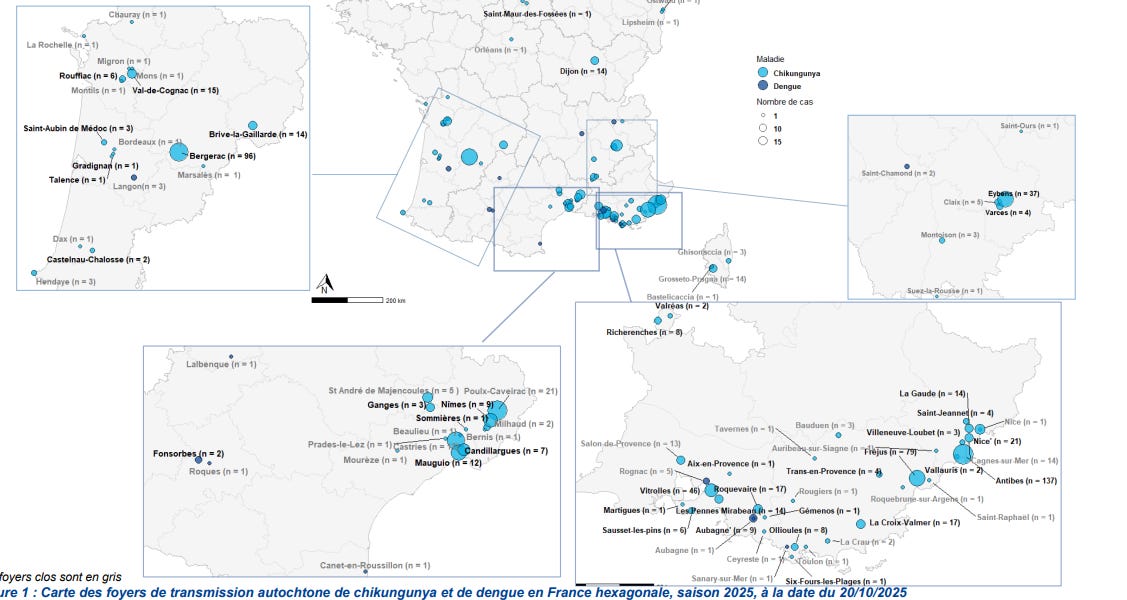
Sante publique France reports, as of October 20, 766 locally acquired chikungunya cases were reported in mainland France.
In addition, 29 local transmission of dengue fever have been reported this year.
91 outbreaks of indigenous vector-borne…

Investor sentiment around UP Fintech Holding (NasdaqGS:TIGR) has picked up after UBS and Jefferies each began covering the company with optimistic outlooks. The analysts highlighted the company’s foothold in expanding Hong Kong and Singapore wealth markets as well as its financial momentum.
See our latest analysis for UP Fintech Holding.
The upbeat analyst attention and momentum in Hong Kong and Singapore have helped fuel a stellar run for UP Fintech, with a 53.9% year-to-date share price return and a striking 1-year total shareholder return of 66.1%. Both the recent buzz and the longer-term track record, up 173% over three years, suggest that optimism around the company’s growth story is gaining traction among investors.
If fresh analyst optimism has you rethinking your watchlist, this could be the perfect moment to broaden your investing horizons and discover fast growing stocks with high insider ownership
But with shares already rallying this year and analyst targets suggesting more upside, the question is whether UP Fintech’s impressive growth is still underappreciated or if markets have already accounted for those future gains.
With the latest narrative valuing UP Fintech at $14.12, the gap versus the last close at $10.28 has caught attention. This fair value, calculated using a specific set of forward-looking earnings and margin assumptions, shapes the current debate around where the market might move next.
Strong growth in revenue, assets, and profitability; expansion into high-potential markets; and ongoing tech innovation position UP Fintech for durable, scalable, and diversified earnings.
Read the complete narrative.
Record margins, bold revenue forecasts, and a future earnings multiple are at the heart of this narrative. Want to see what assumptions drive this eye-catching target? The reasoning behind these numbers will surprise you.
Result: Fair Value of $14.12 (UNDERVALUED)
Have a read of the narrative in full and understand what’s behind the forecasts.
However, intensifying regulatory scrutiny and higher client acquisition costs in key markets could disrupt UP Fintech’s strong growth momentum and future profit forecasts.
Find out about the key risks to this UP Fintech Holding narrative.
If you think the numbers tell a different story or want to dig into the details yourself, you can craft your own take on UP Fintech in just a few minutes. Do it your way
A good starting point is our analysis highlighting 4 key rewards investors are optimistic about regarding UP Fintech Holding.
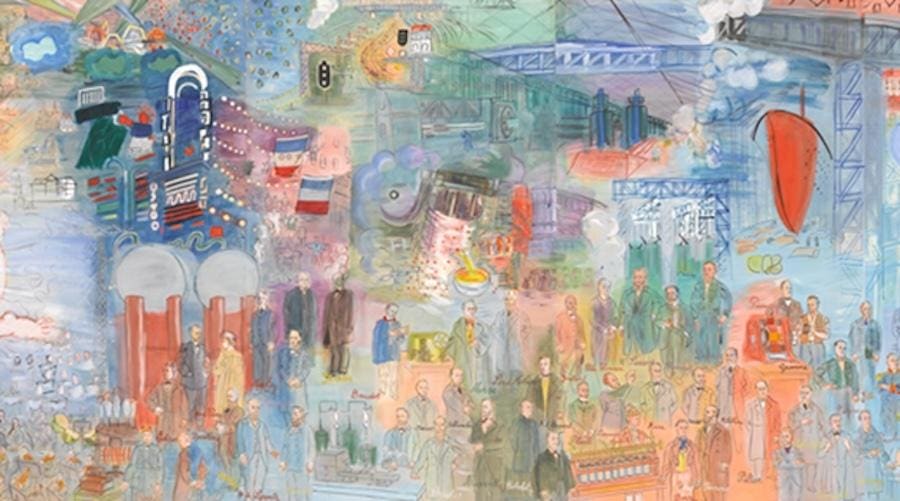
Samsung has announced that it’s secured a partnership with Paris’s famed Centre Pompidou museum that will bring no less than 25 of the gallery’s most famous and revered masterpieces to Samsung’s online digital Art Store, enabling Samsung…

SAN FRANCISCO, CA—The need for an implantable cardiac device before or after transcatheter tricuspid valve replacement (TTVR) does not appear to have a big impact on clinical outcomes, at least through the first year, according to an analysis of the TRISCEND and TRISCEND II studies.
After accounting for baseline differences between groups, patients who had a preexisting cardiac implantable electronic device (CIED) before TTVR or who required a new one after the procedure did not have a higher rate of all-cause death or hospitalization for heart failure (HF) at 1 year compared with those who didn’t need a device, Santiago Garcia, MD (The Christ Hospital, Cincinnati, OH), reported here during the WorldLink Forum at TCT 2025.
Moreover, CIEDs did not have an impact on reductions in the severity of tricuspid regurgitation (TR) with the procedure or measures of health status and function.
Lead discussant Kashish Goel, MD (Vanderbilt University Medical Center, Nashville, TN), emphasized the importance of showing no difference in hard outcomes, procedural efficacy in reducing TR, or health status changes across the groups. In addition, there was a low rate of lead malfunction, including no fatal cases, after TTVR.
What to do with CIEDs in the context of TTVR—including whether to extract the leads or “jail” them is a hot topic, Goel said, noting that about one-third of patients have preexisting leads at the time of the procedure.
“We should take a balanced approach in terms of what we’re going to do for these patients and not just say [that] jailing in everybody is okay,” he said.
Few Lead-Related Problems
With the emergence of transcatheter interventions for symptomatic severe TR, the interaction between TR and CIED leads that go through the tricuspid valve has gained more attention. Operators must decide whether to remove the leads or “jail” them—crushing them between the device and the native valve annulus—when performing TTVR. Jailing leads potentially damages them and could cause them to stop working properly.
In the current analysis, Garcia and his colleagues explored the safety and efficacy of TTVR using the Evoque system (Edwards Lifesciences) in patients with symptomatic severe TR with or without CIED leads using data from the single-arm TRISCEND study of patients with at least moderate-severity symptomatic TR and the randomized TRISCEND II trial of patients with severe or greater symptomatic regurgitation.
This analysis included 176 patients from TRISCEND and 259 from TRISCEND II who both underwent TTVR with the Evoque system and received optimal medical therapy. Mean patient age was nearly 80 years, and most participants (73%) were women. Slightly more than half did not require a CIED, 34.9% had a CIED in place before the procedure, and 12.6% needed a new CIED after the intervention.
At baseline, those with a preexisting CIED had a significantly higher EuroSCORE II and a lower LVEF compared with the other two groups, along with a higher prevalence of ischemic heart disease reflected by the nearly 20% rate of prior CABG. There were no significant differences across the three groups in the number of HF hospitalizations in the past year, median Kansas City Cardiomyopathy Questionnaire (KCCQ) overall summary score, or 6-minute walk distance. Echocardiographic measures of ventricular function and TR severity were similar across groups. Roughly half of patients had massive or torrential TR, and half had moderate or severe TR.
The researchers assessed outcomes in a 30-day landmark analysis to account for the timing of CIED implantation after TTVR. Before adjustment, the 1-year rate of all-cause death or HF hospitalization was higher in the patients with a preexisting CIED at the time of TTVR (25.4%) than in those who received a CIED after the procedure (15.9%) and those who did not require a CIED (15.0%).
However, after adjustment for potential confounders, which included sex, age, prior CABG, and right and left ventricular function, neither of the CIED groups had a higher risk of the composite outcome compared with the patients without a device (P = NS for both). Garcia said that indicates that the higher unadjusted rates observed in patients with preexisting CIED leads could be related to a higher burden of comorbidities at baseline—in particular, a high rate of ischemic heart disease and lower LVEF.
The efficacy of the procedure was similar across groups, with no significant differences in the proportion of patients who had a TR reduction by at least 2 grades (about 98% overall) and who achieved a TR grade of moderate or less (nearly 100% overall). There were similar proportions of patients who improved by at least one NYHA class and who had a gain in their 6-minute walk distance of at least 30 meters. Mean KCCQ overall summary score was about 73 points.
Lead-related problems among the 152 patients with a preexisting CIED were infrequent, occurring in 10 patients (6%). In six cases, the issue was corrected with placement of a new lead or repositioning of the existing lead. There were two cases addressed by a change in device programming and two involving medical management or no intervention.
The findings should be interpreted in light of some limitations, Garcia said. The investigators excluded patients with pacemaker dependency who did not have an alternative pacing option and those with an RV pacing lead placed within 90 days of the procedure. In addition, events that occurred prior to randomization, such as CIED lead extraction, were not captured and the analyses did not examine periprocedural events occurring in the first 30 days.
Moreover, there was a lack of longer-term data, which will be needed to better understand the potential risks of jailing leads during TTVR, Garcia said.
When considering the approach to these patients, it’s important to consider patient factors like age, pacemaker dependence, infection risk, and the contribution of lead placement to TR, as well as anatomical factors like slack in the lead and lead location, Goel indicated.
In addition, he said, “the expertise of the electrophysiologist in the practice will be important to make sure we have a risk-benefit analysis of what’s the best strategy for that patient.” And finally, longer-term follow-up beyond 1 to 2 years is critical to determine whether jailing CIED leads during TTVR will be safe for patients, Goel said.

Max Verstappen is anticipating a “difficult” race from P5 on the grid at the Mexico City Grand Prix, with the Dutchman admitting that the “whole weekend has been tough” so far at the Autodromo Hermanos Rodriguez.
Despite topping the…

Lewis Hamilton believes that “P3 is kind of the perfect spot at this track” to challenge for the lead at the start of the Mexico City Grand Prix after his best Saturday Qualifying performance since joining Ferrari.
The seven-time World Champion…