
Introduction
Background
Adolescent mental health is a cornerstone of national well-being and a pivotal focus of China’s “Healthy China” initiative. This commitment is demonstrated by consecutive national policies explicitly targeting the enhancement of mental health literacy (MHL). Key actions include the “Healthy China Action (2019-2030),” which sets specific literacy targets, and the “Action Plan for Children and Adolescent Mental Health (2019-2022),” which aimed to boost mental health knowledge among youths [,]. This policy momentum has been sustained through recent strategic outlines, underscoring the ongoing priority of safeguarding adolescent psychological well-being [,].
Against this policy backdrop, a pressing public health challenge has emerged. National data indicate that 14.8% of adolescents in China face depression risk, with 40% frequently experiencing loneliness [,]. This psychological vulnerability coexists with a near-saturated digital environment, characterized by 96.8% internet penetration among minors []. Within this context, a pronounced reliance on digital technology is evident, as over one-third of adolescents exhibit psychological dependence on smartphones. Moreover, prolonged social media use is linked to a significantly increased risk of anxiety and depression []. This combination of factors means today’s teenagers, who are “digital natives,” face 2 major risks: heightened psychological distress and problematic social media use. Therefore, improving health literacy—particularly in the digital mental health domain (mental eHealth literacy [MeHL])—and mitigating social media addiction (SMA) has emerged as a critical public health imperative.
Enhancing health literacy is widely established as a cornerstone strategy for public health improvement [,]. Yet, adolescents often exhibit insufficient health literacy, which manifests as help-seeking dilemmas (eg, “not recognizing illness” or “recognizing but not seeking treatment”) that hinder access to care []. This is particularly critical for senior high school students, whose developing literacy can shape lifelong health trajectories. In theory, health literacy is thought not only to directly affect health but also to work by influencing other factors (as a mediator) or by changing the strength of a relationship (as a moderator) [-].
However, research has seldom examined the distinct and potentially synergistic roles of its multidimensional facets in the digital context. Specifically, a significant gap remains in understanding the interplay between MHL—focused on psychological cognition, eHealth literacy (eHL)—centered on digital competency, and their integration as MeHL in relation to adolescent SMA and depression-anxiety-stress (DASS). To address this gap, this study aims to investigate the multifaceted effects and underlying mechanisms of this multidimensional health literacy framework, thereby informing targeted mental health interventions.
Theory and Research Hypotheses
Health Literacy, SMA, and DASS
Health literacy, initially proposed by Simonds in 1974, emphasizes improving public health decision-making skills through education []. Later, Nutbeam [] further expanded the concept, proposing a 3-level model of functional, interactive, and critical health literacy, focusing on individuals’ ability to acquire health information while emphasizing the ability to assess information and implement health decisions. The World Health Organization defines health literacy as “the ability to access, understand, evaluate, and apply health information and services to promote and maintain good health” []. In the “Healthy China Action (2019-2030)” [], health literacy is viewed as the ability to acquire, process, and understand health-related information, which is essential for maintaining or improving health and quality of life, and is a critical means for improving health outcomes and promoting healthy behaviors. Thus, health literacy is not limited to the acquisition of health knowledge but emphasizes the promotion of overall health through effective health decision-making and behavior change.
As an important branch of health literacy, mental health literacy was first introduced by Jorm et al [], focusing initially on individuals’ ability to recognize, understand, and address mental health issues, while emphasizing the reduction of stigma and the enhancement of help-seeking willingness []. As research deepened, the scope expanded to include multiple dimensions such as recognizing mental health problems, understanding causes, and coping strategies []. The core feature of MHL focuses on psychological content, emphasizing cognitive processing and attitude transformation toward mental states.
With the widespread penetration of digital technologies, eHL and MeHL have emerged. The former, defined by Norman and Skinner [], emphasizes the ability to search, evaluate, and apply broad health information through electronic media, highlighting the operational characteristics of media approaches. The latter, as an emerging concept, is defined as “the knowledge, beliefs, and skills to manage mental health through digital tools” [], which represents an intersection of MHL and eHL within a specific technological context. It is a dual-core integration dimension of “media × psychology.” Although these 3 aspects fall under the health literacy system, they are interconnected but not hierarchically subordinate, and should be understood as parallel and intersecting multidimensional variables []. In conclusion, health literacy is a multidimensional, systematic concept that encompasses the acquisition, understanding, judgment, and application of health knowledge and services. It is a learned psychological tendency that is highly interventionable and modifiable [].
In the current educational context, stress has become a significant psychosocial factor affecting adolescents, with anxiety and depression being the most common mental health disorders []. According to data from the China Youth Research Center [], the detection rate of anxiety among primary and secondary school students is 31.3%, with a depression risk rate of 17.9%. Additionally, 57.4% of high school students report high levels of academic pressure. Many adolescents delay or are unwilling to seek psychological support due to the stigmatization of mental health issues, lack of knowledge about mental health assistance, and insufficient external support [], reflecting a deficiency in MHL. Adolescent mental health is directly influenced by MHL. Good MHL not only helps to recognize mental disorders [] but also increases help-seeking willingness and coping ability [], alleviates negative emotions, and reduces the risk of depression and anxiety [,], with a particularly significant improvement observed in adolescents with mild to moderate depression.
eHL, which is the ability to obtain and apply online health information, is also crucial for adolescent mental health. Lower levels of eHL lead to difficulties in understanding information, which in turn affects health management behaviors. Higher levels of eHL are linked to adolescents’ ability to acquire effective health resources, higher psychological well-being, and better self-regulation abilities []. Furthermore, eHL is negatively correlated with anxiety and depression [], playing a positive role in relieving psychological stress, enhancing social support, and improving emotional adaptability [,].
SMA, as a typical behavioral addiction of the digital age, is characterized by maladaptive dependence on social media platforms and a loss of self-regulation []. A representative survey of nearly 6000 adolescents revealed that 4.5% of them are at risk for SMA [], with prevalence rates generally higher than those in university students and community adults []. Existing research primarily explains the mechanisms of SMA from the perspectives of personality traits (eg, emotional stability) and negative emotions (eg, depression and anxiety) [], with limited attention given to the role of health literacy.
Social cognitive theory (SCT) suggests that the interaction between individuals, behaviors, and environments shapes behavioral patterns, and adolescents’ social media use is influenced not only by the media environment but also by their level of health literacy []. Research has found that higher MHL is significantly associated with a lower likelihood of SMA and can effectively intervene in maladaptive usage behaviors []. eHL has also been shown to be strongly negatively correlated with internet addiction []. Adolescents with lower health literacy are more likely to develop internet dependence, using the internet to distract themselves, escape reality, or regulate negative emotions such as loneliness, anxiety, and depression []. The information overload and social pressure in the online environment further amplify their negative emotional experiences, particularly in groups with insufficient eHL, which increases the likelihood of feelings of anxiety, isolation, and self-denial [].
It is crucial to distinguish between the core constructs of “digital literacy” (eg, eHL) and the contextual challenge of “information overload.” Digital literacy refers to an individual’s subjective capability to process digital health information, acting as a protective factor. In contrast, information overload represents an objective environmental stressor or risk factor. The core logic of our framework is to investigate how high levels of digital literacy enable adolescents to effectively navigate and mitigate risks within an information-overloaded environment. Additionally, adolescents who use social media for more than 2 hours a day often experience increased DASS and suicidal ideation, highlighting the real threat of addictive behaviors. The higher the level of eHL, the more effectively individuals can use digital resources to regulate emotions and improve behavioral health, demonstrating lower addiction tendencies and higher psychological resilience.
The Impact of Health Literacy on SMA and DASS
MeHL is a composite literacy formed by integrating the core elements of MHL and eHL in the context of digital media. It emphasizes an individual’s ability to acquire, understand, assess, and apply mental health information using digital tools []. Compared to MHL, which focuses on the recognition and management of mental health problems, and eHL, which emphasizes the acquisition and assessment of digital health information, MeHL involves both cognitive processing of psychological content and the technical processing of media information, forming an integrated, rather than subordinate, independent dimension [].
As an important intermediary pathway through which education levels influence health status, lower MeHL is significantly associated with an increased risk of mental health disorders []. Individuals with higher levels of eHL and MHL are better equipped to use digital platforms to access psychological support and intervention resources. This results in stronger MeHL, which enables them to more effectively identify and address psychological risks, thus reducing maladaptive and addictive behaviors associated with social media use []. Some studies also suggest that digital literacy is negatively correlated with behavioral addiction, meaning that the higher the digital skills, the better adolescents can avoid excessive social media use [].
Further research has found that both MHL and eHL have a significant positive effect on predicting health behaviors, and that MHL can play a key moderating role in the process by which eHL influences health behaviors, with its moderating effect reaching 31.1% []. Individuals with higher levels of eHL possess the ability to filter information and operate media tools, but without the cognitive support of MHL, they may find it difficult to convert information into effective behavioral intentions. On the other hand, individuals with higher MHL are more likely to proactively identify, understand, and integrate health information in complex digital environments, thereby enhancing their behavioral execution and psychological regulation []. This mechanism aligns with the behavioral-driving logic of “perceived benefits” and “self-efficacy” in the health belief model (HBM) [] and is consistent with the “individual-behavior-environment” triadic interaction pathway proposed by SCT [].
This Study
Existing research primarily focuses on the independent roles of eHL and MHL, lacking a comprehensive examination of their interactive effects, particularly in the context of SMA. While MeHL is an emerging concept, its role and interactions within the digital environment remain underexplored. To address these gaps through an integrated theoretical lens, this study synthesizes conservation of resources (COR) theory, HBM, and SCT. These theories offer complementary explanations: COR theory provides the motivational foundation by framing health literacy as a key personal resource; HBM elucidates the cognitive decision-making process; and SCT offers the overarching behavioral framework of triadic reciprocity. Guided by this framework, we construct a comprehensive model () to elucidate the joint influence pathways of eHL, MHL, and MeHL on adolescent SMA and DASS. The following hypotheses are proposed:
H1: eHL and MHL have a significant negative effect on adolescent SMA and DASS.
H2: MeHL mediates the effect of eHL and MHL on adolescent SMA and DASS.
H3: MHL significantly moderates the effect of eHL on MeHL and, through a dual moderation mediation pathway, influences SMA and DASS.
Methods
Study Design
This study used a cross-sectional design with a stratified cluster random sampling method to examine the relationships between adolescents’ multidimensional health literacy and their engagement with SMA, as well as symptoms of depression, anxiety, and stress. The study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement [].
Setting
This cross-sectional study was conducted in 5 provinces of China (Beijing, Zhejiang, Shanxi, Henan, and Jiangsu), selected to represent a range of regional digitalization levels. Data collection was carried out in the computer labs or classrooms of the participating schools over a 3-month period, from February to April 2025.
Participants
The sampling procedure was conducted in 3 stages: first, 5 provinces were selected as strata based on regional digitalization indices; second, 2 general high schools were randomly selected within each province; and finally, 2 intact classes were randomly chosen from each school, resulting in a total of 20 classes. The target population comprised adolescents attending school, with exclusion criteria including severe physical or mental disabilities, inability to independently complete the questionnaire, or ongoing related treatment. A total of 855 adolescents completed valid questionnaires (response rate 85.5%), with 449 (52.5%) males, 406 (47.5%) females, and a mean age of 16.38 (SD 0.86) years.
Variables
This study examined the following variable classes, all derived from self-report questionnaires:
- Outcome variables: SMA and a composite score of DASS served as the primary outcomes.
- Exposure variables: eHL and MHL were the core independent variables.
- Mediating variable: MeHL was tested as the mediator in the hypothesized pathways.
- Effect modifier: MHL was additionally examined as a moderator of the relationship between eHL and MeHL.
- Covariates: Participant age and gender were included as control variables in all multivariable analyses.
Measurement
eHealth Literacy Scale
The eHealth Literacy Scale (eHEALS) developed by Norman and Skinner [] was used. This scale contains 8 items and covers 3 dimensions: the ability to acquire, evaluate, and apply health information online. It assesses adolescents’ knowledge, comfort, and self-perceived ability to acquire, understand, assess, and apply electronic health information. The scale uses a 5-point Likert scale, with responses ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). The total score ranges from 8 to 40, with higher scores indicating higher levels of eHL. In this study, the scale demonstrated excellent internal consistency, with both a Cronbach α of 0.944 and a McDonald ω of 0.959 for the total score. The consistency estimates for the 3 dimensions were also high: application ability (α=0.907; ω=0.948), evaluation ability (α=0.883; ω=0.934), and decision-making ability (α=0.809; ω=0.922).
Mental Health Literacy Scale
MHL was assessed using a 12-item short form adapted for this study from the original scale by O’Connor and Casey []. To ensure brevity, we selected items that best represented the 4 theoretical dimensions: problem recognition, willingness to seek help, knowledge understanding, and attitudes toward professional help. The measure uses a 5-point Likert scale (“1=strongly disagree” to “5=strongly agree”), and a sum score is calculated (range 12-60), with higher scores reflecting higher MHL. The validity and reliability of this adapted form were supported empirically in our sample: its structural validity was upheld by confirmatory factor analysis (CFA). It demonstrated high internal consistency, with a Cronbach α of 0.946 and a McDonald ω of 0.964 for the total score. The coefficients for the 4 dimensions were problem recognition (α=0.885; ω=0.942), help-seeking (α=0.838; ω=0.919), knowledge understanding (α=0.867; ω=0.941), and attitude (α=0.901; ω=0.949).
Mental eHealth Literacy Scale
The Mental eHealth Literacy Scale (MeHLS) developed by Richard [] was used. This scale consists of 23 items, divided into 3 dimensions: cognitive (8 items), knowledge (7 items), and skills (8 items), to assess an individual’s knowledge, beliefs, and online information processing abilities in managing mental health. The scale uses a 5-point Likert scale (“1=never” to “5=always”), with a total score range of 23 to 115. Higher scores indicate higher levels of digital MHL. In this study, the internal consistency was excellent, with a Cronbach α of 0.953 and a McDonald ω of 0.960 for the total scale. The values for the 3 dimensions were cognitive (α=0.933; ω=0.949), knowledge (α=0.929; ω=0.943), and skills (α=0.937; ω=0.948).
Social Media Addiction Scale
The Bergen Social Media Addiction Scale (BSMAS), developed by Banyai [], was used for assessment. This scale consists of 6 items reflecting 6 typical addiction characteristics: salience, emotional regulation, tolerance, withdrawal symptoms, conflict, and relapse [,]. In line with its widespread application and robust psychometric validation across different cultures and adolescent samples, the BSMAS is consistently treated as a unidimensional scale, and the sum of all items is used to indicate the severity of SMA tendencies [-]. It is used to identify adolescents’ problematic social media use behaviors. The scale uses a 5-point Likert scale (“1=never” to “5=always”), with a total score range of 6 to 30. Higher scores indicate stronger tendencies toward SMA. In this study, the internal consistency for the scale was good, as indicated by both Cronbach α (0.894) and McDonald ω (0.928).
Depression-Anxiety-Stress Scale
The Depression Anxiety Stress Scale-21 (DASS-21), developed by Lovibond in 1995 and later revised and optimized by Antony, was used. This scale contains 21 items divided into 3 subscales—depression, anxiety, and stress—to assess the severity of emotional symptoms over the past week. The scale uses a 4-point Likert scale (“0=never” to “3=always”), with higher scores on each subscale indicating more severe symptoms. For the purpose of this study, a composite psychological distress total score was computed by summing the scores from the three DASS-21 subscales (depression, anxiety, and stress). For the primary analyses (including correlation and mediation analysis), a composite “psychological distress” total score was computed by summing the scores of the 3 subscales. The scale demonstrated excellent reliability in our sample. The internal consistency estimates for the subscales were as follows: depression (Cronbach α=0.909; McDonald ω=0.946), anxiety (α=0.898; ω=0.939), and stress (α=0.914; ω=0.947). The psychological distress total score also showed excellent internal consistency (α=0.959; ω=0.963).
The scales used in this study were all based on mature tools developed both domestically and internationally, or were revised and localized based on previous research. They are grounded in clear theoretical frameworks, scientifically structured designs, and supported by solid practical applications. The full survey questionnaire is available in . To assess the construct validity of the scales, CFA was conducted to evaluate the goodness-of-fit of each measurement model.
The results showed that all models met the evaluation criteria: the χ2/df ratio was within a reasonable range, and the robust comparative fit indices (comparative fit index, Tucker-Lewis index, and incremental fit index) consistently exceeded the recommended threshold of 0.90, with most surpassing 0.95. While the goodness-of-fit index and adjusted goodness-of-fit index for the more complex DASS-21 model were slightly below 0.90—a common occurrence for multidimensional scales—the collective evidence strongly supports model fit. The root-mean-square error of approximation was less than 0.05, and the factor loadings were all at moderate to high levels, indicating that the scales have good construct validity. In conclusion, the measurement tools used in this study meet psychometric standards in terms of reliability and validity, ensuring high measurement quality and providing a solid quantitative foundation for subsequent empirical analyses.
Bias
To address potential sources of bias, several strategies were implemented, with a specific focus on common method bias given the exclusive reliance on self-reported data. Procedural remedies during the research design and data collection phases included anonymous completion, randomization of questionnaire items, and the use of scales with varied response formats to mitigate the influence of potential source bias at the outset. Statistically, Harman single-factor test was planned and used to empirically evaluate the presence of common method bias [].
Study Size
The study size was determined by both feasibility and statistical considerations. Given the constraints of the stratified cluster sampling design, we aimed to recruit a feasible sample from the accessible schools in 5 provinces. The final analytic sample consisted of 855 adolescents. To confirm the adequacy of this achieved sample, a post hoc power analysis was conducted using G*Power 3.1. For a linear multiple regression with 8 predictors, an alpha of 0.05, and a medium effect size (f2=0.15), our sample provided over 95% power, substantially exceeding the minimum requirement of 160 participants, ensuring sufficient power to detect medium and small effect sizes.
Statistical Methods
Data analysis was performed using IBM SPSS 20.0 for tests of common method bias, descriptive statistics, and correlation analysis; IBM Amos 24.0 for CFA and structural equation modeling (SEM); and SPSS PROCESS v4.1 macro for testing mediation and moderation effects. To account for the nonindependence of observations arising from the clustered sampling design, all primary analyses (including SEM and moderated mediation) were conducted using cluster-robust SEs with the classroom as the cluster unit. This method provides corrected SEs and CIs, mitigating the risk of type I error.
A total of 1000 questionnaires were distributed, with 893 returned, resulting in a response rate of 89.3%. The 107 nonreturned questionnaires were primarily attributed to student absences or leave during the survey period. The 893 returned questionnaires were screened for validity and missing data through a 2-stage process. First, to handle missing data, incomplete questionnaires (n=28) with any missing items were excluded. The extent of missing data was minimal, with item-level missingness ranging from 0.2% to 0.5% across all study variables. Little’s test for missing completely at random (MCAR) was nonsignificant (χ285=98.76, P=.15). Given that the data met the MCAR assumption and the fraction of incomplete cases was very small, the use of complete-case analysis was considered methodologically appropriate for this step [].
Subsequently, a second stage of screening for data quality was performed on the remaining complete cases, leading to the exclusion of an additional 10 questionnaires due to abnormal completion times (n=7) or patterned responses (n=3) []. Following this rigorous process, 855 valid and complete questionnaires were retained for all subsequent analyses, representing 95.7% of returned surveys.
Ethical Considerations
This study was conducted in strict accordance with ethical principles for research involving human participants. The study protocol was reviewed and approved by the Academic Ethics Committee of Capital University of Physical Education and Sports (approval no. 2025A0105). Prior to data collection, written informed consent was obtained from all participating adolescents and their parents or legal guardians. The consent process was conducted through the schools. Specifically, information sheets and consent forms detailing the study’s purpose, procedures, potential risks and benefits, and the right to withdraw at any time without penalty were distributed to parents via students. After parental consent was secured, the same documents were presented to the adolescents in an age-appropriate manner to seek their assent.
All data were collected and processed anonymously, with no personally identifiable information stored, to ensure participant privacy and confidentiality. Data were used solely for the purposes of this academic research. Participants did not receive any monetary or material compensation for their involvement in the study. Finally, this manuscript does not contain any images that could lead to the identification of an individual participant.
Results
Common Method Bias Test
The results of the Harman single-factor test were examined to assess the threat of common method bias. The unrotated exploratory factor analysis revealed 8 factors with eigenvalues greater than 1. The first factor accounted for 31.07% of the total variance, which is significantly below the critical threshold of 40%. This indicates that no single factor explained the majority of the variance, suggesting that common method bias is not a severe issue in this dataset and does not pose a substantial threat to the interpretation of the study’s findings. Furthermore, the CFA demonstrated good psychometric properties for all measurement scales, confirming their construct validity ().
| Measurement scales | χ2/df | GFIa | AGFIb | RMSEAc | SRMRd | NFIe | IFIf | CFIg | TLIh | Factor loadings range |
| eHEALSi | 1.768 | 0.996 | 0.981 | 0.030 | 0.032 | 0.998 | 0.999 | 0.999 | 0.996 | 0.753-0.928 |
| MHLS-SFj | 2.711 | 0.982 | 0.958 | 0.045 | 0.042 | 0.989 | 0.993 | 0.993 | 0.986 | 0.753-0.887 |
| MeHLSk | 2.943 | 0.942 | 0.922 | 0.048 | 0.045 | 0.965 | 0.977 | 0.977 | 0.971 | 0.711-0.883 |
| BSMASl | 2.972 | 0.998 | 0.976 | 0.048 | 0.047 | 0.998 | 0.999 | 0.999 | 0.999 | 0.536-0.894 |
| DASSm | 2.774 | 0.809 | 0.792 | 0.046 | 0.052 | 0.883 | 0.922 | 0.922 | 0.917 | 0.628-0.840 |
aGFI: goodness-of-fit index.
bAGFI: adjusted goodness-of-fit index.
cRMSEA: root-mean-square error of approximation.
dSRMR: standardized root-mean-square residual.
eNFI: normed fit index.
fIFI: incremental fit index.
gCFI: comparative fit index.
hTLI: Tucker-Lewis index.
ieHEALS: eHealth Literacy Scale.
jMHLS-SF: Mental Health Literacy Scale – Short Form.
kMeHLS: Mental eHealth Literacy Scale.
lBSMAS: Bergen Social Media Addiction Scale.
mDASS: Depression-Anxiety-Stress Scale.
Intraclass Correlation and Clustering Effects
Prior to testing our hypotheses, we quantified the clustering effect by calculating the intraclass correlation coefficient (ICC) for our primary outcome variables. The analysis revealed that 8.5% of the total variance in SMA (ICC=0.085, 95% CI 0.043-0.150) and 6.2% of the variance in DASS (ICC=0.062, 95% CI 0.028-0.125) resided between classrooms, justifying the need to account for the clustered data structure. All subsequent analyses used cluster-robust SEs to ensure valid statistical inference.
Descriptive Statistics and Pearson Correlation Analysis
Descriptive statistics and correlation coefficients for each variable are presented in . The results revealed significant positive correlations between eHL, MHL, and MeHL. Specifically, eHL showed a moderate to strong positive correlation with both MHL and MeHL. MHL and MeHL also demonstrated a significant positive correlation. Furthermore, all 3 health literacy variables were significantly negatively correlated with SMA and DASS, with these relationships being statistically significant. This suggests that individuals with higher health literacy levels tend to experience lower levels of SMA and psychological distress related to DASS. Gender was significantly correlated with some variables, while age showed relatively weaker correlations. Therefore, gender and age were included as control variables in subsequent analyses to enhance the accuracy and robustness of the results.
| Variable | Mean (SD) | Gender | Age | eHLb | MHLc | MeHLd | SMAe | DASSf |
| Gender | 1.47 (0.500) | 1 | ||||||
| Age | 16.38 (0.865) | –0.062 (–0.130 to 0.007) | 1 | |||||
| eHL | 26.63 (7.928) | 0.029 (–0.039 to 0.096) | 0.042 (–0.023 to 0.109) | 1 | ||||
| MHL | 46.74 (10.184) | 0.089g (0.024 to 0.155) | –0.020 (–0.085 to 0.045) | 0.547g (0.495 to 0.596) | 1 | |||
| MeHL | 70.25 (17.457) | 0.030 (–0.035 to 0.096) | 0.081h (0.010 to 0.153) | 0.695g (0.659 to 0.729) | 0.579g (0.528 to 0.623) | 1 | ||
| SMA | 15.72 (6.026) | –0.015 (–0.082 to 0.052) | –0.022 (–0.045 to 0.087) | –0.369g (–0.432 to –0.303) | –0.400g (–0.462 to –0.335) | –0.370g (–0.430 to –0.309) | 1 | |
| DASS | 39.59 (14.649) | –0.031 (–0.096 to 0.036) | –0.009 (–0.073 to 0.056) | –0.433g (–0.491 to –0.373) | –0.658g (–0.706 to –0.604) | –0.444g (–0.502 to –0.381) | 0.536g (0.479 to 0.591) | 1 |
aGender was dummy-coded, with 1 representing male and 2 representing female. The 95% CIs for the Pearson correlation coefficients, shown in parentheses, were derived from 5000 bootstrap samples. The correlation coefficients in the table are based on 2-tailed tests; the Pearson correlation coefficients are presented below the diagonal.
beHL: eHealth literacy.
cMHL: mental health literacy.
dMeHL: mental eHealth literacy.
eSMA: social media addiction.
fDASS: depression-anxiety-stress.
gP<.01.
hP<.05.
Mediation Effect Test
To further explore the mechanisms of the associations between eHL, MHL, and SMA among high school students and to examine the potential mediating effect of MeHL, the study constructed an SEM path analysis. The chi-square statistic was significant (χ22276=6102.464, P<.001); thus, the normed chi-square (χ2/df) was consulted []. The fit indices of the revised model indicated an acceptable to good fit with the data: χ2/df (2.681), root-mean-square error of approximation (0.044), standardized root-mean-square residual (0.048), normed fit index (0.895), incremental fit index (0.931), comparative fit index (0.931), Tucker-Lewis index (0.927), and coefficient of determination (0.85) []. Although the goodness-of-fit index (0.814) and the adjusted goodness-of-fit index (0.797) were slightly below the commonly used threshold (0.90), the model still demonstrated good fit based on the other major fit indices, supporting further analysis of the relationships between the variables [,].
As shown in and , both eHL and MHL were significantly and positively associated with MeHL (β=0.531, 95% CI 0.468-0.594, P<.001; β=0.356, 95% CI 0.297-0.415, P<.001). Both were significantly negatively associated with SMA (β=–0.152, 95% CI –0.242 to –0.062, P=.01; β=–0.261, 95% CI –0.345 to –0.177, P<.001). However, eHL did not have a significant effect on DASS (β=–0.011, 95% CI –0.060 to 0.038; P=.81), while MHL was a significant negative predictor of DASS (β=–0.590, 95% CI –0.647 to –0.533; P<.001). Additionally, MeHL was also a significant negative predictor of SMA and psychological distress (β=–0.150, 95% CI –0.277 to –0.023, P=.02; β=–0.139, 95% CI –0.207 to –0.071, P=.006).
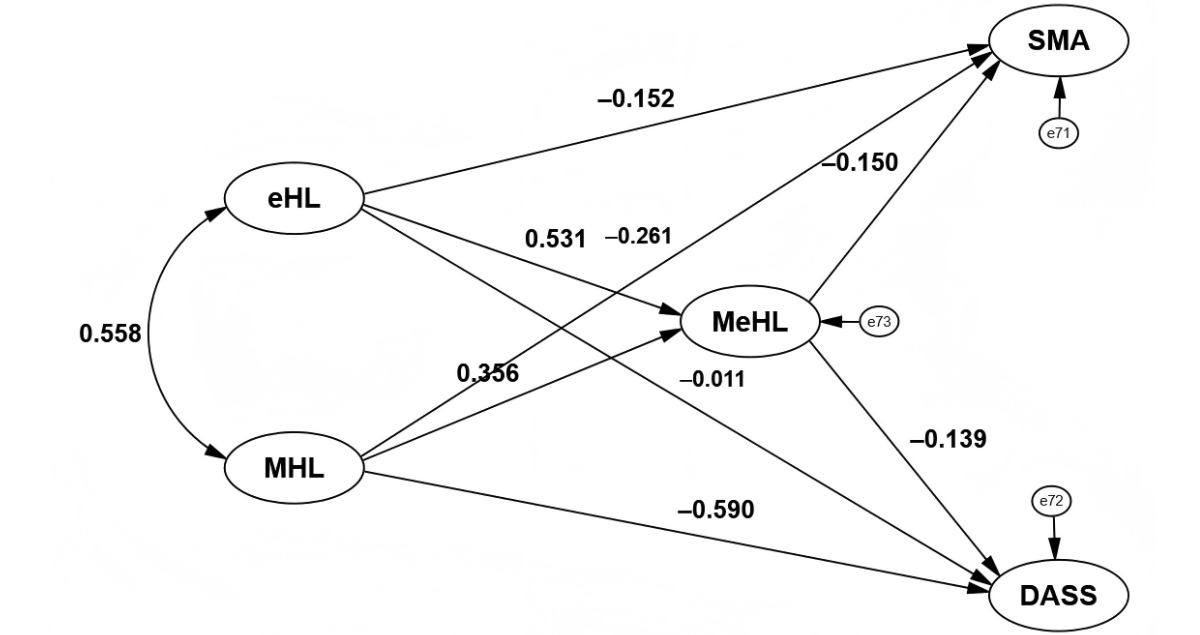
| Path | Estimate, β (95% CI) | SE | CRb | P value |
| eHLc → MeHLd | 0.531 (0.468 to 0.594) | 0.032 | 12.188 | <.001 |
| MHLe → MeHL | 0.356 (0.297 to 0.415) | 0.030 | 9.433 | <.001 |
| eHL → SMAf | –0.152 (–0.242 to –0.062) | 0.046 | –2.543 | .01 |
| MHL → SMA | –0.261 (–0.345 to –0.177) | 0.043 | –5.093 | <.001 |
| eHL → DASSg | –0.011 (–0.060 to 0.038) | 0.025 | –0.240 | .81 |
| MHL → DASS | –0.590 (–0.647 to –0.533) | 0.029 | –11.241 | <.001 |
| MeHL → SMA | –0.150 (–0.277 to –0.023) | 0.065 | –2.431 | .02 |
| MeHL → DASS | –0.139 (–0.207 to –0.071) | 0.035 | –2.743 | .006 |
aAll parameters estimated with cluster-robust SEs (clustered by classroom).
bCR: critical ratio.
ceHL: eHealth literacy.
dMeHL: mental eHealth literacy.
eMHL: mental health literacy.
fSMA: social media addiction.
gDASS: depression-anxiety-stress.
To further examine the mediation effects, we calculated the fully standardized indirect effects and their 95% bias-corrected CIs using bootstrap sampling with 5000 resamples and cluster-robust SEs (). The results indicated that both eHL and MHL exerted significant negative indirect effects on SMA through MeHL, as the 95% CIs for these paths did not contain zero. Specifically, the indirect effect of eHL was β=–0.062, 95% CI –0.125 to –0.010, and that of MHL was β=–0.045, 95% CI –0.090 to –0.008. In practical terms, this suggests that for every one standard deviation increase in eHL, SMA is expected to decrease by 0.062 standard deviations via the mediator. Similarly, the indirect effects on DASS were also significant (eHL: β=–0.037, 95% CI –0.072 to –0.009; MHL: β=–0.027, 95% CI –0.053 to –0.007). The proportion of the total effect mediated (relative effect size) for each path is also presented in .
| Path and effect type | Estimate, β (95% CI) | P value | Proportion mediated | ||||
| eHLb→ MeHLc→ SMAd | 34.4% | ||||||
| Mediation | –0.062 (–0.125 to –0.010) | .01 | |||||
| Total | –0.179 (–0.258 to –0.105) | .001 | |||||
| MHLe→ MeHL → SMA | 17% | ||||||
| Mediation | –0.045 (–0.090 to –0.008) | .01 | |||||
| Total | –0.264 (–0.350 to –0.188) | .001 | |||||
| eHL → MeHL → DASSf | 86.6% | ||||||
| Mediation | –0.037 (–0.072 to –0.009) | .008 | |||||
| Total | –0.043 (–0.087 to –0.004) | .03 | |||||
| MHL → MeHL → DASS | 77% | ||||||
| Mediation | –0.027 (–0.053 to –0.007) | .007 | |||||
| Total | –0.353 (–0.422 to –0.290) | .001 | |||||
aBootstrap CIs and P values are based on cluster-robust SEs (clustered by classroom). Estimates are fully standardized indirect effects (β).
beHL: eHealth literacy.
cMeHL: mental eHealth literacy.
dSMA: social media addiction.
eMHL: mental health literacy.
fDASS: depression-anxiety-stress.
In summary, the research results are consistent with a model in which MeHL plays a potential mediating role in the associations linking eHL and MHL to adolescent SMA and DASS. Specifically, higher levels of eHL and MHL were associated with higher MeHL, which in turn was linked to lower levels of SMA and psychological distress related to DASS. The study suggests a potential synergistic pathway of the “eHealth–mental health” dual-track mechanism that may be relevant for interventions targeting SMA and psychological distress, offering significant theoretical value and practical implications.
Moderation Effect Analysis
To explore the interaction between eHL and MHL in predicting MeHL, the study used a stepwise regression analysis with cluster-robust SEs to construct a 3-stage progressive model (). Model 1 serves as the baseline model, controlling for gender and age. The results show that demographic variables explain very little of the variance in MeHL (R2=0.008), though the overall model was not statistically significant (F=3.344, P<.05). Model 2 introduces eHL and MHL as predictors. Both have a significant positive effect on MeHL (eHL: β=0.535, 95% CI 0.472-0.598, P<.01; MHL: β=0.288, 95% CI 0.229-0.347, P<.01). The model’s explanatory power significantly increases (R2=0.544), with a ΔR2=0.536 compared to model 1, F=253.232, P<.001, indicating that these 2 forms of health literacy are important predictors of MeHL. Model 3 adds the interaction term of eHL and MHL (centered). The results show that the interaction term’s regression coefficient is significant (β=0.067, 95% CI 0.010-0.124; P<.05), and the model’s explanatory power slightly increases (R2=0.547, ΔR2=0.003, F=205.285, P<.001), indicating a synergistic effect between the two, enhancing their ability to predict MeHL.
| Variable | MeHLb | ||
| Model 1 | Model 2 | Model 3 | |
| Gender | 0.036 (–0.032 to 0.104) | –0.007 (–0.055 to 0.041) | –0.004 (–0.052 to 0.044) |
| Age | 0.083 (0.019 to 0.147) | 0.064 (0.016 to 0.112) | 0.063 (0.015 to 0.111) |
| eHLc | 0.535d (0.472 to 0.598) | 0.524d (0.461 to 0.587) | |
| MHLe | 0.288d (0.229 to 0.347) | 0.322d (0.263 to 0.381) | |
| eHL × MHL | 0.067f (0.010 to 0.124) | ||
| R2 | 0.008 | 0.544 | 0.547 |
| ΔR2 | — | 0.536 | 0.003 |
| F | 3.344f | 253.232g | 205.285g |
aAll models estimated with cluster-robust SEs (clustered by classroom). All reported coefficients are standardized regression coefficients (β) with 95% CIs in parentheses.
bMeHL: mental eHealth literacy.
ceHL: eHealth literacy.
dP<.01.
eMHL: mental health literacy.
fP<.05.
gP<.001.
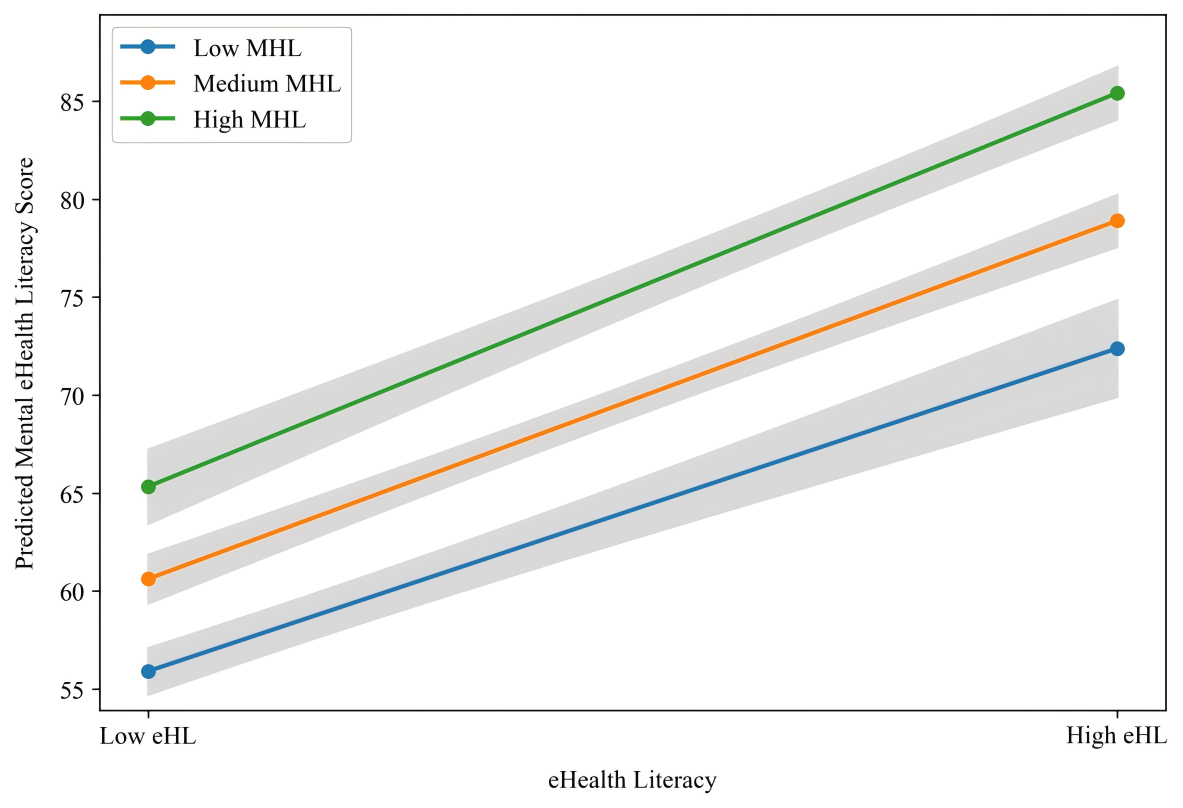
To further clarify the nature of the interaction, a simple slope analysis was conducted to probe the association between eHL and MeHL at low (mean – 1 SD), medium (mean), and high (mean + 1 SD) levels of MHL (). The analysis revealed a significant positive association between eHL and MeHL at low (b=1.040, 95% CI 0.881-1.199), medium (b=1.154, 95% CI 1.033-1.275), and high (b=1.268, 95% CI 1.131-1.405) levels of MHL. As visually represented in , which plots the predicted MeHL scores and their CIs, these results demonstrate a clear synergistic pattern: the positive relationship between eHL and MeHL grows progressively stronger as the level of MHL increases.
Moderated Mediation Effect Test
The study used the PROCESS (model 7) model proposed by Hayes in 2022 to test the mediation mechanism of MeHL in the relationship between eHL and SMA, as well as the moderating effect of MHL on this mediation path. In the analysis, all continuous predictor variables (ie, eHL and MHL) were mean-centered to reduce the impact of multicollinearity on the estimation of interaction terms. The bootstrap method was used for 5000 resamples to generate 95% bias-corrected CIs to assess the significance and stability of the moderated mediation effect. The Johnson-Neyman technique was used to precisely characterize the moderation pattern across the full range of MHL levels.
The moderated mediation analysis results (), estimated with cluster-robust SEs, demonstrate a consistent strengthening of indirect effects with increasing MHL levels. For SMA, the standardized indirect effect intensified from β=–0.084 at the 16th percentile to β=–0.099 at the 84th percentile of MHL, with a statistically significant pairwise contrast between high and low levels (Δ=–0.016, 95% CI –0.038 to –0.006). A more pronounced pattern was observed for DASS, where the indirect effect increased from β=–0.252 to β=–0.299 across the same percentile range, supported by a significant pairwise contrast (Δ=–0.047, 95% CI –0.102 to –0.008). The Johnson-Neyman analysis further confirmed that these mediation pathways remain statistically significant throughout the complete observed range of MHL, with no significant transition points identified. These findings indicate that higher levels of MHL significantly enhance the protective indirect effect of eHL on both behavioral and psychological outcomes through MeHL.
| Outcome variable, contrast, and MHLb percentile | Effect size, β (95% CI) | |||
| eHLc→ MeHLd→ SMAe | ||||
| Conditional indirect effect | ||||
| Low (16th) | –0.084f (–0.142 to –0.031) | |||
| Medium (50th) | –0.091f (–0.152 to –0.035) | |||
| High (84th) | –0.099f (–0.166 to –0.037) | |||
| Pairwise contrast (high vs low), Δ (95% CI) | –0.016g (–0.038 to 0.006) | |||
| eHL → MeHL → DASSh | ||||
| Conditional indirect effect | ||||
| Low (16th) | –0.252f (–0.358 to –0.151) | |||
| Medium (50th) | –0.273f (–0.382 to –0.169) | |||
| High (84th) | –0.299f (–0.418 to –0.185) | |||
| Pairwise contrast (high vs low), Δ (95% CI) | –0.016g (–0.038 to 0.006) | |||
aAll values are standardized coefficients (β). CIs and significance tests are based on cluster-robust SEs (clustered by classroom).
bMHL: mental health literacy.
ceHL: eHealth literacy.
dMeHL: mental eHealth literacy.
eSMA: social media addiction.
fP<.01.
gP<.05.
hDASS: depression-anxiety-stress.
Discussion
Principal Findings
This study proposed and tested a multidimensional health literacy model to elucidate the synergistic pathways through which eHL and MHL influence adolescent SMA and DASS, with MeHL as a mediator and MHL as a moderator. Our findings, supported by robust bootstrap CIs, provide precise estimates of these complex relationships. In support of our hypotheses, the findings revealed that (1) H1 was partially supported, as both eHL and MHL were significant negative predictors of SMA, with CIs indicating stable negative associations, but only MHL was a significant negative predictor of DASS, while the nonsignificant path from eHL to DASS suggests a negligible direct effect; (2) H2 was fully supported, with MeHL serving as a significant mediator in the relationships from both eHL and MHL to SMA and DASS, with all indirect effect CIs excluding zero; and (3) H3 was also supported, as MHL positively moderated the effect of eHL on MeHL, indicating a statistically significant though modest synergistic interaction that strengthened the proposed moderated mediation pathways to the outcomes.
Delving into the distinct associations posited in H1, our findings clarify the unique roles of different health literacies. These differential pathways align with yet extend previous research that has often examined these literacies in isolation. MHL demonstrated a robust negative association with DASS, suggesting it serves as a primary psychological resource for emotional regulation [], effectively breaking the “negative emotions–compensatory use” cycle [,]. This is consistent with population-based surveys that have identified MHL as a key correlate of psychological well-being in adolescents []. Conversely, eHL showed a more targeted association with reducing behavioral risks (SMA), equipping adolescents to navigate algorithmic “information cocoons” and use practical strategies like time management [,]. This finding resonates with large-scale studies linking digital competency to lower risks of problematic online behaviors, highlighting the role of eHL in mitigating specific behavioral risks rather than broad emotional distress []. Together, these dual pathways illustrate how distinct health literacies serve as protective resources. This mechanism aligns with the COR theory, as both literacies help adolescents conserve mental resources and mitigate digital threats []. Therefore, enhancing multidimensional health literacy constructs a dual barrier of “cognitive defense–behavioral regulation,” providing concrete intervention entry points.
The mediating role of MeHL (H2) represents a crucial synthesis of digital capability and psychological cognition. Our bootstrap analysis provides precise estimates of this integration, showing significant indirect effects from both eHL and MHL through MeHL. This result is consistent with the “triadic reciprocal model” in SCT, where personal factors (MHL), behaviors, and the digital environment interact continuously []. eHL provides the tool for information access, while MHL provides the cognitive framework for interpretation; their confluence fosters MeHL. This integration is critical, as individuals must not only find digital health information but also critically evaluate and apply it. The ability to identify and resist health misinformation is a key component of advanced health literacy, which our MeHL construct appears to capture []. Furthermore, general health literacy has been associated with more sophisticated information processing strategies, which may underpin the effective integration of digital and mental health knowledge reflected in MeHL []. Notably, the stronger mediation effect for eHL suggests the digital capability pathway is particularly dependent on this integrative process. MeHL thus plays a key role in the “knowledge internalization–behavioral transformation” process, offering a layered intervention path.
Most importantly, the supported moderated mediation hypothesis (H3) reveals a dynamic synergy at the heart of our model. The positive moderation effect indicates that higher MHL levels strengthen the effect of eHL on MeHL. This finding offers strong support for COR theory’s principle of resource caravans [], wherein existing resources (MHL) facilitate the acquisition and transformation of new resources (eHL). This boosting effect makes sense when we consider teenage brain development. Teenagers’ brains are especially tuned to seek rewards and are highly motivated to learn new things that help them adapt []. In this context, MHL may provide the necessary motivational and cognitive framework—the “why”—making the technical skills of eHL—the “how”—more valuable and worth applying to mental health contexts, thereby enhancing MeHL. This positions MHL as a “cognitive catalyst” that unlocks digital skills’ potential. Individuals with high MHL show greater cognitive processing depth when dealing with digital health information, while those with low MHL struggle to achieve behavioral transformation despite technical skills [].
In conclusion, this study challenges the siloed perspective of previous research by proposing and validating a comprehensive model that elucidates the dynamic interplay between different health literacies. Unlike earlier work that primarily examined eHL and MHL in isolation, our findings demonstrate that their synergistic association—where MHL catalytically enhances the utility of eHL—is crucial for understanding adolescent outcomes in the digital age. This integrated perspective is supported by research indicating that combined literacy interventions can be more effective, and our model provides a specific mechanistic account of this synergy []. This validated dual-path moderated mediation model provides a significant theoretical advancement by moving beyond direct effects to reveal a more complex relational network. Methodologically, our robust approach accounting for clustered data strengthens the ecological validity of these observed associations. These insights carry direct practical implications, providing an evidence-based blueprint for integrated health promotion that concurrently targets psychological cognition and digital competencies. Fostering this synergy represents a promising and efficient strategy for safeguarding adolescent well-being and building a healthier digital future.
Limitations
Notwithstanding its contributions, this study has several limitations that should be considered. The cross-sectional design precludes causal inference, leaving open the possibility of reverse causality, such as the potential for psychological distress to diminish health literacy acquisition. While common method bias was statistically assessed and fell below critical thresholds, the use of self-reported data may still introduce social desirability bias and inflate relationship estimates. Furthermore, the generalizability of the findings may be constrained by the regional sampling frame within China, and the omission of potential confounders such as socioeconomic status, academic pressure, and precise social media usage metrics means that the reported associations, though robust, may partially reflect the influence of these unmeasured variables. Future longitudinal studies incorporating objective behavioral data and a broader set of covariates in diverse cultural contexts are warranted to confirm the causal and generalizable nature of these synergistic pathways.
Conclusions
This cross-sectional study validates a new model that overcomes the limitations of previous research, which typically examined health literacy dimensions in isolation. It reveals the key role of eHL and MHL in reducing SMA and alleviating DASS among adolescents. The study shows that while both eHL and MHL contribute to reducing SMA, only MHL directly alleviates DASS. Additionally, MeHL plays a critical mediating role in this process. The innovation of this study lies in demonstrating that MHL is not merely an independent protective factor but an important moderator that enhances the effect of eHL in promoting MeHL. MHL provides the cognitive foundation for the effective application of digital skills, enabling adolescents to better use digital tools to manage their mental health, thereby maximizing the protective potential of digital skills. Therefore, public health strategies should focus on integrated interventions that simultaneously enhance both psychological resilience and digital competence, which is crucial for safeguarding adolescent well-being.
The authors declare that no generative artificial intelligence tools were used in the writing of any portion of this manuscript.
This research was supported by the National Social Science Fund of China under the major project (grant 23&ZD196). The funder was involved in the study design and provided supervision and mentorship throughout the manuscript preparation process.
The deidentified datasets generated and analyzed during this study are not publicly available due to restrictions in the ethical approval aimed at protecting adolescent participant confidentiality. However, they are available from the corresponding author, Zuosong Chen, upon reasonable request. Requestors will be required to complete a data use agreement, committing to use the data solely for noncommercial academic research purposes. The analysis code (IAMOS syntax and PROCESS macro) is also available upon request.
YTX contributed to the conceptualization, investigation, data curation, and formal analysis of the study, and was responsible for drafting the original manuscript. ZSC contributed to the conceptualization of the study, supervised the project, secured funding, and managed project administration, in addition to reviewing and editing the manuscript.
None declared.
Edited by S Brini; submitted 02.Aug.2025; peer-reviewed by J Peng, A Shivanna; comments to author 19.Sep.2025; accepted 30.Oct.2025; published 28.Nov.2025.
©Yuting Xu, Zuosong Chen. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 28.Nov.2025.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research (ISSN 1438-8871), is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.