The history of neurosurgery in Iraq is deeply rooted in ancient Mesopotamia, where early forms of surgical intervention, such as abscess drainage, were documented on cuneiform tablets. The scientific structure of neurosurgery in Iraq took shape in the 1950s, with the first elective neurosurgical procedure being carried out by Dr. Najeeb Al-Yaaqubi and was further formalized in 1966 by Dr. Saad Al-Witry, considered the father of Iraqi neurosurgery. A milestone was passed when 1972 the Neurosurgery Teaching Hospital was inaugurated in Baghdad; this became a central focal point for neurosurgical training and practice [6]. The history of neurosurgery development took another course in the Kurdistan region of Iraq when international collaborations aimed at building local neurosurgical capacities in cities like Duhok started in 2012 [7].
The research findings are useful in understanding the role of the neurosurgical virtual laboratory at Neuroscience Hospital, Baghdad (Figs. 3, 4 and 5). The neuroscience hospital at Baghdad uses a stepwise, competency-based educational model in the neurosurgical lab. This was mainly developed through simulation-based training on clinically relevant scenarios. Iterative practice further reinforces learning, whereby immediate feedback from mentors during the process provides participants with opportunities to refine techniques and decision-making. It provided a very excellent avenue of professional growth between mentors and mentees. The mentors then took the mentees through iterative learning cycles of providing personalized feedback and clinical insights that could help fine-tune surgical precision and decision-making. Teaching in the neurosurgical lab was led by experienced neurosurgeons and senior residents with specialized expertise in simulation-based training.
Neurosurgical Training Facilities at Neuroscience Hospital, Baghdad. (A) Microscope stations and 3D training models used by residents for hands-on neurosurgical simulation and skill development. (B) A collection of photos showcasing collaborative workshops and innovation sessions between neurosurgery residents, faculty members, and international visitors, underscoring the importance of mentorship and skill sharing in the lab
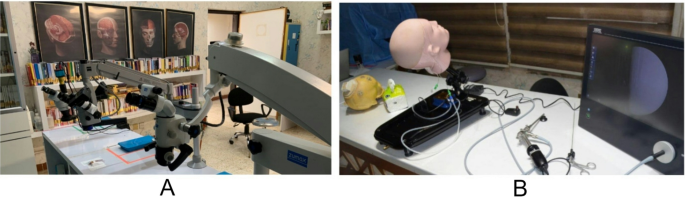
Advanced Neurosurgical Training Equipment at Neuroscience Hospital, Baghdad. (A) High-resolution microscopes used for neurosurgical simulations, enabling residents to practice precision techniques in a controlled environment. Anatomical posters and reference books support theoretical learning alongside practical skills. (B) Endoscopic training setup featuring a head model and monitor, simulating real-time surgical procedures for enhancing skills in minimally invasive neurosurgery
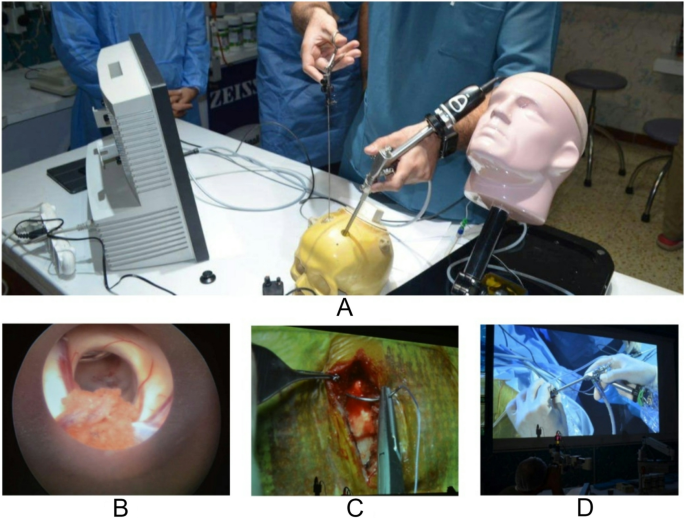
Endoscopic and Microsurgical Simulation in Neurosurgical Training at Neuroscience Hospital, Baghdad. (A) Hands-on endoscopic training using a skull model, allowing residents to practice minimally invasive neurosurgical techniques. (B) Endoscopic view displaying the needed anatomy during a simulated procedure, enhancing visual-spatial understanding. (C) Microsurgical practice with high magnification, providing precision skill training in surgical anatomy and dissection. (D) Live demonstration of microsurgical techniques projected on a screen, used for educational purposes in ongoing resident workshops and seminars
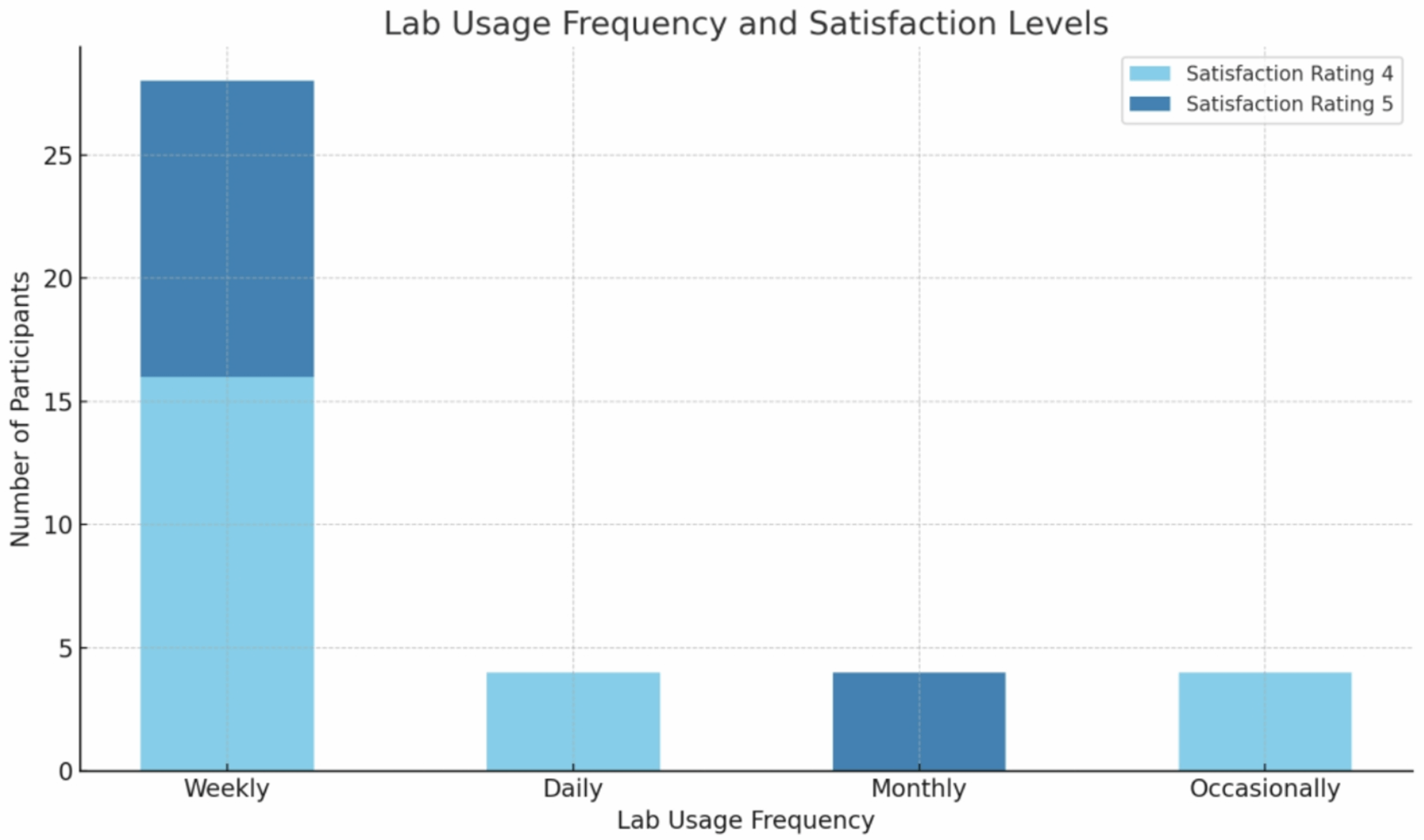
A considerable proportion of participants (70%) reported weekly lab use, indicating that the facility is integral to their training and practice. Moreover, overall satisfaction with the lab experience was high, with 60% rating their satisfaction as 4 and 40% rating it as 5. This suggests that the lab is meeting the expectations of its users across various levels of experience. Notably, the chi-square test revealed a statistically significant association between satisfaction and the frequency of lab use (p = 0.010), highlighting that those who use the lab more frequently are more likely to be satisfied with their experience. Interestingly, satisfaction was not significantly influenced by gender (p = 0.519), indicating that both male and female participants had comparable satisfaction levels. However, years of neurosurgical experience significantly affected satisfaction (p = 0.009), with participants having more than 15 years of experience showing the highest levels of satisfaction. The gender distribution was skewed toward male participants, reflecting the broader gender imbalance currently observed in the neurosurgical field in our region.
The results demonstrate the high perceived educational value of various lab resources. The microscope and training models were consistently rated highly, with 40% of participants giving a maximum score of 5 for both tools. The impact of the 3D printers is rated lower: 20% gave a score of 5, and 40% gave a score of 4. This suggests variability in either utilization or perception of this resource. For medical textbooks, the rating was incredibly positive for 40% of the respondents.
In the article about the surgical skills in neurosurgical residency training, Liu et al. [8] focused on the especially important role of neurosurgical residency training in the context of surgical skills laboratories. They sought to enhance residents’ technical skills in complex skull base operations through a cadaveric-based, structured dissection curriculum and modern equipment at Cleveland Clinic. Furthermore, three-dimensional printing has evolved to be a robust neurosurgical education and anatomy training tool. Thiong’o et al. (2021) [9] describe the role that 3D printing plays in neurosurgical simulation, including skull base surgery and vascular procedures, to practice complex surgical skills outside the operating theater. It has proved beneficial in decreasing the learning curve for difficult procedures. Also, Baskaran et al. (2016) [10] point out that 3D printing precision in generating anatomical models from patient-specific data has dual benefits including improved surgical training and preoperative planning. Realistic simulation of neurosurgical tasks can be developed using additive manufacturing processes such that skill acquisition is improved, and patient outcomes are positive. Innovative problem-solving using 3D printing received a wider range of responses, topping at 30%, rating it 2. This would suggest that while 3D printing is recognized as important, it is not yet integral to every participant’s training or practice, probably because of its recent introduction or unfamiliarity with the technology.
Research has often been central to the goals that decide career choices and build surgical skills in medical students. Awad et al. (2016) [11] note that this trend is notably reflected in the number of medical students who receive research grants, of which more than 50% go on to pursue a residency in neurosurgery. Additional support for this view is inferred from the fact that 40% of the participants rated the lab’s role in research skills as 4, and 30% rated it as 5. Likewise, leadership and decision-making skills promoted by the non-medical resources of the lab are also rated to be four by 50% of the participants and rated to be five by 20%. This shows that the role of the laboratory goes beyond technical skills to include research competencies regarding professional development. 60% of all the participants highly rated the lab’s contribution to fostering innovation. The entire neurosurgical residency is six years in length, during which time the critical emphasis in each year has been tailored, almost in a pillar-like fashion. Lab training is organized in such a way that it complements this pillar development and progressively increases in intensity from foundational-level lab skills to more advanced surgical-based decision-making as the years progress.
The integration of neurosurgery into the curricula of medical schools remains an important underdeveloped feature in the medical education system worldwide. Lee et al. (2020) [12] study indicated that the level of neurosurgical exposure varied grossly across different regions, with only 39.7% of students reporting any form of neurosurgical experience during their education. The idea is that regular use of the lab enhances participants’ ability to innovate in their practice. Kato et al. (2020) [1] review global disparities in neurosurgical education between developed and developing countries. Despite advances in surgical techniques or diagnostic tools, many developing regions still face huge barriers, including access to limited resources, training, and modern technology. They also advocate for international collaboration to close these gaps and support programs. Kanmounye et al. (2020) [13] discuss how the role of the Foundation for International Education in Neurological Surgery has transformed to decrease global neurosurgical disparity through education. Until recently, FIENS, founded in 1969, focused on brief mission trips but, since then, has transformed into a more sustainable model through the education of local neurosurgeons and the establishment of residency programs in LMICs. This model, labeled “service through education,” has enhanced the development of neurosurgical systems in LMICs and has led to a sustainable effect due to local ownership and international cooperation.
Limitations
This study has several limitations. The sample size is relatively small, limiting the generalizability of findings to a broader population of neurosurgeons and trainees. Additionally, the study relies on self-reported data, which may introduce response bias. The cross-sectional design does not allow for the assessment of the long-term impacts of the neurosurgical lab on clinical outcomes. The survey instrument was developed specifically for this study and has not been previously validated, which may influence the reliability and interpretability of the results. Moreover, all participants were active users of the lab, which may introduce selection bias and lead to an overestimation of satisfaction and perceived benefit. Furthermore, while the study highlights the effectiveness of simulation-based training, it does not compare outcomes with traditional training methods. Future research should incorporate larger cohorts, objective skill assessments, and longitudinal follow-up to validate these findings.