Sample Page
Could the exoplanet TRAPPIST-1 e harbor alien life? : Short Wave : NPR
Written by
admin
in
7. Science
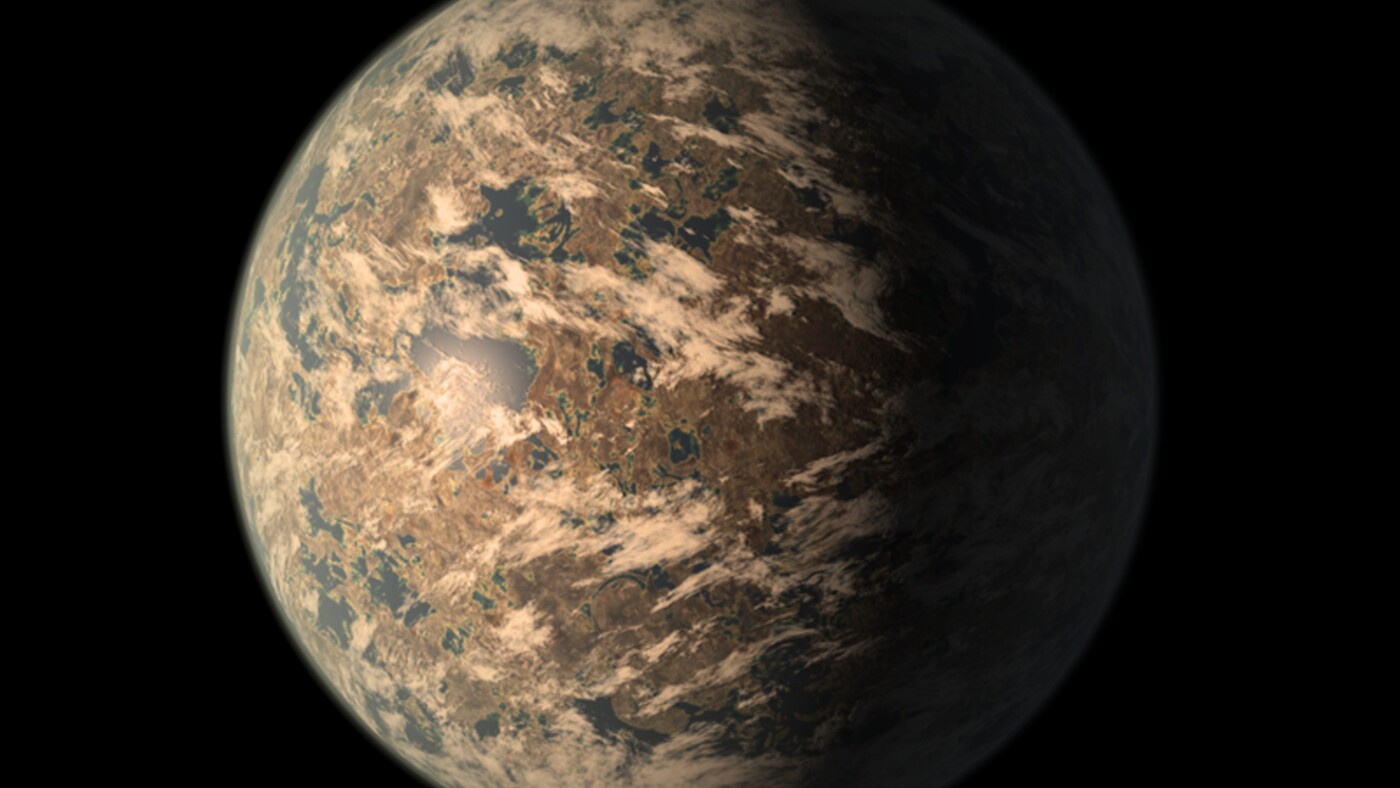
Artist’s impression of TRAPPIST-1e planet, as of 2018
…
Continue Reading
←
Taylor Swift reveals moment she broke down over Southport attack in new documentary
Mirakl Launches First-Ever Advertising Campaign, A Fully AI-Generated Christmas Film
→
More posts
Amazon Prime Video Pauses AI Video Recaps Following Plot Line Errors – PCMag
December 12, 2025
Aviation essential for the economy and calls for a national SAF fund
December 12, 2025
Tracking Chikungunya’s debilitating impact in East Africa
December 12, 2025
Practical Answers for Common Compliance Questions
December 12, 2025