
How are we enjoying the “normal seasonal soft patch” so far? The stock market spent the past week chopping around the range left by the sharp drop the prior Friday, while confronting the ghosts of crises past: regional-bank balance-sheet worries , possible re-escalation of China trade hostilities, a crypto flash correction and a reversal in the most speculative and fundamentally flimsy stocks. The S & P 500 managed a 1.7% weekly gain, almost all of it coming from Monday’s reflex rebound, carving out what now amounts to a five-week trading range bounded by the all-time high above 6,750 and the twice-tested low of 6,550. Entering last week, nearly early everyone lining up behind the consensus bullish argument pointed to the AI-investment bonanza, a Federal Reserve poised to cut rates twice more this year into a still-firm economy and the heaven-bestowed right to a year-end performance-chasing rally. Along with these hard-to-dispute premises would come the standard disclaimer that one should be ready for some October volatility along the way. We’ve now had some of that, though the net effect so far is the mildest of pullbacks, just shy of 3% at the worst from a record high. But last week saw an observable upwelling of anxiety, reflecting a break of the preceding low-volatility climb and some possible pent-up selling from historically elevated equity allocations. Investors all-in The upward march in the indexes has pushed the aggregate equity allocation of Bank of America’s high-net-worth clients up to 64%, just shy of the two-decade high set in late 2021. This suggests less need to top up stock balances, even if they have wanted to, with inflows to equity funds from wealthier households heavy in recent months. Long-short hedge funds, after failing to capture much of the initial surge off the April correction lows, had largely “re-risked” into last week, based on cycle-high gross and net leverage among BofA’s prime-brokerage customers. The tactical fast-money players no doubt backed away in the past week, as they confront the annual fourth-quarter choice either to lock it in or let it ride. Goldman Sachs head of hedge-fund coverage, Tony Pasquariello, says, this cohort last week executed “the largest selling of both US and global equities since April (with a big increase in macro shorts),” adding that “while I believe there’s still plenty of length held by a variety of market actors, the fact is the market did clean up some risk over the past two weeks — and, as we move through October, I believe the technicals will improve.” It’s impossible to prove, but it seems the market has also suffered a bit from a confluence of anniversaries and milestones causing investors to recognize how generous the market has been. The third anniversary of this bull market just passed, with the S & P 500 having compounded at a 24% annual pace over that span, lifting valuations to the upper edge of the post-pandemic range. We also crossed the six-month mark since the April tariff-panic low, pushing a 40% burst from low to high. And in recent weeks the S & P 500 surpassed 6,666 for the first time, registering a ten-bagger since the financial-crisis bottom of 666 set in March 2009. The index crossed that level in each of the past six trading days and closed Friday two points below. First sign of volatility in a while Such nostalgic atmospherics aside, the drop from the record high has likely felt worse than it looks on a chart because it punctuated an unusually long stretch of sleepily rising prices. Before Oct. 10, it had been 48 days since the prior 1% S & P 500 daily decline. That slide also ended the longest-ever streak that saw the index stay above its 20-day moving average. And the index had gone 123 days since the last 3% pullback, one of the dozen longest runs on record, according to 3Fourteen Research founder Warren Pies – and the gain over that period was the best of any such streak at the 123-day mark. Reassuringly, Pies crunched the numbers on what followed past such streaks, and concludes that such calm ascents rarely come at the very end of a bull market. And the subsequent market performance following a busted streak has been a good deal better when the Fed’s next move was a cut rather than a hike. It’s quite possible, even if the recent slippage is not the start of a severe tailspin, that the interruption of the harmoniously rotating, low-drama uptrend let the volatility goblin loose for a while. The Cboe S & P 500 Volatility Index and the futures tied to it saw a much larger jump than one would expect given the relatively mild index setback, the VIX jumping from 16 on Oct. 9 to a high above 28 on Friday before receding below 21. .VIX YTD mountain Cboe Volatility Indes, YTD This promises to put in a nice spike on the chart if the sort that can mean the anxiety attack is waning and a tactical buy-the-dip signal might be flashing. Or perhaps the AI excitement and recent wild momentum stampedes into and out of speculative thematic subsectors means we could be in for a jumpier phase of the bull market. Three weeks ago, when spit-balling about what signs might accompany the acceleration into a more euphoric environment, I noted : “Another feature of markets growing toward an unstable bubbly episode is volatility rising along with stock prices – counter to the broad inverse interplay. The excitable, erratic flows in 1999 drove such a phenomenon, the CBOE Volatility index rarely dropping below 20 as the S & P 500 rallied 20% and the Nasdaq Composite soared 85%.” Too early to declare this is where we are now, but it can’t be dismissed. Credit worries Volatility can also be manifesting the flareup of credit concerns related to losses in a confluence of “one-off” commercial bankruptcies (in part chalked up to alleged fraud), fed into a simmering unease with somewhat loose non-bank lending and opaque structures in the fast-growing private-credit realm. We have had more false alarms than real ones when it comes to selloffs shadowed by credit-contagion fears, but if nothing else the price action in alternative asset managers, regional banks and the investment bank Jefferies Financial have undermined the comfort many investors were taking in historically tight corporate-debt spreads. Hints of a souring credit cycle matter most to equities because they would work against the consensus view that the Fed will be cutting rates a bit more for “the right reasons” into a still-sturdy economy. The same goes for the rhetorical escalation of trade hostilities between the U.S. and China. To remain aggressively bullish now, one must opt for the bright-side interpretation of a few apparent paradoxes. One is that divide between isolated commercial-credit weakness and still-healthy indicators of corporate creditworthiness. Another is the divide between the GDP tracking models showing above-trend growth while all job-market indicators are near stall speed. A third is the tenacious strength in gold , traditionally a risk-off asset that feeds off fears of calamity but recently a globally embraced momentum trade and “universal diversifier” against elevated equities, a surplus of government debt, a less-trustworthy U.S. dollar and cryptocurrencies that move with techno-enthusiasm. @GC.1 YTD mountain Gold, YTD Coming into Friday, traders were unsettled by the recent moves lower in stocks, Treasury yields, the dollar and crude oil – disinflationary, decelerating-growth signals – along with the unceasing buying of gold even at grossly extended prices. In this context, the metal’s $100 slide on Friday from a record above $4,380 an ounce came as a mild relief to equity traders. Whether this triggers a more disorderly unwind in gold remains to be seen, of course, and there’s no telling how stocks might correlate to such a reversal. Do we need a proper scare? Not on the same scale, but some of the more overheated meme-like stocks have been punctured without much apparent disruption to the large-cap core of the market. Quantum-computing playthings IonQ and Rigetti Computing both fell more than 20% in two days after monstrous rallies, and Robinhood shares have lost 15% in six trading days. With any luck, attention can turn next week to more fundamentally grounded matters. Earnings reporting starts to pick up in coming weeks, with year-over-year growth expected to exceed 8% (14.9% for the Magnificent 7 and 6.7% for the rest), according to FactSet. It’s tough for the economy and market to get into all that much trouble with profits and profit forecasts still on the rise, and with a U.S. federal deficit still near 6% of GDP. Last week’s action never broke the bounds of a purely routine consolidation, though it also settled nothing in particular. Scrutinizers of the tape were flagging relatively weak market responses to great Taiwan Semiconductor results and Oracle’s ecstatic growth outlook. There were more 52-week lows than highs on both major exchanges on Friday. The bounce in financial stocks Friday wasn’t all that emphatic; this group has much to prove with the sector barely above its high from late 2024. And is it a bit too trite for the S & P 500 to undergo its first noticeable pullback in six months and have it halt a mere point above the 50-day moving average, as it did at last Tuesday’s low? An ideal scenario for the remainder of the year would have the recent choppiness last a bit longer to qualify as a proper scare, skimming the froth off the speculative stuff and resetting expectations in a way that rebuilds investors’ capacity to be surprised to the upside.
Blog
-

Belzutifan Plus Pembrolizumab and Lenvatinib Demonstrates Potential in Advanced Clear Cell RCC
Treatment with belzutifan (Welireg) plus pembrolizumab (Keytruda) and lenvatinib (Lenvima) improved efficacy outcomes compared with multiple other pembrolizumab-based triplet regimens in patients with advanced clear cell renal cell carcinoma (ccRCC), according to findings from substudy 3A of the phase 1/2 KEYMAKER-U03 trial (NCT04626479) presented at the
2025 ESMO Congress .Providing the background for the study, Cristina Suarez Rodriguez, MD, PhD, of Vall d’Hebron University Hospital, Barcelona, Spain, said, “First-line triplet regimens adding novel mechanisms of action to standard doublet therapy may be a promising approach for advanced clear cell renal cell carcinoma…The potent and selective HIF-2α inhibitor belzutifan is a treatment for advanced RCC following prior anti-PD-(L1) and VEGFR-TKI therapy, and may be a highly suitable candidate for novel triplet therapy in the first-line setting.”
For substudy 3A (NCT04626479) of the umbrella phase 1/2 KEYMAKER-U03 trial, investigators sought to evaluate novel pembrolizumab-based regimens as first-line treatment for advanced ccRCC.
“The study employed an adaptive design in which experimental arms were added and/or inactivated on a rolling basis with a continuous enrolling reference arm. Experimental arms each had a safety lead-in phase of 10 patients,” Suarez Rodriguez explained.
Patients with histologically confirmed locally advanced or metastatic ccRCC as measurable by RECIST v1.1, no prior systemic therapy for advanced RCC, and a KPS score of at least 70% were eligible for the study. Following the safety lead-in phase, the study entered the randomized phase. In this phase, patients were randomly assigned to 2:1 to 1 of 5 arms. Arm 1 included coformulated favezelimab/pembrolizumab 800mg/200 mg intravenously every 3 weeks, and lenvatinib 20 mg orally once daily. Arm 2 included coformulated vibostolimab/pembrolizumab 200/200 mg IV every 3 weeks plus belzutifan 120 mg orally once daily. Arm 3 included coformulated quavonlimab/pembrolizumab 25 mg/400 mg IV every 6 weeks plus lenvatinib 20 mg orally once daily. Arm 4 included belzutifan 120 mg orally once daily plus pembrolizumab 400 mg IV every 6 weeks, plus lenvatinib 20 mg orally once daily. A concurrent reference arm included pembrolizumab 400 IV every 6 weeks plus lenvatinib 20 mg orally once daily.
Primary end points were overall responsive rate (ORR) as measured by RECIST v1.1 by blinded independent central review (BICR), as well as safety. Secondary end points included duration of response (DOR) and progression-free survival by RECIST v1.1 by BICR, as well as overall survival (OS).
Suarez Rodriguez reported ORR for the arms as follows:
• Arm 1: At a median follow-up of 39.2 months (range, 28.8-44.6 months), ORR was 62.7% (95% CI: 48.1-75.9).
• Arm 2: At a median follow-up of 16.4 months (range, 11.8-23.4 months), ORR was 42.5% (95% CI: 31.5-54.1).
• Arm 3: At a median follow-up of 22.1 months (range, 13.5-40.6 months), ORR was 71.3% (95% CI: 60.0-80.8).
• Arm 4: At a median follow-up of 23.4 months (range, 14.1-41.0 months), ORR was 77.5% (95% CI: 66.8-86.1).
• Reference arm: At a median follow-up of 21.2 months (range, 11.9-44.4 months), ORR was 80.6% (95% CI: 68.6-89.6).
Complete response was observed in 5 (9.8%), 4 (5.0%), 5 (6.3%), 10 (12.5%), and 4 (6.5%) patients across the respective arms.
In arm 1, DOR and PFS were found to be numerically similar to the reference arm, Suarez Rodriguez reported. The treatment regimen of arm 2 was found to be not superior to the reference arm. For arm 3, median DOR was 25.0 months (range, 2.4-37.1+ months) in arm 3 and 25.6 months (range, 1.4+-27.6 months) in the reference arm.
Arm 4 “showed a median duration of response of 33 months vs 26 months in the reference arm,” Suarez Rodriguez said. Median PFS was 31.8 months (95% CI: 26.3-NR) in arm 4 vs 20.8 months (95% CI: 12.4-29.0) in the reference arm (HR, 0.45, 95% CI: 0.25-0.83). OS was not reached in either arm.
Suarez Rodriguez also discussed safety across the regimens. Arm 1 had the highest incidence of grade 3 or higher adverse events (AEs) (86.9%), followed by arm 3 (73.3%), the reference arm (71.0%), arm 4 (70.0%), and arm 2 (68.9%). Arm 1 had the highest rate of treatment-related AEs (37.7%), followed by arm 3 (34.4%), arm 2 (31.1%), the reference arm (30.6%), and arm 4 (24.4%). Serious treatment-related AEs were highest in arm 1 (36.1%) followed by arm 3 (34.4%), the reference arm (30.6%), arm 2 (27.8%), and arm 4 (22.2%).
“As expected, the most common adverse event observed in the combination arms containing lenvatinib was hypertension. The most common adverse event in the combinations containing belzutifan was anemia,” Suarez Rodriguez said.
“In conclusion, observed efficacy of pembrolizumab plus lenvatinib were confirmatory of prior observations for this combination. Belzutifan/pembrolizumab plus lenvatinib and the anti-CTLA-4 combination had similar overall response rate compared to pembrolizumab/lenvatinib as first-line therapy in patients with previously untreated advanced clear cell renal cell carcinoma. Responses were potentially less favorable in the anti-LAG-3 and anti-TIGIT arms. Belzutifan plus pembrolizumab plus lenvatinib, but not the other investigative arms, may have been associated with a higher proportion of complete response, prolonged duration of response, and prolonged progression-free survival compared to pembrolizumab plus lenvatinib,” Suarez Rodriguez said in her concluding remarks.
Suarez Rodriguez also noted that belzutifan plus pembrolizumab plus lenvatinib and quavonlimab/pembrolizumab plus pembrolizumab are being evaluated in the phase 3 LITESPARK-012 study (NCT047367706).
DISCLOSURES: Suarez Rodriguez noted research funding and medical writing support from Merck Sharp & Dohme (MSD) LLC; research funding from Bristol Myers Squibb, Ipsen, Pfizer, and Roche; advisory board membership with Astellas, AstraZeneca, Bristol Myers Squibb, and MSD; travel accommodations from Bayer, speakers’ bureau membership with AstraZeneca, Astellas, Bristol Myers Squibb, Ipsen, and MSD; an invited speaker for Bristol Myers Squibb and MSD; and expert testimony for Bristol Myers Squibb and MSD.
Reference
1. Suarez Rodriguez C, Rojas CI, Shin SJ, et al. First-line pembrolizumab-based regimens for advanced clear cell renal cell carcinoma: KEYMAKER-U03 substudy 03A. Presented at: European Society for Medical Oncology Congress. October 17-21, 2025. Berlin, Germany. Abstract LBA96. https://s3.eu-central-1.amazonaws.com/m-anage.com.storage.esmo/static/esmo2025_abstracts/LBA96.html.pdf
Continue Reading
-

Single Gene Swap Transfers Courtship Behavior Between Two Species For The First Time
Researchers have engineered a courtship ritual from one species of fruit fly into another using genetic modification.
A Japanese research team tweaked a single gene in the fly Drosophila melanogaster, causing it to display a courtship ritual…
Continue Reading
-

Lilah Fear/Lewis Gibson take spicy route to rhythm dance lead; Guillaume Cizeron finds “magic” on comeback
Cizeron not flawless but finds “magic” in comeback
France’s Guillaume Cizeron is no stranger to feeling victorious on Grand Prix de France ice, having won this Grand Prix stage a record six times with his former partner Gabriella…
Continue Reading
-

Lenvatinib/Everolimus Beats Cabozantinib in Phase 2 RCC Study
The combination of lenvatinib (Lenvima) and everolimus (Afinitor) reduced the risk of progression or death by 49% compared with cabozantinib (Cabometyx) for patients with metastatic clear cell renal cell carcinoma (ccRCC) following progression on a PD-1 inhibitor, according to findings from a phase 2 study presented at the
European Society for Medical Oncology Congress 2025 and simultaneously published in the Annals of Oncology.1,2In the multicenter phase 2 study, the median progression-free survival (PFS), which was the primary end point of the study, was 15.7 months with the combination of lenvatinib plus everolimus compared with 10.2 months with cabozantinib (HR, 0.51; 95% CI, 0.29-0.89; P = .02). There were more adverse events (AEs) observed with the combination, but these differences were not deemed statistically significant. Grade 3/4 AEs were experienced by 67.5% of those treated with lenvatinib plus everolimus compared with 50% of those receiving cabozantinib (odds ratio [OR], 2.08; 95% CI, 0.86-5.02).
“Lenvatinib plus everolimus significantly prolonged progression-free survival over cabozantinib,” Andrew W. Hahn, MD, Department of Genitourinary Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, said during a presentation of the results. “As the first head-to-head randomized comparison of contemporary second-line or later treatments after immune checkpoint inhibition, these results are relevant to treatment sequencing and inform oncology practice.”
The study enrolled 86 patients, with 40 receiving the combination and 46 receiving cabozantinib. For the combination arm, lenvatinib was administered at 18 mg per day and everolimus was given at 5 mg per day. Cabozantinib was administered at 60 mg per day. The most common prior treatment was the combination of nivolumab (Opdivo) and ipilimumab (Yervoy), which was received by 70.9% of patients enrolled in the study. This was followed by the combination of pembrolizumab (Keytruda) and axitinib (Inlyta) for 16.3%, adjuvant pembrolizumab for 4.7%, and any other checkpoint inhibitor for 8.1%.
Baseline characteristics were well balanced between the groups with most patients (69.8%) in each group having received 1 prior line of therapy and 30.2% having received 2 prior lines of therapy. Nearly half of patients had received prior VEGF-targeted therapy (45% for the combination arm and 41.3% for the single agent group). The IMDC risk was primarily intermediate in both groups (80% for combination and 73.9% for single agent). The IMDC risk was poor for 7.5% of those in the combination arm and for 8.7% of those in the control arm.
The objective response rate was 52.6% with lenvatinib plus everolimus compared with 38.6% with cabozantinib. Although numerically higher, this rate did not pass the bar for statistical significance (OR, 1.87; 95% CI, 0.75-4.6; P = .17). In addition to responses, stable disease was observed in 39.5% of those receiving the combination and for 54.5% of those in the single-agent arm.
The study was not designed to assess differences in overall survival (OS) and findings for this end point were still immature, Hahn noted. After a median of 20 months of follow-up, there had been 11 events in the combination arm and 13 in the control group. The 1-year OS probability was 87.0% with lenvatinib plus everolimus compared with 84.6% with cabozantinib (HR, 1.05; 95% CI, 0.47-2.38; P = .86).
Serious AEs were experienced by 27.5% of those treated with lenvatinib plus everolimus compared with 19.6% of those in the cabozantinib arm (OR, 1.56; 95% CI, 0.57-4.24). Dose interruptions were necessary for 70% of those in the combination arm compared with 78.3% of those in the cabozantinib group (OR, 0.65; 0.24-1.73). Dose reductions were necessary for 57% and 60.9% of those in the combination and control arm, respectively (OR, 0.80; 95% CI, 0.33-1.93). Treatment discontinuation was more common in the combination group at 20% compared with the single agent at 10.9% (OR, 2.05; 95% CI, 0.61-6.91).
“Of the 8 patients who discontinued treatment with lenvatinib plus everolimus, 5 of those were due to proteinuria,” said Hahn.
The most commonly observed AEs in the study aligned with those historically associated with each agent, Hahn noted. For the combination and single agent arms, respectively, the most common all-grade AEs were diarrhea (70% vs 73.9%), fatigue (72.5% vs 60.9%), proteinuria (65% vs 37%), hypertension (57.5% vs 39.1%), nausea (40% vs 39.1%), palmar-plantar erythrodysesthesia (20% vs 52.2%), vomiting (32.5% vs 34.8%), and oral mucositis (15% vs 43.5%).
“This is a positive phase 2 trial and demonstrates improved PFS and response compared with cabozantinib, but with higher toxicity,” said invited discussant Lisa M. Pickering, consultant medical oncologist at The Royal Marsden, MD, PhD, FRCP. “So, is it positive enough? I think that depends on you and your patient, but I would say that we can and should consider using lenvatinib/everolimus, particularly in patients for whom the priority is response and to who the toxicity rate is acceptable.”
The combination of lenvatinib and everolimus was approved by the FDA in 2016 for the treatment of patients with advanced RCC after a prior anti-angiogenic agent.3 The phase 2 study was completed to assess the combination in a more contemporary treatment setting, Hahn noted.
References
- Hahn AW, Chahoud J, Skelton W, et al. LenCabo: A randomized phase II multicenter trial of lenvatinib plus everolimus (len/eve) versus (vs) cabozantinib (cabo) in patients (pts) with metastatic clear cell RCC (ccRCC) that progressed on PD-1 immune checkpoint inhibition (ICI). Presented at: 2025 ESMO Congress; October 17-21, 2025; Berlin, Germany. Abstract LBA94.
- Hahn AW, Chahoud J, Skelton WP, et al. A multicenter randomized phase II trial of lenvatinib plus everolimus versus cabozantinib in patients with metastatic clear cell RCC that progressed on PD-1 immune checkpoint inhibition (LenCabo). Ann Oncol. 2025. Doi:10.1016/j.annonc.2025.10.009.
- Lenvatinib in combination with Everolimus. FDA. May 16, 2016. Accessed October 18, 2025. https://www.fda.gov/drugs/resources-information-approved-drugs/lenvatinib-combination-everolimus
Continue Reading
-
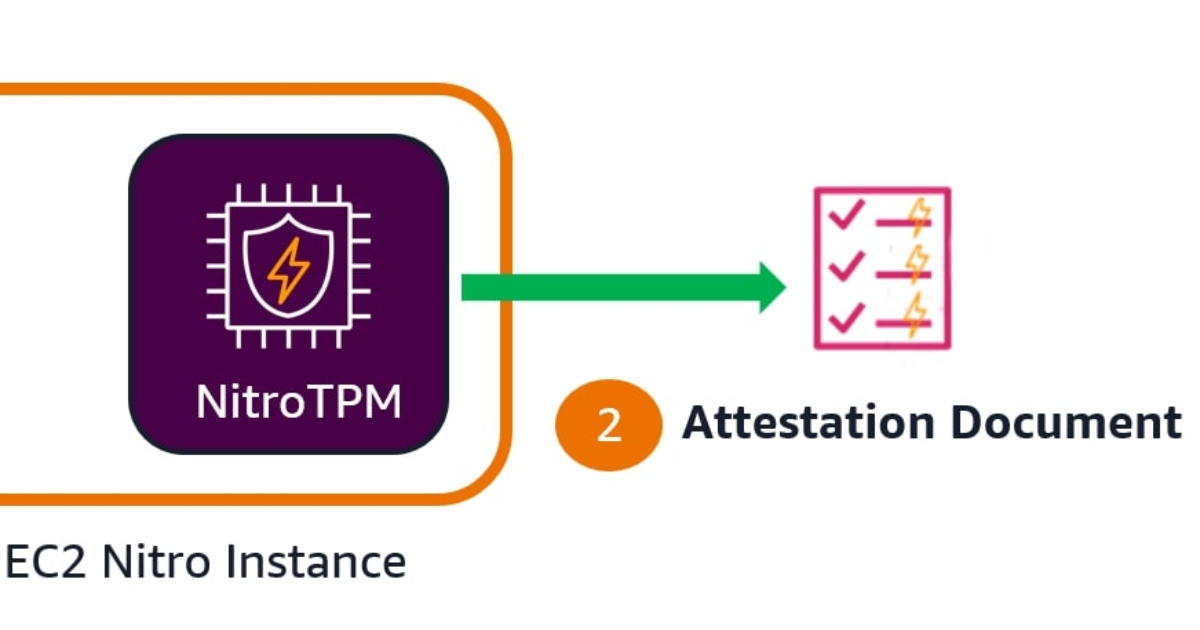
AWS Introduces EC2 Instance Attestation
AWS has introduced EC2 instance attestation, a new security feature that enables customers to verify that their virtual machines are running approved software configurations in a cryptographically secure manner. The capability is powered…
Continue Reading
-

How Dr. Barbara Sturm Turned Glowing Skin Into a Global Empire
It’s a summery Monday in Gstaad, and Dr. Barbara Sturm has just finished an afternoon of tennis with her younger daughter, Pepper, who recently turned 11. But if the renowned skincare guru is at all worn out from the sun—or from trying to…
Continue Reading
-

Update Microsoft Windows Now — New 2 Week Security Deadline Confirmed
Update Windows 10 and 11 security now, CISA demands.
NurPhoto via Getty Images
Updated October 18 with expert comment regarding CVE-2025-24990, which is now confirmed as residing in “legacy code installed by default on all Microsoft Windows…
Continue Reading
-
Scientists Discover Rogue Star-Eating Black Hole Far From Home
Welcome back to the Abstract! Here are the studies this week that mounted a defense, felt out of place, found new life, and resurrected the gods of yore.
First, a tale of pregnant stinkbugs, parasitic wasps, and fungi weapons that…
Continue Reading
