The study shows that the prevalence rate of SD is 20.2%, significantly higher than the prevalence rate (4.0%) obtained by WY Li et al. [5] using a random effects model for meta-analysis. There is no significant statistical difference between the prevalence rate of men and women(21.7% for men and 19.1% for women). This result is inconsistent with the systematic evaluation results of WY Li et al. (5% for men and 15% for women). The prevalence rates of the 10 included literature ranged from 2.27 to 65.45% [9, 22,23,24,25]. Firstly, the research subjects include elderly people in emergency hospitalization, rehabilitation, long-term care institutions, and communities, while Nagano et al. [26] research subjects only include old women who underwent hip fracture surgery; Secondly, there are significant differences in the methods used to evaluate swallowing function and skeletal muscle included in the literature; Thirdly, among the 10 articles, 8 are from Japan, 1 is from South Korea, and 1 is from Türkiye, so regional bias cannot be ruled out. Although we obtained a lower prevalence rate than Sakai, K et al. [27] who used the same evaluation methods (CC, WST) (20.2% vs. 35.1%), but we included a larger sample size (3134 vs. 245); This may be the reason for the difference. Therefore, further verification is needed in a wider population. Although the assessment methods for sarcopenia and swallowing disorders were different in these studies, their final conclusions emphasized the strong correlation between swallowing disorders and sarcopenia.
Comparison with previous studies
Our study confirms previous research findings that SD is associated with aging, low BMI, frailty, malnutrition, oral weakness, and comorbidity in patients. Age has been identified as an independent risk factor for SD [28, 29]. To verify this viewpoint, we conducted a stratified analysis of age and found that the difference in incidence rate between the 65–74 age group and the ≥ 85 age group (5.7% vs. 37.8%) was significantly increased.
compared to the previous studies, we new found that SD was also related to marital status, educational level, main caregivers, income, psychology, etc. Divorced, widowed, or single older patients have a higher incidence of SD than while married individuals indicate a higher quality of life [30, 31]. Most studies have reported a positive correlation between marital status and health, and the research results are consistent across different cultures and countries. Gender has a significant impact, with males exhibiting greater health benefits than females [32]. The incidence rate of illiterate patients is significantly higher than that of other cultural levels, and the level of education is closely related to the patient’s cognitive level and self-care ability. Low educated individuals have limited understanding of diseases, and may overlook the adverse effects of oral health, nutrition, and other factors on diseases, which also indicates lower levels of healthcare [33]. The incidence rate of patients who need professional care is 4.7 times that of patients who can take care of themselves. Being able to take care of themselves means higher self-care ability and more activity, so their risk of muscle reduction is lower. Patients with monthly income exceeding 10,000 RMB have an increased risk of SD. The possible reason is that high-income patients are more likely to have access to high-quality living and high-level medical care, resulting in longer lifespans [34]. Therefore, the real risk of SD for these older patients is not income itself, but the age increase brought about by high income. It is not economic income that affects the prevalence of SD, but age that affects SD [35].This speculation requires further research to verify.
Research has found that SD is closely related to patients’ daily habits and abilities. Reduced self-care ability, lack of participation in community activities, and lack of housework were independent risk factors for SD. Self-care ability reflects the patient’s independent activity ability, the worse the self-care ability, the lower the activity ability, the higher the incidence of disease. The incidence of SD in patients with regular daily activities and physical exercise was significantly lower than that in patients who basically did not take part in outdoor physical exercise, community activities, housework and irregular life, indicating the importance of older people to strengthen daily exercise and maintain healthy and positive living habits in preventing the occurrence and development of SD, which also verified the role of lifestyle medicine in reversing and preventing diseases [36]. Surprisingly, non-drinking and non-smoking patients showed a higher prevalence rate than those who smoked and drank. However, in China, there is a significant gender gap in alcohol consumption and smoking, and gender bias cannot be ruled out.
SD is related to the physical health status of patients. Low BMI, frailty, poor oral health [37], are independent risk factors for SD. The impact of oral health on the prevalence of SD has been confirmed by previous studies [38, 39], however, according to Japanese diagnostic algorithm for SD, the tongue pressure is an important indicator to comfirm whether it has SD or not. The tongue pressure detectors is too expensive to widely use in the institution, therefore there need a simple and cheap tool to know the swallowing muscle strength. Our study used Zhao’s Chinese version of the Brief Oral Health Status Examination (BOHSE) [10] score to describe oral health. This table has 10 entries, including lymph nodes, lips, tongue, mucosa, gums, saliva, natural teeth, artificial teeth, number of chewing teeth, and oral hygiene. Each project is graded from 0 (normal) to 2 (problematic), with scores ranging from 0 to 20. The higher the score, the more severe the oral problems. Our study result showed that the total score of BOHSE will increase the risk of patients suffering from possible SD by 1.144 times increasing each score. Poor oral health, also known as oral debilitation [40], includes diseases such as tooth loss, dry mouth, inflammation of oral soft and hard tissues, which may lead to a decrease in the amount and quality of food intake, causing malnutrition and a reduction in skeletal muscle throughout the body, ultimately resulting in swallowing disorders, forming a vicious cycle, and overall deterioration of the patient [41, 42]. Given the severe situation and harm of poor oral health, the World Health Organization has identified it as an important public health issue worldwide [43]. The European Elderly Oral Health Policy Recommendations provide early oral health management for the older people [44].
Aging, decreased self-care ability, lack of participation in community activities, avoidance of household chores, low BMI, frailty, and poor oral health are independent risk factors for SD in our study which is consistent with the main risk factors for sarcopenia (age, nutrition, activity, disease, oral weakness, etc.), but our research also found that certain demographic characteristics, daily habits, and psychological cognitive disorders of patients are closely related to SD. This reminds us that when evaluating and intervening in SD, we should not only pay attention to the patient’s physical illness, but also to their individual differences, lifestyle habits and abilities, as well as psychological and cognitive issues. So as to reduce the incidence rate of SD, improve the self-care ability and quality of life of older patients, and reduce the medical finance and family economic burden. However, becaese of the lack of definite SD (due to the absence of DXA/BIA and tongue pressure data) weakened the specificity of the research results. Future research should use standardized SD standards to validate these results.
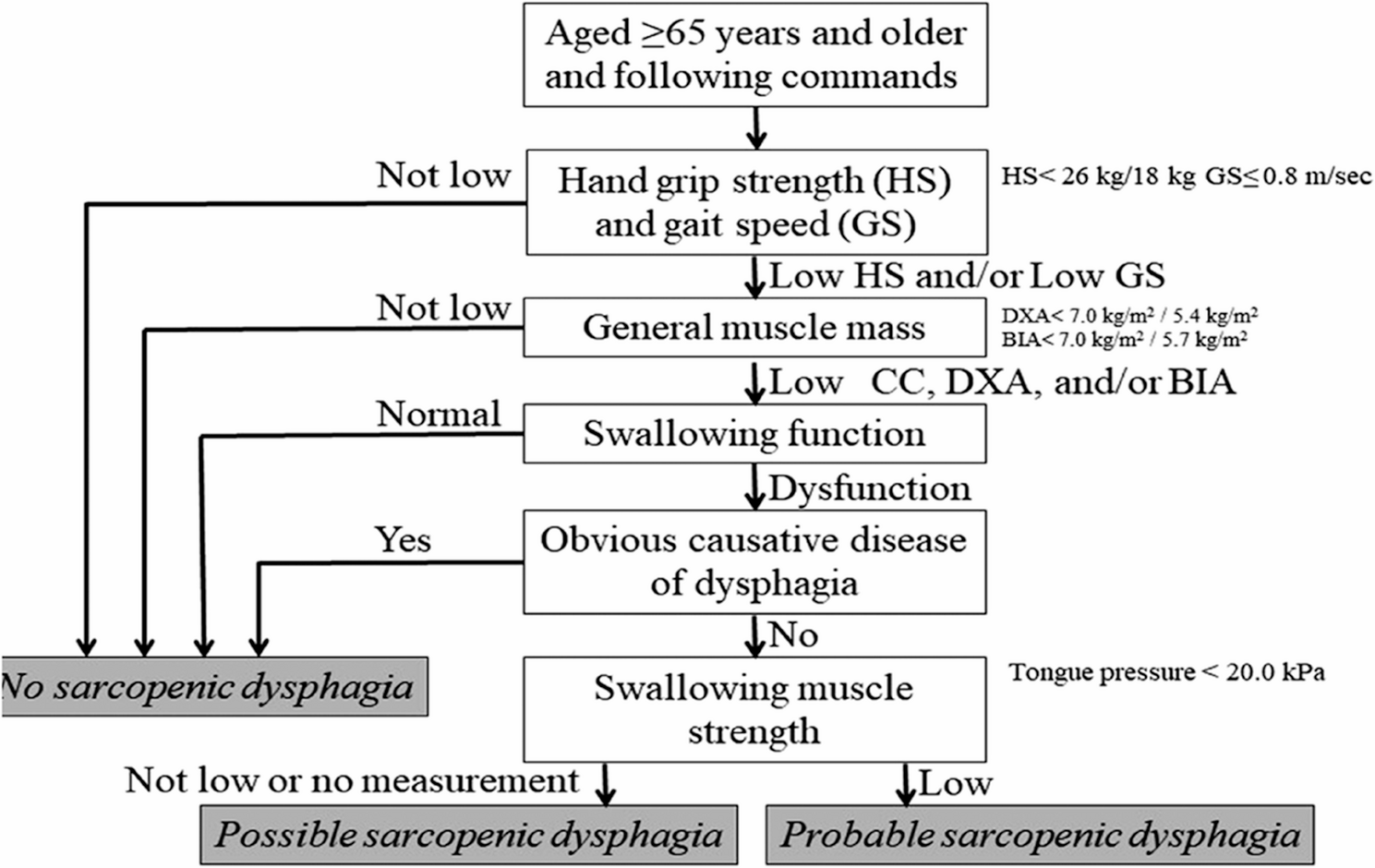
As a relatively new concept, SD has not been formally introduced in China and lacks unified diagnostic criteria. Currently, there is no large-scale population study on it. It is feasible for us to use CGA data and a SD diagnostic algorithm developed by Japanese researchers to diagnose SD, laying the groundwork and making efforts for research in this field. The advantage of this diagnostic algorithm is that it can diagnose very likely or possible SD without assessing swallowing muscle mass, its disadvantage lies in the inability to diagnose specific SD, as it is currently impossible to accurately assess swallowing muscle mass and determine its cutoff value. This may lead to biased research results.Therefore, more research is needed to optimize and improve this diagnostic algorithm, and to unify relevant evaluation tools, such as integrating DXA, BIA, Tongue pressure assessment and imaging examination. The use of this diagnostic algorithm should be improved, and all qualified clinical medical personnel should be able to use the tool correctly to promote the research and management of SD in clinical practice, and to improve the evaluation and intervention rate of SD in clinical practice.
Limitations
This study is a retrospective cohort study based on single center CGA data from Southwest China, with a focus on elderly hospitalized patients in the geriatric department. The results may not represent the prevalence of SD in the entire elderly population in the country. According to the Japanese diagnostic algorithm, SD is divided into three types (definite, very likely, and possible). However, due to the lack of DXA or BIA data, or even tongue pressure, the study did not include definite sarcopenic dysphagia. And the current study has not yet determined the critical value of swallowing muscle mass, According to the diagnostic algorithm, it is impossible to diagnose definite dysphagia without evaluating swallowing muscle mass. Due to the lack of the above objective data and other issues, and the subjective evaluation data have a certain impact on the diagnostic results, our study only investigated the possible SD and analyzed its influencing factors, which may not show the overview of SD in China. Although there are these limitations, our research has focused on this field earlier in China, providing reference and assistance for future related research. More multicenter studies are needed in the future to validate, improve, and optimize SD diagnostic tools, establish SD diagnostic standards in China, and promote screening, diagnosis, and intervention of SD.