The Suns and Cavs will square off on New Year’s Day as part of an NBA TV triple-header.
• Download the NBA App
• Amex 2025-26 Season Preview
NEW YORK — The National Basketball Association (NBA) today announced a new multi-platform…

The Suns and Cavs will square off on New Year’s Day as part of an NBA TV triple-header.
• Download the NBA App
• Amex 2025-26 Season Preview
NEW YORK — The National Basketball Association (NBA) today announced a new multi-platform…
A total of six Salmonella strains were isolated from green onion, peach leaves, peach orchard soil, and cow manure collected in Daegu and Gyeonsangbuk-do provinces, South Korea. Each sample (25 g) was pre-enriched in 225 mL of tryptic soy broth…
Terms
While we only use edited and approved content for Azthena
answers, it may on occasions provide incorrect responses.
Please confirm any data provided with the related suppliers or
…

Revered filmmaker Mira Nair will present Rohan Parashuram Kanawade’s “Cactus Pears” (Sabar Bonda) for its North American release, with support from Payal Kapadia, whose “All We Imagine as Light” earned international acclaim last…

MINNEAPOLIS, Oct. 13, 2025 /PRNewswire/ — BAE Systems (LON: BA) and the U.S. Army Combat Capabilities Development Command Armaments Center (DEVCOM AC) successfully tested the Scorpio-XR artillery projectile from a 155mm…

This year’s overarching theme for MIPCOM‘s Women In Global Entertainment Power Lunch? Resilience.
Some of television’s most senior industry execs flocked to Cannes’ Hotel Majestic on Monday as MIPCOM formally kicks off another…
This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!
After gaining informed consent, the university hospital used aseptic surgery to remove the umbilical cord tissue from a healthy donor. Before dissecting Wharton jelly (WJ), UC tissue was submerged in phosphate-buffered saline (PBS) containing 100 U/ml penicillin, 100 µg/ml streptomycin, and 2 µg/ml amphotericin B [21]. WJ was centrifuged at 340xg after being treated for an hour at 37 °C with collagenase (1 mg/ml type I) and hyaluronidase (0.7 mg/ml). The cell pellet was mixed with DMEM/F12 supplemented with 15% FBS and incubated at 37 °C with 5% CO2. Fresh media was added to the cells every 4 days throughout the 21-day observation period [22]. WJ-MSC cells’ morphology was examined under a microscope. During the culture period, the medium was replaced every 3–4 days to ensure proper cell growth. Cells were split at a 1:4 ratio upon reaching confluence to maintain adequate growth conditions and prevent overcrowding. In WJ-MSC cells during the 21st-day passage, flow cytometric examination revealed the presence of CD14, CD34, CD73, and CD105 labeling. WJ-MSC cell surface receptors CD14, CD34, CD73, and CD105 staining were subjected to the immunofluorescence technique [23].
For 48 h, MSC cells were cultured in 75 cm2 flasks using DMEM/F12 mix that was devoid of FBS (starved). Exosomes secreted from fasting cells during a 48-h period were first obtained by collecting the media. To separate the cells and big vesicles, the fluids were centrifuged for 10 min at 13,000×g and 10 min at 45,000×g. After that, it was centrifuged in an ultracentrifuge for 5 h at 110,000×g (Beckman Coulter) [24]. Ultimately, the pellet was suspended in PBS and the supernatant was discarded [25]. Using flow cytometry, the characteristics of the isolated exosomes were examined for the CD9, CD63, CD81, and HSP70 markers. WJMSC exosomes were incubated with 1.5 × 105 anti-CD63 beads in 50 ml PBS at room temperature for 15 min to perform a flow cytometric analysis. The beads were incubated for the entire night at 4uC with mild stirring after the volume was increased to 300 ml. After 30 min of incubation in 100 mM glycine, the process was halted [26]. Following two rounds of washing, exosome-coated beads were incubated in 50 mg of human IgG (Sigma-Aldrich) for 15 min at 4 °C. They were then treated with anti-CD9 FITC, anti-CD63 PE, anti-CD81 APC, or matched isotype controls (BD Biosciences) and obtained using a FACS Melody (BD Biosciences) [27]. TEM electron microscopy was used to determine the morphology and nano-size of WJMSCs exosomes [28]. The isolation and characterization process were repeated three times to confirm reproducibility and consistency in results.
To assess the effectiveness and safety of WJ-MSC-derived exosome gel in patients with diabetic foot ulcers (DFUs), a randomized double-blind controlled clinical experiment was carried out. The trial protocol was implemented after obtaining the Scientific Research Ethics Committee of Kafr Elsheikh University on 25/3/2024, with final approval by the Committee’s decision No. KESIRB200-175. With Clinical Trial ID. NCT06812637 on ClinicalTrials.gov https://clinicaltrials.gov/study/NCT06812637. All participants provided written informed consent before enrollment.
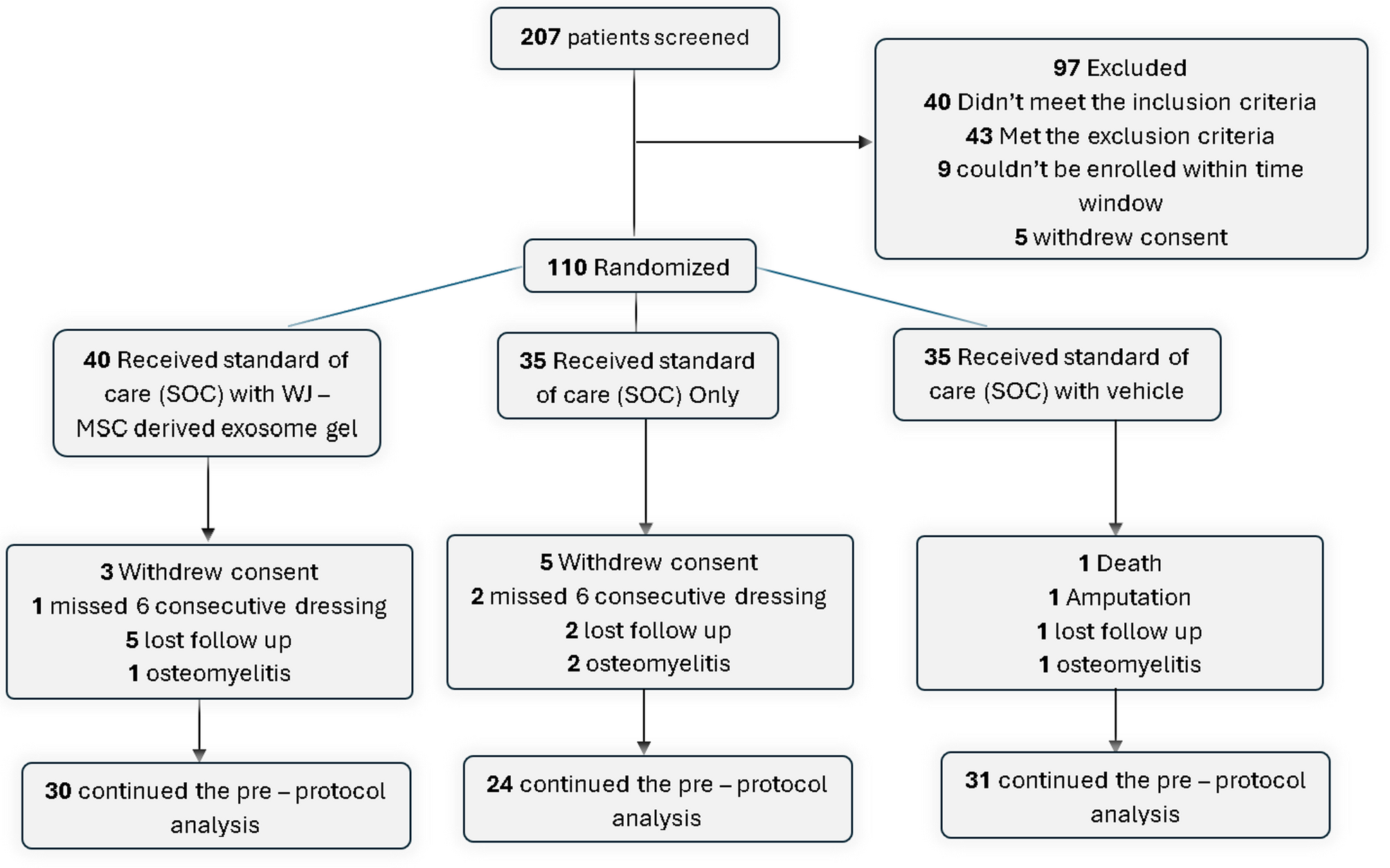
After 207 patients were assessed, 110 of them satisfied the requirements for inclusion. The patients were then split into three groups:
Group treated: 40 patients received standard of care (SOC) once weekly for 4 weeks, followed by a 16-week follow-up, using Wharton jelly derived mesenchymal stem cell (WJ-MSC) exosome gel [29].
Control group: 35 patients had just standard of care (SOC) for 4 weeks, then 16 weeks of follow-up.
A visually similar saline-based formulation was administered once weekly to 35 patients in the placebo group for 4 weeks, followed by follow-up for 16 weeks, along with SOC [29].
Analysis After Dropouts:
Group treated (SOC + WJ-MSC-derived exosome gel):
30 patients completed the pre-protocol analysis.
Dropouts included: 3 withdrew consent, 1 missed 6 consecutive dressings, 5 were lost to follow-up, and 1 developed osteomyelitis.
Control Group (SOC only):
24 patients completed the pre-protocol analysis.
Dropouts included: 5 withdrew consent, 2 missed 6 consecutive dressings, 2 were lost to follow-up, and 2 developed osteomyelitis.
Placebo Group (SOC with vehicle):
31 patients completed the pre-protocol analysis.
Dropouts included: 1 death, 1 amputation,1 was lost to follow-up, and 1 developed osteomyelitis.
A consort flow diagram showing the progress through the trial phases is shown in Fig. 1.
Consort flow diagram showing the progress through the phases of the trial
People with type 2 diabetes who are 42–62 years of age.
The existence of a persistent DFU that does not go away after 7 days of standard of care (SOC) treatment or that does not shrink by more than 30%.
Ulcers smaller than 30 cm² that are seen on the plantar, medial, or lateral portions of the foot.
Individuals suffering from ischemic, neuropathic, or mixed neuropathic-ischemic ulcers.
Revascularization performed for ischemic ulcers before enrollment.
Pregnancy or breastfeeding.
Type 1 diabetes who are 18 years of age or older.
Presence of venous ulcers or active infections.
Exposure of bone, ligaments, or tendons.
Demographic data, comorbidities, and concomitant medications were recorded. All participants received instructions on ulcer care and offloading.
Two systems were used for classification: the Wound, Ischemia, and Foot Infection system (WIFI system) and the Site, Ischemia, Neuropathy, Bacterial Infection, Area, Depth system (SINBAD system) [30].
The SINBAD method makes it easier to classify diabetic foot ulcers (DFUs) using a 0–1 point scale. The severity of the ulcer is indicated by a score that ranges from 0 to 6 [31]. This approach is easy to use, gives good intra-observer and modest inter-observer repeatability, and doesn’t require any specific equipment beyond standard clinical examination. The SINBAD system is a useful tool for clinical application, as recommended by the IWGDF, and it efficiently monitors ulcer progression, healing, and amputation risk Table 1.
The WIFI system, developed by the Society for Vascular Surgery in 2014, addresses the limitations of existing classifications by evaluating three major risk factors for amputation: wound characteristics, ischemia (based on ABI scores), and infection. Each factor is scored from 0 to 3, providing a detailed severity assessment as shown in Table 2. While the WIFI system aids in predicting major amputations and guiding interventions like revascularization, its reliance on specialized vascular measurements limits its utility in primary or community care settings, making it more suitable for specialized vascular clinics.
The categorization method is used to determine whether a diabetic has a foot infection and how serious it is, as shown in Table 3.
The presence of clinically significant foot ischemia makes both diagnosis and treatment of infection considerably more difficult.
Infection refers to any part of the foot.
In any direction, from the rim of the wound.
If osteomyelitis is demonstrated in the absence of ≥ 2 signs/symptoms of local or systemic inflammation, classify the foot as either grade 3(O) (if < 2 SIRS criteria) or grade 4(O) if ≥ 2 SIRS criteria).
An Android smartphone was used to measure the ulcer’s length, breadth, and surface area exactly [33]. The camera was positioned 25 cm from the ulcer, making sure it was parallel to the wound. After taking the picture, the operator marked the edges of the wound and determined the size of the ulcer. A blinded medical practitioner assessed each wound three times to ensure reproducibility, and statistical analysis was performed using the average of these data [29]. Ulcer size reduction will be computed using the following formula: ulcer size reduction = (Ai – Af)/Ai × 100, where Ai is the initial ulcer area and Af is the ulcer area during follow-up after treatment. Ulcers were assessed and photographed for healing [34].
Debridement of diabetic foot ulcers was initially performed to remove hyperkeratotic skin or necrotic and infected tissues. Following that, the area was cleaned with regular saline. Before beginning any research, measurements were made of the ulcer’s length, width, and surface. After applying the Wharton jelly derived mesenchymal stem cell (WJ-MSC) exosome gel to the ulcer, the treatment group covered the region with sterile gauze and a non-compressible bandage. After a month of doing every 3 days, the wound was irrigated with regular saline, examined for infection, and then treated with Wharton jelly derived mesenchymal stem cell (WJ-MSC) exosome gel. The SOC was administered to the control and placebo groups, which included removing necrotic, hyperkeratotic, and infected tissues, washing the wound with regular saline, and covering the ulcer with non-compressible bandages and sterile gauze. The patients were instructed to change the bandages every day and wipe the ulcer with regular saline [29].
Participants were followed up for 16 weeks with evaluations conducted at 2, 4 weeks, then 6 weeks, and then at 2, 4, and 6 months [29]. At each visit:
Ulcers were cleansed and assessed for infection.
A record of the interim medical history was kept, which included adverse events and prescription drugs.
Photographs of the ulcers were taken at each time point.
Primary Endpoint:
Secondary Endpoints:
The average reduction in ulcer size throughout the research.
Complete healing rate (100% re-epithelialization without drainage).
Safety assessment, including adverse events and tolerability [29].
The study utilized clinical classification systems, including the SINBAD and WIFI systems, to stratify ulcers by severity, vascular health, and infection risk. Evaluating an ulcer involves several diagnostic tools to uncover underlying complications. To provide a comprehensive picture of systemic health and inflammation, laboratory tests usually include fasting blood sugar levels, glycated hemoglobin (HbA1c), a full metabolic panel, complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP).
Imaging studies play a critical role, with plain X-rays used to identify hidden issues such as osteomyelitis, subcutaneous air, fractures, or foreign bodies. When osteomyelitis is suspected, MRI stands out as the preferred diagnostic tool due to its superior accuracy. Peripheral vascular disease can be assessed using arterial Doppler and ankle-brachial index (ABI) measurements, ensuring vascular factors are addressed. The probe-to-bone (PTB) test provides a straightforward but efficient way to identify osteomyelitis at the patient’s bedside: if a sterile metal probe contacts bone while exploring the ulcer, the test is positive. When treating diabetic individuals who may have bone infections, this rapid and accurate test is quite helpful [35].
To get rid of necrotic or diseased tissues, wounds were debrided.
After cleaning the region with regular saline, the therapy was administered.
The ulcers were covered with non-compressive bandages and sterile gauze.
Participants were instructed to clean and redress ulcers daily.
The non-parametric Wilcoxon rank-sum test was used to evaluate differences in continuous variables of interest, while the chi-square test (or Fisher’s exact, if more applicable) was employed to compare categorical variables between groups. The Wilcoxon signed-rank test was used for post hoc comparisons to find changes in ulcer area across the timepoints of interest, and the non-parametric Friedman test was used to find differences in ulcer size at baseline, 2 weeks, and 4 weeks for the effects of therapy. Software GraphPad Prism (GraphPad version 8.0.2) was used to conduct statistical analysis. When P was less than 0.05, statistical significance was reached.
