More focus is needed on female-specific barriers to enrollment and completion of programs that can improve their outcomes.
Despite evidence to support the role that cardiac rehabilitation can play in improving outcomes after serious…

Despite evidence to support the role that cardiac rehabilitation can play in improving outcomes after serious…
This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!
SAN JOSE, Calif. — October 22, 2025 — QuantumScape Corporation (NYSE: QS), a global leader in next-generation solid-state lithium-metal battery technology, today announced that it has begun shipping B1 samples of its QSE-5 cell. The company reached this milestone during the third quarter of 2025, achieving one of the company’s key goals for the year.
These samples are the most advanced QS cells to date and feature separators produced using the company’s groundbreaking Cobra process. By combining the high-performance QSE-5 design with more efficient production processes, these cells represent a major step toward high-volume commercial production of QS technology for electric vehicles and other applications.
Cobra-based QSE-5 cells are featured in QS’s first vehicle program with the VW Group, the Ducati V21L motorcycle. The Ducati program is designed as a real-world demonstration of the no-compromise performance profile of QS solid-state battery technology.
This cell shipment milestone reflects QS’s commitment to executing on its roadmap and advancing next-generation battery technology. In a further step toward bringing QS technology to scale and achieving automotive-grade reliability, the company is installing a highly automated cell production pilot line, the Eagle Line, at its headquarters in San Jose, California.
“We are proud to announce the start of deliveries of these QSE-5 samples,” said Dr. Luca Fasoli, Chief Operating Officer of QS. “We are working together with our partners to bring our groundbreaking solid-state lithium-metal battery technology to market as quickly as possible. This announcement is another critical step toward achieving our goal of revolutionizing energy storage.”
###
About QuantumScape Corporation
QuantumScape is on a mission to revolutionize energy storage to enable a sustainable future. The company’s next-generation solid-state lithium-metal battery technology is designed to enable greater energy density, faster charging and enhanced safety to support the transition away from legacy energy sources toward a lower carbon future. For more information, visit www.quantumscape.com.
Forward-Looking Statements
Certain information in this press release may be considered “forward-looking statements,” within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended, including, without limitation, statements regarding the development, commercialization, and high-volume scale-up of QS’s battery technology, the anticipated benefits from successful installation and operation of production equipment for the Eagle Line, including battery cell reliability and increased production automation, the performance of QS’s technology and its applications, the achievement of technical milestones and goals, and the potential impacts of QS’s technology for electric vehicles and other applications, among others. These forward-looking statements are based on management’s current expectations, assumptions, hopes, beliefs, intentions and strategies regarding future events and are based on currently available information as to the outcome and timing of future events. Because forward-looking statements are inherently subject to risks and uncertainties, some of which cannot be predicted or quantified, you should not rely upon forward-looking statements as predictions of future events. The events and circumstances reflected in the forward-looking statements may not be achieved or occur and actual results could differ materially from those projected in the forward-looking statements due to various risks, including the successful development and commercialization of our solid-state battery technology, achieving technical and financial milestones, building out of high-volume processes and otherwise scaling production, achieving the performance, quality, consistency, reliability, safety, cost and throughput required for commercial production and sale, changes in economic and financial conditions, market demand for EVs, retaining key personnel, competition, regulatory changes, broader economic conditions, and other factors, including those discussed in the section titled “Risk Factors” in our Annual Report and Quarterly Reports and other documents filed with the Securities and Exchange Commission from time to time. Except as otherwise required by applicable law, the company disclaims any duty to update any forward-looking statements.
Long Beach, Calif. October 22, 2025 – Rocket Lab Corporation (Nasdaq: RKLB) (“Rocket Lab” or “the Company”), a global leader in launch services and space systems, today announced the clearance of their Systems Integration Review (SIR) and completion of their Photon spacecraft for Eta Space and NASA’s LOXSAT mission. LOXSAT is an on-orbit technology demonstration of a cryogenic fluid management system, that will inform the design of Cryo-Dock, a full-scale cryogenic propellant depot in low Earth orbit to be operational in 2030.
The SIR, completed in September, marked a key milestone for the program, allowing the team to proceed with payload integration. Rocket Lab will now move the mission into environmental testing – the next phase before its launch on Electron in early 2026.
Rocket Lab was selected in 2020 by Eta Space to provide both the spacecraft and its Electron launch vehicle for the LOXSAT mission, joining a growing list of spacecraft-plus-launch mission solutions supported by the Company, including the CAPSTONE lunar mission for NASA and the upcoming VICTUS HAZE mission for the U.S. Space Force. Rocket Lab’s end-to-end capabilities simplify mission execution and minimize cost and schedule risks, providing customers with a single, responsive space solutions partner for a wide range of mission objectives.
“We’re proud to be both the spacecraft and launch provider for LOXSAT and for the opportunity to show Rocket Lab’s true end-to-end space systems capabilities,” said Brad Clevenger, Vice President of Space Systems. “With LOXSAT, we’re supporting a critical technology demonstration that will enable key steps toward making orbital propellant depots a reality. The ability to refuel in space is fundamental to unlocking reusable and sustainable exploration beyond Earth’s orbit. With the spacecraft build and payload integration complete, our team is focused on environmental testing ahead of its launch on Electron.”
“We are excited to reach this milestone”, said Bill Notardonato, CEO of Eta Space. “We chose Rocket Lab as a launch provider based on their proven Electron rocket and the chance to have a dedicated launch to our exact orbit on our schedule. But their spacecraft experience and payload hosting services have proven to be just as valuable as launch services for our project success.”
Despite being one of the most efficient and energetic propellants for spacecraft, cryogenic propellants can vaporize as temperature rises, causing critical loss on orbit. LOXSAT will test the ability to store liquid oxygen (LOX) in a zero-loss configuration, with the goal of creating a larger scale model in the future that could serve as a commercial cryogenic propellant depot in space. This would enable reuse and refueling of spacecraft on orbit.
The basis of the spacecraft is the Company’s Photon platform, which gained flight heritage in 2022 with NASA’s CAPSTONE mission to the Moon. LOXSAT was designed and built using Rocket Lab’s vertically integrated components and systems, including star trackers, propulsion systems, reaction wheels, solar panels, flight software, radios, composite structures, tanks, separation systems, and more. The spacecraft was produced and will undergo environmental testing at the Company’s Spacecraft Production Complex and headquarters in Long Beach, California, and will ultimately be launched from Rocket Lab Launch Complex 1 in New Zealand.
The LOXSAT mission is sponsored by NASA’s Tipping Point program that aims to advance technologies that could support human space exploration in the future.
###
Rocket Lab Media Contact
Lindsay McLaurin
media@rocketlabusa.com
+ About Rocket Lab
Rocket Lab is a leading space company that provides launch services, spacecraft, payloads, and satellite components serving commercial, government, and national security markets. Rocket Lab’s Electron rocket is the world’s most frequently launched orbital small rocket; its HASTE rocket provides hypersonic test launch capability for the U.S. government and allied nations; and its Neutron launch vehicle in development will unlock medium launch for constellation deployment, national security and exploration missions. Rocket Lab’s spacecraft and satellite components have enabled more than 1,700 missions spanning commercial, defense and national security missions including GPS, constellations, and exploration missions to the Moon, Mars, and Venus. Rocket Lab is a publicly listed company on the Nasdaq stock exchange (RKLB). Learn more at www.rocketlabcorp.com.
+ About Eta Space
Eta Space is a technology development company founded in 2019 by former NASA personnel. Named after the Greek letter η — symbolizing efficiency — Eta Space develops advanced cryogenic systems for space exploration and the future hydrogen energy economy. From the lunar surface to local airports, Eta Space is Fueling Future Exploration with cutting-edge solutions that push the boundaries of efficiency and innovation. Learn more at etaspace.com.
+ Forward Looking Statements
This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. We intend such forward-looking statements to be covered by the safe harbor provisions for forward looking statements contained in Section 27A of the Securities Act of 1933, as amended (the “Securities Act”) and Section 21E of the Securities Exchange Act of 1934, as amended (the “Exchange Act”). All statements contained in this press release other than statements of historical fact, including, without limitation, statements regarding our launch and space systems operations, launch schedule and window, safe and repeatable access to space, Neutron development, operational expansion and business strategy are forward-looking statements. The words “believe,” “may,” “will,” “estimate,” “potential,” “continue,” “anticipate,” “intend,” “expect,” “strategy,” “future,” “could,” “would,” “project,” “plan,” “target,” and similar expressions are intended to identify forward-looking statements, though not all forward-looking statements use these words or expressions. These statements are neither promises nor guarantees, but involve known and unknown risks, uncertainties and other important factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements, including but not limited to the factors, risks and uncertainties included in our Annual Report on Form 10-K for the fiscal year ended December 31, 2024, as such factors may be updated from time to time in our other filings with the Securities and Exchange Commission (the “SEC”), accessible on the SEC’s website at www.sec.gov and the Investor Relations section of our website at www.rocketlabcorp.com, which could cause our actual results to differ materially from those indicated by the forward-looking statements made in this press release. Any such forward-looking statements represent management’s estimates as of the date of this press release. While we may elect to update such forward-looking statements at some point in the future, we disclaim any obligation to do so, even if subsequent events cause our views to change.

When TikTok videos started to go viral on Instagram and Reddit, TikTok turned to professional sound designers to protect their content.
More and more…
This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!

Baker McKenzie advised ResInvest Group on the acquisition of Onyx Power Group from Riverstone Holdings LLC. The closing of the transaction is subject to customary approvals. Onyx Power Group is a European energy supply company and an expert in the safe and weather-independent provision of electricity and heat. Onyx Power Group has six power plants in Germany and the Netherlands with a total net capacity of 1.65 GW. The portfolio includes some of the most modern thermal power plants in Europe, which combine high efficiency with low emissions. The most important locations include Wilhelmshaven, Rotterdam, Zolling and Farge near Bremen.
“With our experienced, international team, we were able to support our client in further expanding its position in the European energy market”, commented Holger Engelkamp, Corporate/M&A Partner in Berlin. “The transaction also gives our client the opportunity to tackle important transformation projects for the German energy market”, adds Dr. Claire Dietz-Polte, energy law partner in Berlin, who led the transaction together with Holger Engelkamp and heads the German energy and infrastructure practice with him.
ResInvest Group is an international trading and investment company that supplies essential commodities for the global markets. The company has extensive experience in the energy sector and in the operation of conventional power plants in Europe. As a strategic investor, ResInvest Group strengthens Onyx Power’s strategy and the upcoming transformation in the context of the energy transition.
The Energy and Infrastructure team, which is part of Baker McKenzie’s corporate/M&A practice, regularly advises on domestic and international transactions. Most recently, the energy and infrastructure team advised the American company Sunoco on the acquisition of the tank terminal operator Tanquid, the Dutch battery storage investor Return on the purchase of four large-scale battery storage sites in Germany from BESSMART, the battery storage developer J+P Batterien on the entry of the Dutch battery storage investor Return and Terra One Climate Solutions on the conclusion of a framework agreement with S4 Energy. Baker McKenzie’s Corporate/M&A practice also advised AURELIUS on the acquisition of Landis+Gyr’s EMEA business; Knorr-Bremse on the acquisition of duagon Group; Cheyne Capital on the refinancing of Kaffee Partner; JD.com on the acquisition of Ceconomy; VINCI Energies on the acquisition of R + S Group and the acquisition of Zimmer & Hälbig Group; Bristol Myers Squibb on the transfer of Juno Therapeutics to TQ Therapeutics; Georg Fischer on the acquisition of VAG Group; AURELIUS on the acquisition of Teijin Automotive Technologies; Centric Software on the acquisition of Contentserv Group; Fagron Group on the acquisition of Euro OTC & Audor Pharma GmbH; Berlin Packaging, a portfolio company of Oak Hill Capital Partners and Canada Pension Plan Investment Board, on the acquisition of RIXIUS AG; and Instalco on the investment in FABRI AG.
Legal adviser to ResInvest:
Baker McKenzie
Lead:
M&A/Energy: Holger Engelkamp (partner, Berlin)
Projects/Energy: Dr. Claire Dietz-Polte (partner, Berlin)
Team:
Corporate/M&A: Ben Boi Beetz (senior associate)
Projects/Energy/Regulatory: Dr. Katharina Weiner (partner, Düsseldorf), Dr. Janet Butler, Dr. Maximilian Voll (both Counsel, Berlin), Nico Ruepp (associate, Berlin), Stefanie Zenzen (associate, Düsseldorf)
Employment / Pensions: Dr. Matthias Köhler (partner, Berlin), Dr. Verena Böhm (counsel, Frankfurt), Isabell Guntermann (associate, Berlin)
Financing: Kathrin Marchant (partner), Esther Kapern (associate, both Frankfurt)
IT/Data Protection: Florian Tannen (partner), Daniel Wulle (senior associate), Clarissa Rach (associate, all Munich), Anela Winzig (associate, Frankfurt)Antitrust/FDI: Dr. Anika Schürmann (partner), Dr. Florian Kotman (counsel, both Düsseldorf), Anahita Thoms (partner), Alexander Ehrle (senior associate, both Berlin)
The Netherlands: Mohammed Almarini (partner), Laila Kouchi (legal director), Anne van den Dorpel (associate), Anna van Bracht (partner), Lois Knijpinga (associate, Amsterdam)
Belgium: Roel Meers (partner), Arnaud Flamand (associate, both Brussels) as well as other lawyers in the Netherlands and Belgium.
About Baker McKenzie
Complex business challenges require an integrated response across different markets, sectors, and areas of law. Baker McKenzie’s client solutions provide seamless advice, underpinned by deep practice and sector expertise, as well as first-rate local market knowledge from more than 70 offices globally. Baker McKenzie works alongside clients to deliver solutions for a connected world.
www.bakermckenzie.com

Artificial intelligence (AI) is increasingly being integrated into health care, offering a wide array of benefits [-]. Current AI applications encompass patients’ diagnosis, treatment, data mining, and more to enhance patient care and quality of life. Recent breakthroughs in AI and machine learning have led to the building of reliable and safe AI systems capable of handling the complexity of health care support in disciplines such as cardiology, radiology and oncology, health information management, patient care, and workforce development. AI fast tracks results in emergency rooms, trauma units, supply chain systems, and radiology and pathology units, for example. The impact is to minimize deficiencies in human resources, provide considerable benefits for patient safety and quality of care, alleviate clinician burnout, and decrease health care costs over time.
These gains offer great transformative potential, enabling acceleration of processes in diverse areas of health care [-]. Furthermore, AI is democratizing access to expert support by providing timely and accurate disease diagnoses, better clinical management, quicker drug discovery, improved disease prevention, big data management, and enhanced health protection [,]. In addition, 23% of health care executives in the United States believe that AI and machine learning are very effective at improving clinical outcomes [].
The potential of AI to optimize resource use and boost productivity underscores its critical role in health care management and patient care. Building on this promising start necessitates striking a balance between technical advancements and management of ethical considerations. Responsible deployment of AI applications by the health care sector can lead to automated services, effective care delivery, and improved patient outcomes. This transformation requires policy support through strong governance, and for ethical concerns and regulatory issues to be addressed.
The current use of AI complements and boosts human resources and has a far-reaching impact in health management, health care worker training, and health services. Its full adoption will enhance leadership and management experiences in the delivery of care while supporting current functions and future innovations in the health care sector [,]. To ensure that health care workers are adequately equipped, skilled, and trained to use AI proficiently in health management and clinical practice, health care managers, educators, and providers must play a more proactive role in the ongoing digital revolution to ensure its effective and regular use [-]. Furthermore, health care leaders should actively promote the translation of innovation and research findings into health care management and delivery practices [,]. This will help revolutionize health care management, improve resource use, advance precision medicine, institutionalize operational efficiency, automate processes, and maximize predictive analytics [].
Understanding AI adoption, progression, characteristics of early adopters, barriers to adoption, the extent to which and why individuals support AI adoption, and the role played by different levels of health management or leadership will inform future AI-related programs and policies. This will enable the global health care sector to adopt new management or leadership styles and organizational structures to harness the potential of AI effectively []. This study aimed to garner viewpoints from across the world on AI adoption in health care, its usefulness in patient care and health management or leadership, and the characteristics of early AI adopters.
We conducted a worldwide cross-sectional survey using a self-administered questionnaire developed with the Qualtrics electronic data collection tool, targeting senior health care professionals for their opinions on the use of AI in the health care sector. The questionnaire included sections on AI adoption, deployment, use, benefits and barriers to AI adoption, as well as basic, anonymized demographic information of the participants (). We piloted and reviewed the questionnaire to ensure completeness, accuracy, acceptability, cultural sensitivity, and relevance. The questionnaire and subsequent data analysis complied with the protocol and checklist outlined in CHERRIES (Checklist for Reporting Results of Internet E-Surveys) [] ().
The study population comprised health care executives, health care leaders, and service providers drawn from the 6 inhabited continents of the world (North and South America, Asia, Africa, Australia or Oceania, and Europe). We used a population prevalence of 23% and a confidence level of 95% to arrive at a sample size of 273 [,].
Health care executives and providers were identified through a convenience sampling technique of professional associations or organizations, social media platforms, and professional networks. The survey was sent to over 500 health care professionals, using their personalized email addresses. We also used professional networks to distribute the questionnaire, and anyone who received the questionnaire link could participate in the study. Participants were informed in the invitation email of the nature of the study, the length of time necessary to complete the questionnaire (less than 10 minutes), and the identity of the principal investigator (OOO). Participants were also informed that fully anonymized information would be collected and stored for 6 months behind a firewall and that no personal, traceable, or identifiable data would be collected. A link was provided in the email to the questionnaire, which required a “1-time only” password to prevent multiple completions of the questionnaire by individual participants.
Participation was voluntary with no incentives offered, and data collection occurred over a 7-week period from October 1 to November 19, 2024. The questionnaire was formatted over 16 pages with 1 to 2 questions per page and hosted on the Qualtrics website for the duration of the study. Participants were able to check for completeness and could review their answers using a “back button.” If participants were unsure or unwilling to disclose their responses, options including “not sure,” “not applicable,” or “prefer not to say” were available. According to the Qualtrics assessment, the study had a 99% completion rate for those persons who received the email, accessed the link, and started to complete the questionnaire.
After closure of the survey, data analysis was performed on anonymized, submitted questionnaires using SPSS (version 27; IBM Corp) and Microsoft Excel. Data were uploaded automatically by Qualtrics, rather than being uploaded manually for analysis. Descriptive and comparative analyses were conducted including frequencies, percentages, and chi-squares. A P value of <.05 was considered significant. To maintain participants’ anonymity, data were aggregated prior to analysis. Results are presented in tables, charts, and as narrative formats for clarity and comprehension.
Ethics approval was received from the California State University, Dominguez Hills Institutional Review Board (IRB) following an IRB approval application (CSUDH IRB-FY2024-66). An information sheet was provided before completion of the questionnaire, informing participants of the survey duration (up to 10 minutes), how the data were to be used, and that participation was optional and asking whether each participant was willing to proceed on that basis. Informed consents were obtained from participants before access to the questionnaire was given. Before completing the study, participants consented to their responses being used in an anonymized, aggregated fashion for medical research purposes and for subsequent secondary data analysis only. Only anonymized data were collected with no traceable information to the individual participants. The data were kept behind an institutional firewall at California State University, Dominguez Hills. Prior parental informed consent was requested in the event that a participant was under the age of consent. However, there was no participant younger than 18 years of age included in the study. No compensation was given for participating in this study.
A total of 506 health care leaders and service providers participated in the survey. Most participants were drawn from Africa, North America, and Europe. The sex distribution was nearly equal, with the male population accounting for 47.8% (181/379) and the female population for 49.1% (186/379) of respondents. The rest were nonbinary or third sex (2/379, 0.5%), others (1/379, 0.3%), and those who preferred not to disclose their sex (9/379, 2.4%). Most participants (265/376, 70.5%) were between the ages of 30 and 59 years. Regarding level of education, 87.3% (331/379) were university graduates, with 71.5% (271/379) holding an advanced degree—a master’s degree (146/379, 38.5%) or a doctorate (125/379, 33%)—as their highest qualification.
In terms of professional experience, respondents were evenly distributed, with similar proportions having less than 10 years and 25 years or more. Approximately half (195/377, 51.7%) were affiliated with federal, state, or college or university systems, and 44.7% (226/506) worked in the health care services, while 28.3% (143/506) were affiliated with the educational sector. Over half (200/373, 53.6%) of the respondents were identified as Black or African American people. Geographically, the majority were based in Africa (159/373, 42.6%), North America (130/373, 34.9%), or Europe (49/373, 13.1%), as outlined in . Black or African American constituted the largest population of respondents (200/373, 53.6%), followed by White (55/373, 14.7%).
To the question “Do you think AI has any role or usefulness in health care practice and management?” 92.3% (467/506) responded Yes. Of these, 58.7% (254/433) were of the view that AI is very (179/433, 41.3%) or extremely (75/433, 17.3%) important. In the near future, 79.8% (375/470) were of the view that AI will be very (199/470, 42.3%) or extremely (176/470, 37.4%) useful ().
A total of 95.6% (173/181) of male participants, 91.9% (171/186) of female participants, 95.6% (154/159) of those from Africa, 93.9% (46/49) of those from Europe, 87.7% (114/130) of those from North America, 95.5% (191/200) of those who identified as Black or African American, 92.7% (51/55) of White, and 86.7% (26/30) of Hispanic or Latino participants stated that AI was useful for health management and patient care. There was a significant difference in the responses of male participants versus female participants (P<.001), organizational affiliations (P=.01), and continent of residence or operation (P=.03; -). Similarly, 87.8% (173/181) of male, 75.3% (140/186) of female, African (147/159, 92.5%), Black or African American (178/200, 89%), European (38/49, 77.6%), Hispanic or Latino (19/30, 63.3%), North American (87/130, 66.9%), and White (40/55, 72.7%) participants were of the view that AI is very or extremely useful in health; however, only sex (P=.01) and the continent of residence or operation (P=.001) showed a significant difference.
| Description | Values, n (%) | |
| Sexat birth (n=379) | ||
| Male | 181 (47.8) | |
| Female | 186 (49.1) | |
| Nonbinary or third sex | 2 (0.5) | |
| Others | 1 (0.3) | |
| Prefer not to say | 9 (2.4) | |
| Age in completed years (n=376) | ||
| <20 | 4 (1.1) | |
| 20-29 | 45 (12) | |
| 30-39 | 89 (23.7) | |
| 40-49 | 104 (27.7) | |
| 50-59 | 72 (19.1) | |
| >60 | 62 (16.5) | |
| Highest educational qualification (n=379) | ||
| High school diploma or General Educational Development | 26 (6.9) | |
| Bachelors | 60 (15.8) | |
| Masters | 146 (38.5) | |
| Doctorate | 125 (33) | |
| Other | 17 (4.5) | |
| Prefer not to specify | 5 (1.3) | |
| Length of experience in health care (years; n=372) | ||
| <5 | 85 (22.8) | |
| 5-9 | 54 (14.5) | |
| 10-14 | 61 (16.4) | |
| 15-19 | 40 (10.8) | |
| 20-24 | 50 (13.4) | |
| >25 | 82 (22) | |
| Affiliation (n=377) | ||
| Federal or state government facility or institution | 100 (26.5) | |
| County or local government facility or institution | 24 (6.4) | |
| College or university | 95 (25.2) | |
| Nonprofit or public charity | 56 (14.9) | |
| Private facility or institution | 67 (17.8) | |
| Other | 35 (9.3) | |
| Professional track (select all that apply)a (n=506) | ||
| Health care services | 226 (44.7) | |
| Health education | 143 (28.3) | |
| Health informatics | 45 (8.9) | |
| Health technology | 32 (6.3) | |
| Health administration or management | 120 (23.7) | |
| Other | 67 (13.2) | |
| Race or ethnicity (n=373) | ||
| Arab or Middle-Eastern | 6 (1.6) | |
| Asian (East and South) | 25 (6.7) | |
| Black or African American | 200 (53.6) | |
| Hispanic or Latino or Latinx | 30 (8) | |
| Native American or Alaskan Native | 3 (0.8) | |
| Pacific Islander or Hawaiian | 1 (0.3) | |
| White | 55 (14.7) | |
| Mixed | 17 (4.6) | |
| Other | 19 (5.1) | |
| Prefer not to say | 17 (4.6) | |
| Location or residence (n=373) | ||
| Africa | 159 (42.6) | |
| Europe | 49 (13.1) | |
| Asia | 19 (5.1) | |
| North America | 130 (34.9) | |
| South America | 8 (2.1) | |
| Australia or Oceania | 8 (2.1) | |
aParticipants were able to select multiple options.
| Description | Yes, n (%) | ||
| Do you think AI has any role or usefulness in health care practice and management? (n=506) | |||
| Yes | 467 (92.3) | ||
| No | 13 (2.6) | ||
| Neither | 26 (5.1) | ||
| If yes, how useful do you think AI is now in health care management and practice? (n=433) | |||
| Not useful | 9 (2.1) | ||
| Slightly useful | 61 (14.1) | ||
| Moderately useful | 109 (25.2) | ||
| Very useful | 179 (41.3) | ||
| Extremely useful | 75 (17.3) | ||
| In the future, how useful do you think AI will be in health care management and practice? (n=470) | |||
| Not useful | 4 (0.9) | ||
| Slightly useful | 20 (4.3) | ||
| Moderately useful | 71 (15.1) | ||
| Very useful | 199 (42.3) | ||
| Extremely useful | 176 (37.4) | ||
| Have you had any formal exposure or training in AI? (n=470) | |||
| Yes | 142 (30.2) | ||
| No | 302 (64.3) | ||
| Not sure | 26 (5.5) | ||
| If yes, what kind of training or exposure did you have? (Select all that apply)a (n=142) | |||
| Basic orientation | 89 (62.7) | ||
| Training in AI use in patient care (diagnosis, treatment, laboratory services, etc) | 24 (16.9) | ||
| Training in AI use in management and leadership | 43 (30.3) | ||
| Training in technical aspects of AI | 43 (30.3) | ||
| Other forms of AI training | 33 (23.2) | ||
| Has your institution or organization adopted or begun the process of AI adoption, adaptation, and use? (n=457) | |||
| Yes, we have adopted AI | 60 (13.1) | ||
| Yes, we will adopt AI | 36 (7.9) | ||
| Yes, we are beginning to think about adopting AI | 107 (23.4) | ||
| No, we have not started adopting AI | 180 (39.4) | ||
| Do not know | 74 (16.2) | ||
| Has your organization trained anyone on AI use? (n=445) | |||
| Yes | 93 (20.9) | ||
| No | 197 (44.3) | ||
| Do not know or not sure | 155 (34.8) | ||
| If staff have been trained, who benefited from the training? (n=210) | |||
| Executive leadership or top level | 33 (15.7) | ||
| Management staff or mid-level | 47 (22.4) | ||
| Operational staff | 58 (27.6) | ||
| IT staff | 44 (21) | ||
| Other | 24 (11.4) | ||
| Prefer not to say | 4 (1.9) | ||
aParticipants were able to select multiple options.
| Description | Race or ethnicity | Chi-square (df) | P value | ||||
| Black or African American (200/373, 53.6%); yes, n (%) | White (55/373, 14.7%); yes, n (%) | Hispanic or Latinx (30/373, 8%); yes, n (%) | |||||
| AI has a role in health care practice and management | 191 (95.5) | 51 (92.7) | 26 (86.7) | 21.8 (20) | .35 | ||
| AI will be very to extremely useful in health care management and practice | 178 (89) | 40 (72.7) | 19 (63.3) | 52.3 (40) | .09 | ||
| Have had formal exposure or training in AI | 69 (34.5) | 15 (27.3) | 6 (20) | 37.6 (20) | .01 | ||
| The organization has adopted AI | 17 (8.5) | 12 (21.8) | 4 (13.3) | 40.6 (40) | .45 | ||
| The organization has trained someone on AI use | 32 (16) | 14 (25.5) | 4 (13.3) | 13.3 (20) | .87 | ||
| The participant will support AI adoption and embedding | 168 (84) | 39 (70.9) | 17 (56.7) | 35.5 (20) | .01 | ||
| Description | Continent | Chi-square (df) | P value | ||||
| Africa (159/373, 42.6%); yes, n (%) | Europe (49/373, 13.1%); yes, n (%) | North America (130/373, 34.9%); yes, n (%) | |||||
| AI has a role in health care practice and management | 154 (96.9) | 46 (93.9) | 114 (87.7) | 20.1 (10) | .03 | ||
| AI will be very to extremely useful in health care management and practice | 147 (92.5) | 38 (77.6) | 87 (66.9) | 44.5 (20) | .001 | ||
| Have had formal exposure or training in AI | 46 (28.9) | 15 (30.6) | 43 (33.1) | 13.4 (10) | .20 | ||
| The organization has adopted AI | 12 (7.5) | 12 (24.5) | 21 (16.2) | 41.6 (20) | .003 | ||
| The organization has trained someone on AI use | 21 (13.2) | 12 (24.5) | 30 (23.1) | 27.8 (10) | .002 | ||
| The participant will support AI adoption and embedding | 145 (91.2) | 41 (83.7) | 76 (58.5) | 53.6 (10) | <.001 | ||
| Description | Sex | Chi-square (df) | P value | ||||
| Male (181/379, 47.8%); yes, n (%) | Female (186/379, 49.1%); yes, n (%) | Other (12/379, 3.2%); yes, n (%) | |||||
| AI has a role in health care practice and management | 173 (95.6) | 171 (91.9) | 7 (58.3) | 36.4 (8) | <.001 | ||
| AI will be very to extremely useful in health care management and practice | 159 (87.8) | 140 (75.3) | 4 (33.3) | 31.7 (16) | .01 | ||
| Have had formal exposure or training in AI | 55 (30.4) | 56 (30.1) | 3 (25) | 3.0 (8) | .94 | ||
| The organization has adopted AI | 24 (13.3) | 22 (11.8) | 3 (25) | 26.1 (16) | .05 | ||
| The organization has trained someone on AI use | 38 (21) | 31 (16.7) | 3 (25) | 9.0 (8) | .34 | ||
| The participant will support AI adoption and embedding | 163 (90.1) | 123 (66.1) | 4 (33.3) | 71.3 (8) | <.001 | ||
| Description | Sex at birth | Age | Education | Experience | Affiliation | Race or ethnicity | Continent | ||||||||||||
| Chi-square (df) | P value | Chi-square (df) | P value | Chi-square (df) | P value | Chi-square (df) | P value | Chi-square (df) | P value | Chi-square (df) | P value | Chi-square (df) | P value | ||||||
| AIa has a role in health care practice and management | 36.4 (8) | <.001 | 12.1 (10) | .28 | 3.2 (10) | .98 | 14.4 (10) | .16 | 22.5 (10) | .01 | 21.8 (20) | .35 | 20.1 (10) | .03 | |||||
| AI will be very to extremely useful in health care management and practice | 31.7 (16) | .01 | 24.9 (20) | .21 | 28.7 (20) | .09 | 18.1 (20) | .58 | 30.6 (20) | .06 | 52.3 (40) | .09 | 44.5 (20) | .001 | |||||
| Have had formal exposure or training in AI | 3.0 (8) | .94 | 30.4 (10) | <.001 | 19.8 (10) | .03 | 43.0 (10) | <.001 | 11.0 (10) | .36 | 37.6 (20) | .01 | 13.4 (10) | .20 | |||||
| The institution has adopted AI | 26.1 (16) | .05 | 35.7 (20) | .01 | 61.4 (20) | <.001 | 28.1 (20) | .11 | 41.8 (20) | <.001 | 40.6 (40) | .45 | 41.6 (20) | .003 | |||||
| The organization has trained someone in AI use | 9.0 (8) | .34 | 11.9 (10) | .29 | 29.7 (10) | <.001 | 29.1 (10) | .001 | 43.1 (10) | <.001 | 13.3 (20) | .87 | 27.8 (10) | .002 | |||||
| The participant will support AI adoption and embedding | 71.3 (8) | <.001 | 52.2 (10) | <.001 | 22.1 (10) | .01 | 27.4 (10) | .002 | 16.1 (10) | .20 | 35.5 (20) | .02 | 53.6 (10) | <.001 | |||||
aAI: artificial intelligence.
On training and exposure to AI, the study revealed that 30.2% (142/470) of the respondents have had formal exposure or training to AI, the majority (89/142, 62.7%) had a basic orientation, 13.1% (60/457) of institutions or organizations have adopted AI in any form, and 20.9% (93/445) have trained management, operational, and IT staff on AI use. Approximately equal percentages of male (55/181, 30.4%) and female (56/186, 30.1%) participants have been exposed to AI technology. However, more people were exposed to AI in North America (43/130, 33.1%) and Europe (15/49, 30.6%) than in Africa (46/159, 28.9%), but this difference was not statistically significant (P=.20). In addition, more Black or African American (69/200, 34.5%) and White (15/55, 27.3%) participants were exposed to AI than Hispanic or Latino (6/30, 20%) participants, and this was statistically significant (P=.01). Furthermore, more male participants reported that their organizations had trained people in AI (38/181, 21% vs31/186, 16.7%), but this difference was not significant (P=.03). European (12/49, 24.5%) and North American (30/130, 23.1%) participants reported more training than African participants (21/159, 13.2%), and this difference was statistically significant (P=.002). However, reported training across racial or ethnic groups was not statistically significant (P=.87).
Among all respondents, 76.5% (300/392) will support AI adoption and embedding in their organization. AI adoption is led mainly by top executive leadership. However, other levels of leadership play significant roles, as shown in .
A total of 38.6% (102/264) of respondents did not know who was or is leading the artificial intelligence adoption process in their organization. More organizations with male respondents have adopted AI (24/181, 13.3% vs 22/186, 11.8%), female respondents (P=.05). Of note, 24.5% (12/49) of European, 16.2% (21/130) of North American, but only 7.5% (12/159) of African organizations have adopted AI (P=.003; and ). The continent of residence or operation had the highest levels of significance in all parameters except formal exposure to AI (α=.20; ).
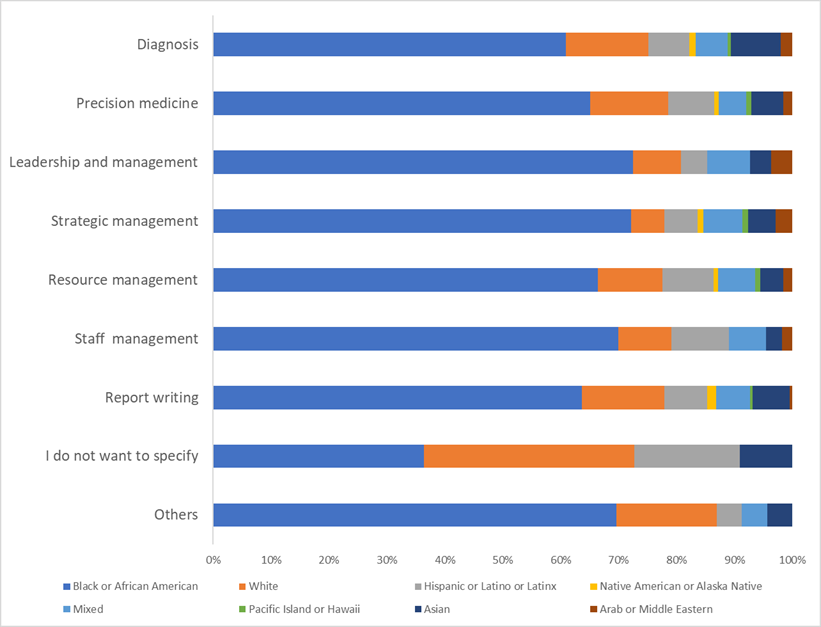
AI is used mostly in diagnosis (247/506, 48.8%), report writing (230/506, 45.5%), and patient care (205/506, 40.5%). Other areas of high use are in precision medicine (160/506, 31.6%), resource management (156/506, 30.8%), staff management, and leadership and management (137/506, 27.1% each; ).
Similarly, in the coming years, it was predicted that AI will still be most relevant in diagnosis (120/407, 29.5%), patient care (75/407, 18.4%), precision medicine (65/407, 16%), and report writing (58/407, 14.3%). Respondents also identified other uses of AI. These include (among several others) marketing, counseling, emergency preparedness and response, customer services, real-time data management, drug discovery and development, modeling and predictive analytics, a tool for triage at the first point of contact, accurate billing and fraud detection, across-board process sequencing, advancing science and policy, monitoring air quality within the health care system, data management (eg, data access, analysis, processing, and report development), assessment (preanalytical, analytical, and postanalytical stages in health care), research (such as cancer research and treatment), environmental sanitation (such as cleaning toilets and emptying bedpans), customer services (such as customer complaints and solutions and generating referral codes), supply chain management, outreach programs, disease surveillance (including mapping, prediction, and preventive medical interventions), documentation, health care education (including staff training), communication and information management (including referrals, collaboration, and electronic health records), report writing (including minutes of meetings), insurance discoveries, data to inform decisions in most domains, health care advocacy, streamlining and standardizing systems (including processes, charting, referrals, and billing), schedule management (for employees and clients), claims and billing, disease surveillance and epidemic early warning, strategy development and leadership and management in global health, staff management (including hiring, training, and evaluation), prediction and management of pandemics and other emergency situations, procurement and purchasing tenders, strategic management, surveys, and community outreach.
AI use in patient care also includes deployment in surgeries (including robotic surgical equipment), preventive health care, patient follow-up or tracking, virtual health, remote patient monitoring, clinical decision support, patient engagement, detecting adverse events in inpatient and outpatient care, care coordination, chart making, blood and blood products delivery in rural and underserved communities, fast diagnosis and prompt treatment including gene therapy and infection control measures, patient reminders to adhere to their medication and appointment schedules, registration and recording, and prescription management.
In this regard, some respondents commented, “Virtually all aspects with no exception,” “Every aspect including management,” “Every aspect of health care,” “Everywhere,” “In all areas of health care,” and “In all areas of health care delivery and improvement.”
Knowledge of AI (121/402, 30.1%), fear of job loss (64/402, 15.9%), and staff resistance to change (39/402, 9.7%) were the top barriers identified by respondents against AI adoption (). Other barriers are the cost of acquisition and inadequate staff skills ().
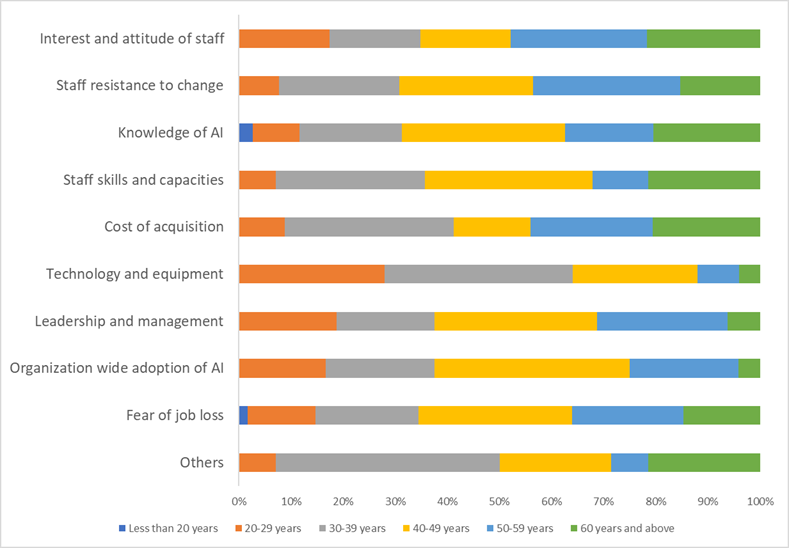
Apart from the itemized barriers, respondents further identified other barriers including poor access to relevant training, hallucination and possible AI inaccuracy, unreliable results, annoying responses in patient care or calls, clinical errors, confidentiality issues, inequitable, patient preference (such as patients not wanting computers or “bots” to talk to them), quality and trustworthiness of AI, grant writing, validity of results, and religious beliefs. Some respondents said, “All options are important barriers.”
Although three-quarters of people were ready to support AI adoption (300/392, 76.5%), 23.5% (92/392) will either not support AI adoption (13/392, 3.3%) or not be sure (79/392, 20.2%). Participants who were unwilling to support AI adoption listed security reasons, lack of in-depth understanding of how AI works, privacy issues, cost, fear of job loss, inaccuracy of results, uncarted future, fear of change, lack of human emotions with AI, fear of AI displacing humanity in patient care, distrust of AI, ignorance of AI and use in health care, patient safety, inferiority to human care, privacy risks, and cost of adoption among all others as their top reasons. A respondent said, “Until it becomes enforced, there will be no need for it.”
The adoption, promotion, impact, and deployment of AI in health leadership and management are a multifaceted process that encompasses various dimensions of health care delivery. The results presented here demonstrate the high importance of AI across all segments, but the adoption of AI and training of workers in AI is low and should be improved upon. A significant proportion of respondents were of the view that AI is already very useful in health care management and patient care and that its value will increase in the future.
Among our survey respondents, exposure to or training in AI was very low (142/470, 30.2%), the majority of which has been basic orientation (89/142, 62.7%). This indicates a serious gap in AI-related professional development that needs to be filled. Given this finding, it is not surprising that participants highlighted the knowledge (and, where relevant, skills) gap as the top barrier to adoption of AI. It is axiomatic, therefore, that if the health care sector wants to improve AI adoption, health care workers and managers must be trained in AI use to a level appropriate for their role.
Similarly, only 13.1% (60/457) of all institutions participating in this survey have adopted AI to date, while 7.9% (36/457) are considering its implementation soon. However, a further 23.4% (107/457) disclosed that they are starting to think about adopting AI. This is not unexpected, as AI is still new, and many people (including some participants) are unaware of its usefulness, skeptical of its precision, and uninformed about its range of applications. Adoption is also low due to key barriers such as fear of job loss, staff resistance to change, and cost, perceived or real, of adoption.
Herein, 20.9% (93/445) of respondents said that their organization had trained someone in the use of AI. This 1 in 5 participation rate compares to the 11.4% reported in a recently published survey on AI chatbot use by medical researchers published in 2024 []. The almost doubling may be due to a combination of many factors, among others including the time difference—a year between the 2 studies, greater awareness, increased adoption, and a reflection that chatbots capture only a small proportion of AI uses in health care. Moreover, in the 2024 study, 69.7% of surveyed individuals expressed interest in further training, whereas 79.5% of participants in our survey would support AI adoption in their organization [].
The drive to adopt AI in the health care sector is primarily led by top leadership and management, followed by technical staff. Very few participating organizations (8/264, 3%) outsourced this process. Therefore, promoting AI technologies was influenced by both top-down and bottom-up approaches. However, more than 38% (102/264) of respondents did not know who was leading the AI movement in their organization. Such a lack of awareness calls for better communication between managers and operational or field staff. If not addressed, it may result in change implementation failure, as it is widely recognized that poor communication is the most common cause of change failure in change implementation [].
The integration of AI technologies in health care has the potential to transform health systems, improve patient outcomes, and enhance operational efficiencies [-]. Our study confirms previous reports, showing that AI is useful across several domains of health management and patient care. These include diagnosis and patient care, data management and review, staff and resource management, research and pipeline analysis, and report writing, a portfolio that is predicted to expand in the coming years. AI was most relevant to in-patient care, diagnosis, precision medicine, and report writing, corroborating previous findings [,].
Among our survey respondents, more Black or African American (drawn from Africa, Europe, and North America) respondents were trained or exposed to AI (69/200, 34.5%) compared to White (15/55, 27.3%) and Hispanic or Latino (6/30, 20%) respondents, and this difference is significant (P=.01). However, geographically, fewer participants from Africa (46/159, 28.9%) have had formal training or exposure to AI compared to participants from Europe and North America; fewer organizations in Africa (12/159, 13.2%) have trained their staff in AI compared to organizations in North America (30/130, 23.1%) and Europe (12/49, 24.5%). Furthermore, AI adoption is lowest in Africa (12/159, 7.5%) but highest in Europe (12/49, 24%). This finding is not surprising, as historically, Africa has faced challenges in adopting new technologies due to infrastructure deficits, unhealthy policies, government instabilities, limited access to technology and education, and economic constraints [-]. Efforts must be made this early to ensure that African health care is not left behind in this AI revolution. In light of traditional development barriers, this may appear an aspirational goal. However, our data show a positive mindset toward embracing AI technology in health care, suggesting that it can be readily implemented. This is because Africa has a higher proportion of participants who believe in the usefulness of AI in health management and patient care currently (154/159, 96.9%) and in the future (147/159, 92.5%) and who are willing to support AI adoption (145/159, 91.2%) when compared to Europe (46/49, 93.9%; 38/49, 77.6%; and 41/49, 83.7%; respectively) and North America (114/130, 87.7%; 87/130, 66.9%; and 76/130, 58.5%; respectively). While further studies are needed to identify why AI adoption support is so low in North America, efforts should be made across all continents to enhance and accelerate AI adoption and to boost uptake and the quality and quantity of staff training programs.
Fewer female participants who completed the survey consider that AI has a role to play in health care management and patient practices (171/186, 91.9%) as against male participants (173/181, 95.6%). Moreover, a significantly lower proportion of female participants are willing to support AI adoption (123/186, 66.1%) compared to male participants (163/181, 90.1%; P<.005). We plan to conduct a qualitative study to determine the root cause of this difference. In the meantime, priority should be given to improve female participants’ awareness of the existence of AI and its usefulness, primarily by raising exposure rates of female participants to AI in schools, universities, hospitals, clinics, and community health facilities. We should also involve female participants in simulation exercises involving AI to improve their AI savvy and use. These practices may improve their acceptance and readiness to support AI adoption in health care management and patient care.
Key barriers to AI adoption as identified by our survey respondents are poor knowledge of AI (121/402, 30.1%), people’s fear of job loss (64/402, 15.9%), and staff resistance to change. Other leading barriers were the cost of acquisition and inadequate staff skills. Similar factor that hinders AI adoption were identified in previous studies [-]. When poor knowledge of AI and inadequate staff skills are combined, we have a disproportionately high ignorance-mediated barrier. All top barriers apart from the cost of acquisition are human resource–mediated, showing that appropriate communication, tailored training, and on-the-job exposure to AI can significantly reduce them. These barriers can further be reduced or removed through adequate explanation to patients and their families to gain social acceptance and build trust of AI technologies. Staff education and improved health literacy will most likely increase the willingness of health care workers to support AI adoption, acquisition, and installation.
This study achieved a notably high completion and participation rate compared with similar surveys, which often report substantially lower levels of engagement. This outcome was not unexpected, as we strategically leveraged the extensive professional and community networks of our research partners located in Africa (n=3), North America (n=3), South America (n=1), and Europe (n=2). In addition, the authors maximized their personal and professional connections to enhance outreach, while multiple reminders to the target population further improved response rates.
A particularly striking finding was that Black or African American participants demonstrated both a higher response rate and a more positive attitude toward AI adoption and use. Whether this reflects genuine readiness or aspirational enthusiasm remains an open question that warrants further investigation. Although several African nations, notably Rwanda, Nigeria, and Ghana [-], have demonstrated notable leadership in AI adoption relative to their regional peers, additional qualitative inquiry is needed to better contextualize and interpret this finding.
Taken together, the results underscore the importance of conducting more detailed qualitative studies to explore the underlying drivers of the variations observed in this research. A deeper, country-level analysis of AI adoption processes, rates, and patterns of use will provide a richer and more nuanced understanding of the current global landscape of AI adoption.
This study is subject to the typical limitations of a cross-sectional online survey, including selection bias, as participation was limited to individuals within the authors’ personal and professional networks. Additionally, the authors are unaware of the total number of individuals who received the questionnaire, making it impossible to calculate an accurate response rate. Furthermore, some email systems may block messages from unknown senders or redirect them to spam or junk folders, which could have further reduced participation.
To mitigate these limitations in future research, a more purposeful study design should be used—one in which participants are deliberately selected and actively encouraged to respond, thereby improving the likelihood of obtaining unbiased and representative results.
Health care workers are aware of the AI revolution and recognize its usefulness in health care management and patient care. However, their knowledge, support, and adoption are each still low. Hence, there is a need to train more health care workers on not just the basic concepts of AI, but on AI use, algorithms, coding, and other technical issues. Universities, colleges, and institutions of higher education have a critical role in AI training and should be equipped and empowered to do this. In addition, a significant percentage of respondents were ignorant of those who were leading the AI adoption process—a pointer to communication failure or breakdown. Therefore, executive health care management should communicate better with their team to prevent innovation adoption failures. To effectively navigate the path forward toward realizing the potential of GenAI in health care, we recommend training health care leaders and workers in various aspects of AI management and use, provision of AI resources and infrastructure, and standardized oversight and guidelines []. This will play a significant role in building the health infrastructures required to achieve the United Nations Sustainable Development Goal 3 of “good health and well-being” [].
In addition, we suggest that organizations and health care managers in Africa should deliberately and proactively invest in AI adoption and staff training, in order not to be left behind. Having health care workers who are favorable to AI adoption is a strength that African leaders can exploit right now. Individuals should be made to understand that AI works best when guided by skilled personnel and thus will not be replacing people. Although some jobs may be lost, AI will create new jobs and further opportunities that will balance the scale. To advance AI adoption, embedding, and use, governments should emulate Vietnamese leadership that has “identified AI as a key technology to boost its economy” and is taking deliberate and proactive steps to build partnerships, train engineers, pilot new products, support startups, and create an enabling environment for AI development to thrive [,]. As opined by one of the subject matter experts, “… successful AI implementation requires a combination of technical expertise, financial sustainability, and socio-political commitment. Each of these factors is crucial to fostering an environment conducive to AI adoption. All of these criteria are now met (in the private sector), but this cannot be said of the public system that is antiquated and overstretched by comparison” []. Yet, unlike the Vietnamese government, training in AI should go beyond engineers who develop the tools to include health care providers who adopt and use the tools to manage and care for patients. Funding public health institutions to adopt and embed AI will go beyond paying for the acquisition of AI and training of appropriate health care workers to expanding institutional infrastructure and mitigating staff resistance to change powered by fear of job loss and inadequate knowledge of AI functionalities and benefits.
In addition, various ethical concerns around data ownership, privacy, and use and the overall governance of AI need to be addressed by developing, adopting, and implementing organization-wide AI policies. As the said author also said, “data privacy, and the overall governance of AI technologies in healthcare, … are critical for building public trust and ensuring the safe deployment of AI systems.” To achieve a seamless adoption of AI across the global health system, health care workers must be permitted unhindered oversight to alleviate inherent fear that may otherwise result in overt and covert resistance, which will thereby foster acceptance among patients [].
Finally, to effectively navigate the path forward toward realizing the potential of GenAI in health care, we recommend training health care leaders and workers in various aspects of AI management and use, provision of AI resources and infrastructure, and standardized oversight and guidelines []. This will play a significant role in building the health infrastructures required to achieve the United Nations Sustainable Development Goal 3 of “good health and well-being” [].
This study reveals that AI adoption is a global phenomenon, with uptake increasing in all continents, including low- and middle-income countries. Our study documents the present adoption rates and some perceived factors that are facilitating or hindering AI adoption. In addition, health care workers believe that AI is useful and will be more relevant in the future. However, despite several advances in AI technology, deployment and adoption are still lower in some regions of the world. A significant number of participants are ready to support AI adoption and embedding in their organization, as they believe that AI will be very to extremely useful in health care management and practice.
The authors are grateful to the following individuals for useful discussion or feedback during preparation of this manuscript: Professor Anupama Joshi and Ms Judith Aguirre of California State University, Dominguez Hills; Professor Elaine Holmes of Murdoch University, Perth, Western Australia; Professor Paiboon Sithithaworn of Khon Kaen University, Khon Kaen, Thailand; Professor Cathryn Edwards of the University of Lincoln Medical School, Lincoln, United Kingdom; and Professor Marsha Y Morgan of University College London, London, United Kingdom. OOO was supported by California State University, Dominguez Hills and Centre for Family Health Initiative for institutional funding support. SDT-R was supported by the Wellcome Trust Institutional Strategic Support Fund awarded to Imperial College London.
Data are available on request from the author (OOO).
OOO, SDT-R, and AWT-R conceived the paper and designed the methodology used. All authors distributed questionnaires, collated and interpreted data, and contributed significantly to writing the manuscript. SDT-R, OOO, and AWT-R revised it critically for important intellectual content. All authors approved the final version and agreed to its submission. All authors agree to be accountable for the content of the work. The authors confirm that this paper does not need institutional approval to be published.
None declared.
Edited by A Coristine; submitted 02.Jan.2025; peer-reviewed by JCL Chow, A Hidki; comments to author 14.Apr.2025; revised version received 15.Jul.2025; accepted 28.Sep.2025; published 22.Oct.2025.
©Obinna O Oleribe, Andrew W Taylor-Robinson, Vetty R Agala, Olajide O Sobande, Ricardo Izurieta, Simon D Taylor-Robinson. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 22.Oct.2025.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research (ISSN 1438-8871), is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.