Burden of pancreatitis attributable to high alcohol use
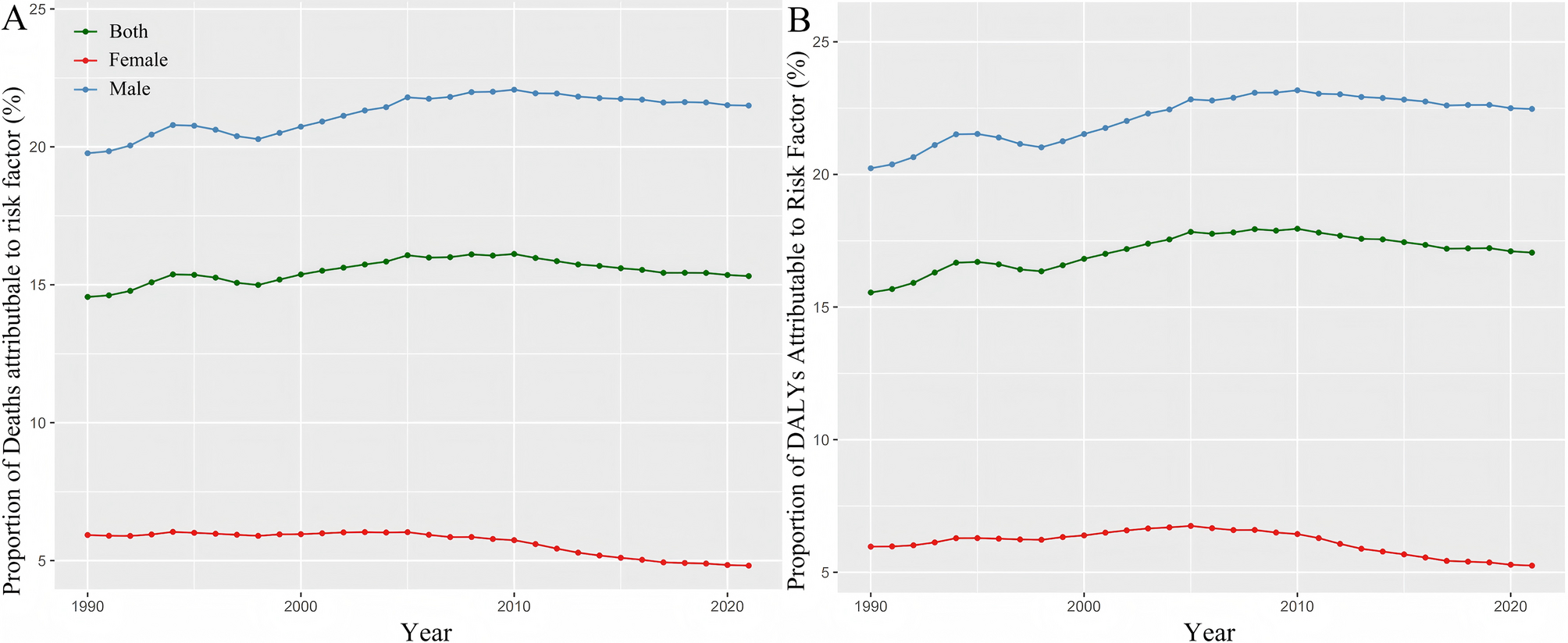
We analyzed the burden of pancreatitis-related deaths and DALY attributable to high alcohol use, incorporating specific data on temporal trends and gender differences. As shown in Fig. 1, the global proportion of pancreatitis deaths attributable to high alcohol use remained relatively stable at approximately 16% between 1990 and 2021. However, significant gender differences were observed in deaths and DALY burdens attributable to high alcohol use. From 1990 to 2021, the proportion of male deaths attributable to high alcohol use increased from approximately 19.77% to a peak of 22.07% in 2010, before slightly declining to stabilize at about 21.5% in 2021. In contrast, the proportion of female deaths remained consistently lower, decreasing from 5.93% in 1990 to around 4.82% in 2021. Regarding DALY, the proportion among males rose from 20.23% in 1990 to 23.17% in 2010, stabilizing at approximately 22.47% in 2021. For females, the proportion slightly increased from 5.97% in 1990 to 6.59% in 2008, before declining to 5.25% in 2021. Overall, the results indicate that the burden of pancreatitis attributable to high alcohol use is significantly higher among males than females.
Proportion of Pancreatitis-Related Deaths (A) and DALYs (B) Attributable to High Alcohol Use by Gender, 1990–2021
As shown in Fig. 2, the number of deaths and total DALY attributable to high alcohol use exhibited an upward trend from 1990 to 2021, with a significantly higher burden among males than females. Deaths attributable to high alcohol use among males increased from approximately 8,444 to 16,563, while female deaths rose from about 1,527 to nearly 2,186. The crude mortality and DALY rates among males were consistently higher than those among females, rising from approximately 0.31 per 100,000 and 13.07 per 100,000 in 1990 to 0.41 per 100,000 and 15.95 per 100,000 in 2021, respectively. Although age-standardized mortality and DALY rates for males showed a slight downward trend during the study period, the changes in these indicators for females were minimal, and their overall burden remained at relatively low levels.
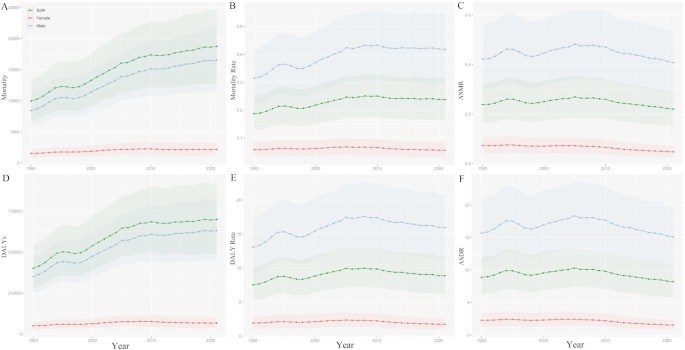
Global Burden of Pancreatitis Attributable to High Alcohol Use by Gender, 1990–2021: (A) Mortality, (B) Mortality Rate, (C) ASMR, (D) DALYs, (E) DALY Rate, (F) ASDR
Trends in the burden of pancreatitis globally and across different SDI regions from 1990 to 2021
From 1990 to 2021, the global number of new pancreatitis cases increased from 1,728,141 (1,495,096 to 1,995,752) to 2,747,368 (2,413,878 to 3,133,076) (Fig. 3 A); deaths rose from 68,490 (60,748 to 78,272) to 122,416 (109,848 to 141,362) (Fig. 3D); and DALYs grew from 2,583,402 years (2,265,738 to 2,985,509) to 4,101,154 years (3,647,631 to 4,684,283) (Fig. 3G). The incidence rate increased from 32.4 per 100,000 people (28.03 to 37.42) to 34.81 (30.59 to 39.7) (Fig. 3B), mortality from 1.28 (1.14 to 1.47) to 1.55 (1.39 to 1.79) (Fig. 3E), and DALY rate from 48.44 years (42.48 to 55.98) to 51.97 (46.22 to 59.36) (Fig. 3H). The age-standardized incidence rate (ASIR) declined from 37.62 (32.57 to 43.46) to 32.81 (28.85 to 37.38) (Fig. 3 C), the age-standardized mortality rate (ASMR) from 1.69 (1.5 to 1.92) to 1.45 (1.3 to 1.67) (Fig. 3 F), and the age-standardized DALY rate (ASDR) from 57.39 years (50.34 to 66.07) to 48.43 (43.07 to 55.35) (Fig. 3I). Globally, the net drift for ASIR, ASMR, and ASDR were − 0.44% (−0.42 to −0.46), −0.49% (−0.47 to −0.51), and − 0.55% (−0.52 to −0.58) per year, respectively (Table 1).
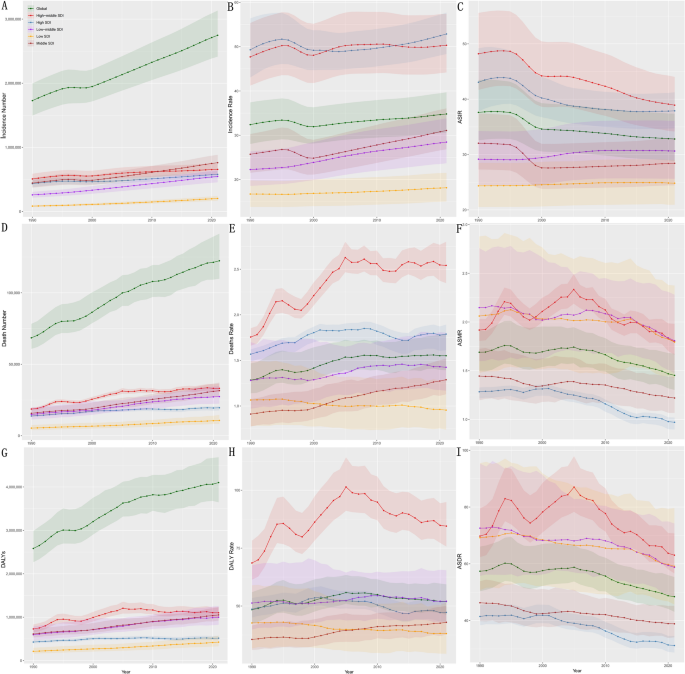
Trends in Global and SDI-Specific Pancreatitis Burden, 1990–2021: (A) Incident Number, (B) Incidence Rate, (C) ASIR, (D) Death Number, (E) Deaths Rate, (F) ASMR, (G) DALYs, (H) DALY Rate, (I) ASDR
The incidence rates in all five SDI regions show a slow upward trend. Mortality and DALY rates in high-middle SDI and middle SDI regions are increasing, with the high-middle SDI region showing the most significant rise, while mortality and DALY rates in low SDI regions exhibit a slow downward trend (Fig. 3). In low SDI regions, the incidence rate increased from 16.74 per 100,000 people (13.83 to 19.81) to 18.16 (15.04 to 21.51) (Fig. 3B), and ASIR rose from 24.34 (20.52 to 28.51) to 24.83 (20.93 to 28.97)(Fig. 3 C). However, ASMR and ASDR declined from 2.06 (1.48 to 2.88) to 1.79 (1.42 to 2.37) and from 69.2 years (50.74 to 95.49) to 59.12 (45.64 to 79.64), respectively (Fig. 3 F and I). In low-middle SDI regions, the incidence rate increased from 22.27 (18.58 to 26.36) to 28.46 (23.69 to 33.82) (Fig. 3B), mortality rate rose from 1.28 (0.97 to 1.7) to 1.42 (1.17 to 1.8) (Fig. 3E), and DALY rate grew from 51.28 years (39.85 to 67.57) to 52.06 (43.03 to 65.44) (Fig. 3H). In middle SDI regions, the incidence rate grew from 25.72 (21.53 to 30.29) to 31.08 (26.83 to 36.07) (Fig. 3B), whereas ASIR declined from 32.04 (27.29 to 37.41) to 28.42 (24.42 to 32.92) (Fig. 3 C); mortality and DALY rates decreased to 1.29 (1.13 to 1.52) and 42.98 years (37.65 to 50.11), respectively (Fig. 3E and H). In high-middle and high SDI regions, ASIR, ASMR, and ASDR all declined significantly (Fig. 3 C, F and I). In high SDI regions, ASMR dropped from 1.28 (1.21 to 1.33) to 0.97 (0.9 to 1.02) (Fig. 3 F), and ASDR fell from 41.45 years (38.33 to 45.55) to 31.21 (28.72 to 34.55) (Fig. 3I). Net drift analysis shows a slight positive growth in ASIR (0.06%) in low SDI regions, while ASMR and ASDR in high SDI regions declined most rapidly, at −0.89% and − 0.91%, respectively (Table 1).
Globally, while the ASIR, ASMR, and ASDR have shown a downward trend, the mortality and DALY rates in high-SDI regions have increased, contrary to the general expectation that the burden in areas with higher social development levels should decrease. This anomaly may be related to changes in alcohol consumption patterns, shifts in dietary habits, or the increasing prevalence of chronic disease comorbidities. Additionally, in low-SDI regions, although the incidence of pancreatitis is on the rise, mortality and DALY rates have slowly decreased. This paradox may reflect the gradual improvement in healthcare levels in these regions, as well as enhancements in early disease diagnosis and intervention measures.
Eastern Europe ranks highest globally in ASDR at 240.99 (278.40 to 211.60), ASMR at 5.60 (6.07 to 5.15), and ASIR at 99.35 (117.93 to 82.69). Western Sub-Saharan Africa ranks second globally in ASMR at 3.23 (4.02 to 2.44) and ASDR at 106.59 (135.71 to 79.03). The High-income Asia Pacific region has the lowest ASDR at 16.87 (20.8 to 13.99) and ASMR at 0.47 (0.51 to 0.41), while Tropical Latin America shows the lowest ASIR at 16.63 (18.83 to 14.70). Other regions, such as High-income North America with an ASIR of 51.99 (55.53 to 48.36) and Central Asia with an ASIR of 47.94 (55.37 to 41.43), display relatively high incidence rates but remain lower than those in Eastern Europe (Fig. 4).
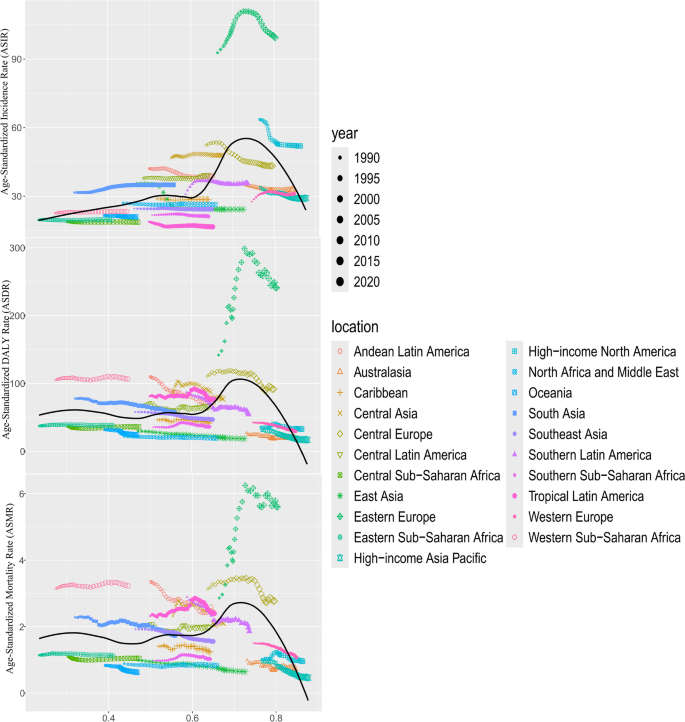
Trends in Age-Standardized Incidence Rate (ASIR), Disability-Adjusted Life Year Rate (ASDR), and Mortality Rate (ASMR) of Pancreatitis by Location from 1990 to 2020
It is noteworthy that Eastern Europe has the highest ASIR, ASMR, and ASDR globally, significantly surpassing other regions. This marked disparity may be attributed to factors such as the region’s long-standing high alcohol consumption, limited healthcare resources, and a heavy burden of chronic diseases. In contrast, the high-income Asia-Pacific region has the lowest burden indicators, particularly ASDR and ASMR, which may be due to lower alcohol consumption rates, more comprehensive public health systems, and effective preventive measures.
In 2021, the global burden of pancreatitis exhibited significant differences across countries and regions.The three countries with the highest ASDR were the Russian Federation (260.76, 300.90 to 229.71), the Republic of Moldova (222.06, 260.97 to 184.93), and Ukraine (203.99, 269.68 to 148.48).The three countries with the highest ASIR were the Russian Federation (102.24, 121.76 to 84.68), Ukraine (96.94, 115.45 to 80.12), and the Republic of Moldova (86.36, 103.99 to 71.43).The ASMR peaked in the Russian Federation (6.28, 6.79 to 5.82), the Republic of Moldova (5.57, 6.45 to 4.78), and Kazakhstan (4.97, 6.32 to 3.93) (Fig. 5).
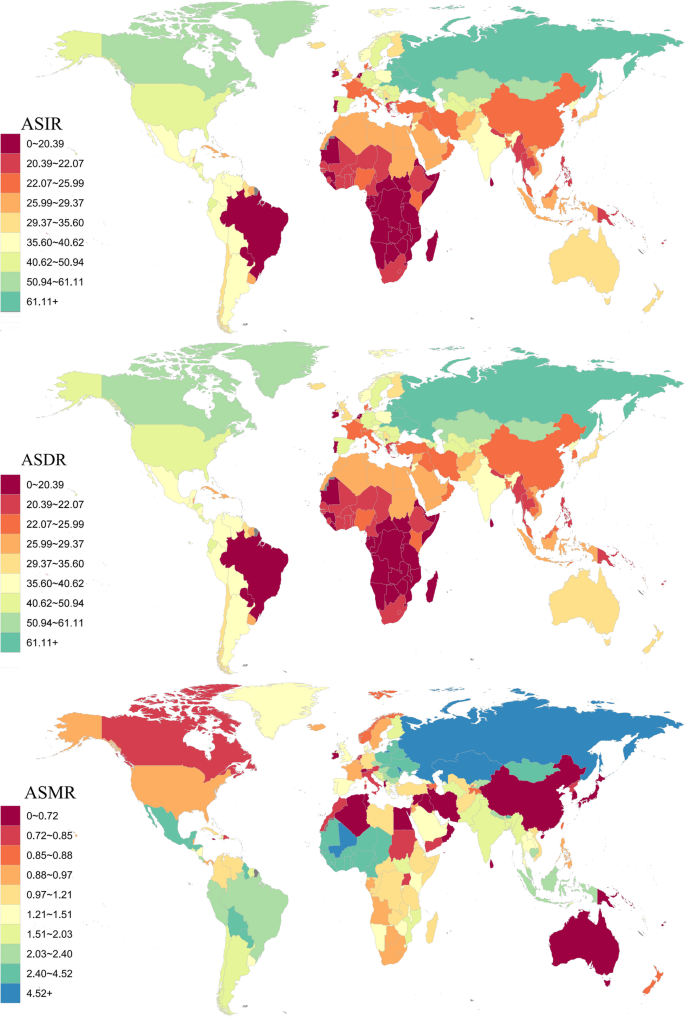
Global maps showing the Age-Standardized Incidence Rate (ASIR), Disability-Adjusted Life Year Rate (ASDR), and Mortality Rate (ASMR) of Pancreatitis in 2021
Analysis of age, period, and cohort effects for pancreatitis globally and across different SDI regions
From the Figs. 6 and 9, it is evident that the incidence, mortality, and DALY rates of pancreatitis globally and across SDI regions increase significantly with age.In high SDI and high-middle SDI regions, the incidence and DALY rates rise sharply after age 50, peaking in the 85–89 age group.Mortality also increases gradually with age, though the growth rate slows in older age groups (80 years and above).In middle SDI regions, the incidence and DALY rates rise significantly after age 70, though the overall trend is slightly lower than in high SDI regions.In low-SDI regions, the growth curve for incidence and DALY rates is more gradual, but it also increases notably after age 70, with the DALY rate peaking after age 80.Mortality rates in low-middle SDI and low-SDI regions are higher across all age groups, with particularly pronounced increases after age 70.The peak age for DALY rates also varies: in high SDI and high-middle SDI regions, the peak occurs at 75–79 years, while in low SDI regions, it appears after age 80, highlighting distinct age effect characteristics across SDI regions.
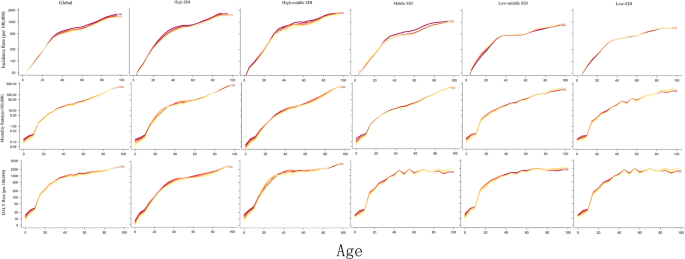
Age effect analysis of incidence rate, mortality rate, and DALY rate of pancreatitis in global and different SDI regions from 1990 to 2021
Between 1990 and 2021, the incidence, mortality, and DALY rates in high SDI and high-middle SDI regions showed stable or declining trends after 2000, with DALY rates in high SDI regions decreasing most significantly.The incidence rates in high SDI and high-middle SDI regions have changed little since 2000, while mortality rates began declining gradually after 2005.In middle-SDI regions, incidence rates slightly increased between 2000 and 2015 before stabilizing, while mortality and DALY rates showed minimal variation.In low-middle SDI and low SDI regions, incidence rates have slightly increased since 2000, with a more pronounced rise in low SDI regions.Mortality and DALY rates in low-middle SDI and low SDI regions have remained consistently high, with slight increases in some years for low SDI regions.Overall, distinct patterns are observed across SDI regions. The burden in high-SDI regions has gradually declined, whereas the burden in middle- and low SDI regions has remained high over the past 20 years, with some indicators continuing to rise (Figs. 7 and 9).
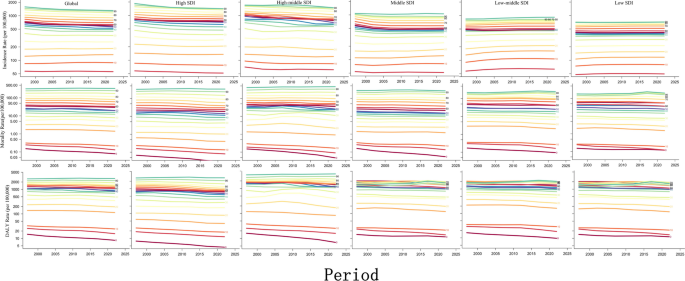
Period effect analysis of incidence rate, mortality rate, and DALY rate of pancreatitis in global and different SDI regions from 1990 to 2021
The cohort effects globally and across SDI regions indicate that incidence, mortality, and DALY rates for recent birth cohorts (e.g., those born in 2000) are significantly higher than for earlier cohorts (e.g., those born in 1895).The cohort effect is most pronounced in low SDI regions, where risks have risen rapidly in recent birth cohorts, with incidence, mortality, and DALY rates peaking in the 2000 birth cohort.The cohort effect curve in middle SDI regions also shows a clear upward trend, though the magnitude is slightly lower than in low SDI regions.In contrast, the cohort effect in high SDI and high-middle SDI regions has increased more moderately, with slight rises in incidence, mortality, and DALY rates among recent birth cohorts.The burden difference between earlier and recent birth cohorts in high SDI regions is small, while recent birth cohorts in high-middle SDI regions show a certain degree of increase.Globally, the cohort effect grows significantly with birth year, with low SDI and middle SDI regions showing the most pronounced growth and the largest increases in burden (Figs. 8 and 9).
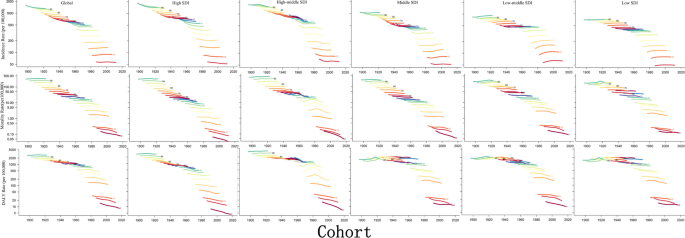
Cohort effect analysis of incidence rate, mortality rate, and DALY rate of pancreatitis in global and different SDI regions from 1990 to 2021
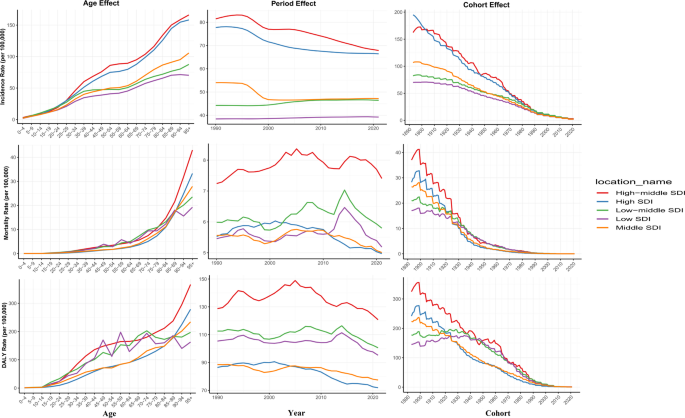
Combined analysis of age, period, and cohort effects on pancreatitis across different SDI regions