SAN DIEGO—The decision whether to resect and discard diminutive rectosigmoid polyps during colonoscopy or to leave them in place can be a tough one. Artificial intelligence–powered CADx can provide objective, real-time polyp characterization and potentially reduce unnecessary polypectomies, but large randomized controlled trials on this issue have been scarce. Two randomized studies presented at DDW 2025 found computer-aided diagnosis to be particularly useful in this setting.
Multicenter Chinese Study
A randomized multicenter study from China showed CADx was more accurate than manual optical diagnosis (OD) in distinguishing diminutive neoplastic lesions from hyperplastic ones in the rectosigmoid colon, although the two approaches were comparable for all polyps (abstract 215). In addition, Italian investigators found that a “leave-in-situ” (LIS) strategy adopted by CADx-assisted endoscopists was noninferior to a “resect-all-polyps” (RA) strategy with respect to adenoma detection rate (ADR), the primary end point, and this approach reduced polypectomies by at least 50% (abstract 361).
Thomas Y.T. Lam, PhD, RN, an assistant professor at the Nethersole School of Nursing at The Chinese University of Hong Kong, led a study conducted at four endoscopy centers in Changchun, Hong Kong, Nanjing and Shenzhen of adults with at least one polyp detected (abstract 215). Patients were randomized to undergo another colonoscopy with a deep convolutional neural network–based CADx system (Eagle Eye, Xiamen Innovision) or colonoscopy with manual OD using high-definition endoscopy systems and colonoscopes, performed by expert (=2,000 colonoscopies) or nonexpert endoscopists with some online training on the use of CADx.
The CADx system characterized the polyps as non-neoplastic, adenoma or invasive tumor with the endoscopic image enhancement mode turned on, for example, using narrow band imaging without magnification. In the OD group, the endoscopists conducted manual OD without magnification, but the narrow band imaging mode could be activated once a polyp was detected. A high or low level of confidence of the assessment was recorded. All polyps were removed and analyzed, and those with indeterminate histology or missed specimen were excluded.
The primary outcome was the accuracy of real-time recognition of neoplastic polyps by CADx versus OD using histology as the gold standard. Secondary outcomes included sensitivity, specificity, and positive and negative predictive values (PPV, NPV) of all polyps, NPV of diminutive rectosigmoid polyps, and agreement of the surveillance interval. They conducted subgroup analyses by experience of endoscopists and polyp size.
Endoscopists removed 1,889 polyps of all sizes from 1,090 patients; the demographic features, colonoscopy quality, colonoscopy findings and histologic diagnoses were comparable between the CADx and OD groups. After various exclusions, 911 polyps were analyzed in the CADx group and 978 in the OD group.
CADx Superior for Rectosigmoid Diminutive Polyps
In the primary analysis, the overall diagnostic performance was comparable between the groups. Both achieved an accuracy of about 85%, sensitivity of more than 90%, specificity of more than 70%, PPV of more than 80% and NPV of more than 85%. Including only the high-confidence diagnoses in the analysis, the number of polyps in the OD group decreased from 978 to 887 and the performance measures remained similar between the groups. There were also no significant differences according to endoscopist experience or polyp size.
However, Dr. Lam reported, for diminutive rectosigmoid polyps, CADx proved far superior to manual OD in differentiating neoplastic from non-neoplastic lesions (Table 1).
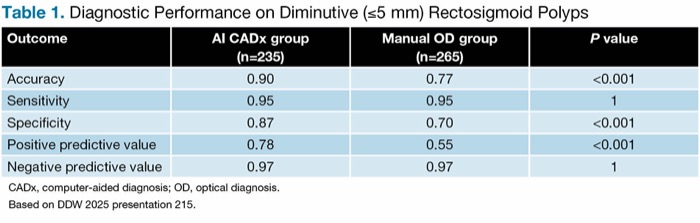
| Table 1. Diagnostic Performance on Diminutive (=5 mm) Rectosigmoid Polyps | |||
| Outcome | AI CADx group (n=235) |
Manual OD group (n=265) |
P value |
|---|---|---|---|
| Accuracy | 0.90 | 0.77 | <0.001 |
| Sensitivity | 0.95 | 0.95 | 1 |
| Specificity | 0.87 | 0.70 | <0.001 |
| Positive predictive value | 0.78 | 0.55 | <0.001 |
| Negative predictive value | 0.97 | 0.97 | 1 |
| CADx, computer-aided diagnosis; OD, optical diagnosis. Based on DDW 2025 presentation 215. | |||
He noted that for both groups, the NPV was 97%, which means that both exceeded the PIVI-2 (preservation and incorporation of valuable endoscopic innovations) threshold of at least 90% for determining whether a diminutive rectosigmoid polyp can be left in situ (Gastrointest Endosc 2011;73[3]:419-422). There also was comparability between the surveillance intervals predicted by polyp histology and those predicted by CADx (0.933) and OD (0.942), meeting the PIVI-1 threshold agreement of at least 90% for the resect-and-discard strategy, he said.
Multicenter Italian Study
The Italian multicenter study enrolled 895 patients undergoing computer-aided colonoscopy, both for detection (CADe) and OD (CADx), performed by average operators participating in organized colorectal cancer screening programs. Patients were randomized to one of two strategies: LIS, where diminutive (<5 mm) rectosigmoid polyps optically diagnosed as hyperplastic with the technologies at the endoscopist’s disposal (white light, blue light and AI) were left in place, or RA, where all detected polyps were resected.
The primary end point was noninferiority of the ADR in the LIS arm. There were several secondary outcomes, and results were based on intention-to-treat analyses.
Giulio Antonelli, MD, PhD, of Castelli Hospital, in Rome, who presented the findings, commented that the aim was to ensure that the adoption of an LIS strategy could be done “without leaving any adenomas behind.”
Dr. Antonelli reported that the primary end point was met in the whole colon and in the rectosigmoid tract (Table 2).
In addition, he said, “we saw a huge difference in the number of resected polyps: 622 with the LIS strategy and 1,289 with the resect-all strategy, with the mean number of polyps [per colonoscopy] nearly doubled in the resect-all arm (2.84 vs. 1.38).”
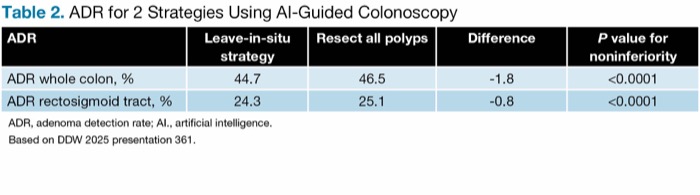
| Table 2. ADR for 2 Strategies Using AI-Guided Colonoscopy | ||||
| ADR | Leave-in-situ strategy | Resect all polyps | Difference | P value for noninferiority |
|---|---|---|---|---|
| ADR whole colon, % | 44.7 | 46.5 | -1.8 | <0.0001 |
| ADR rectosigmoid tract, % | 24.3 | 25.1 | -0.8 | <0.0001 |
| ADR, adenoma detection rate; AI., artificial intelligence. Based on DDW 2025 presentation 361. | ||||
LIS also was associated with improvements in other efficacy outcomes versus the RA group:
- mean number of unnecessary polypectomies per colonoscopy (based on histology): 0.28 versus 1.21, a reduction of 77%;
- PPVs (reflecting resection of clinically relevant lesions): 25.1% versus 13.6%; and
- true histology rates (reflecting resection of adenomatous lesions): 75.5% versus 18.6%
“Our study is the first randomized controlled trial of cost-saving strategies based on optical diagnosis in colonoscopy. We show data supporting the safety and effectiveness of a leave-in-situ strategy when using real-time CADe/CADx assistance by showing a reduction of approximately 50% of unnecessary polypectomies without a loss in terms of ADR,” Dr. Antonelli commented.
Studies Address Rising Concerns
Michael B. Wallace, MD, MPH, the John C. Andersen Professor of Medicine in the Division of Gastroenterology and Hepatology at Mayo Clinic in Florida, Jacksonville, told Gastroenterology & Endoscopy News that the studies are “valuable additions to the literature” and address one of the “rising concerns” about CADe systems, which have “clearly been demonstrated to increase adenoma detection but primarily through increased detection of small [and] diminutive low-risk polyps.”
The identification and removal of all adenomas are clearly associated with a reduced risk for subsequent CRC and death, although it increases procedural cost, Dr. Wallace noted. One potential solution would be to accurately distinguish between premalignant adenomas and diminutive hyperplastic polyps with little to no malignant potential. “This has always been challenging with standard endoscopic techniques, although in expert hands, can be done very accurately,” he said.
“In the Chinese study, … the computer-aided diagnosis software was very accurate at distinguishing benign hyperplastic from adenomatous polyps in the rectosigmoid, which are the ones that are most safely left behind when a confident diagnosis can be made. This reduces the burden, cost and risk associated with removal of polyps that have no malignant potential,” he noted.
“In the Italian study, … similarly … using an optical diagnosis with computer-aided systems to avoid removal of diminutive rectosigmoid hyperplastic polyps resulted in a substantial reduction in the overall burden of polyp removal without reducing ADR. This suggests that the strategy is safe and effective and does not reduce the overall detection of premalignant adenomas, although the use of the ADR measure is a weakness of the study,” he said.
Dr. Wallace maintained that a primary outcome of adenomas per colonoscopy, which counts each adenoma that is removed, would be preferable.
Dr. Antonelli responded that while he did not report adenomas per colonoscopy in his presentation, the analysis found that CADx improved that outcome as well.
—Caroline Helwick
Dr. Antonelli reported financial relationships with Alfasigma, Cosmo IMD, Medtronic, Odin Vision and Olympus. Dr. Lam reported no relevant financial disclosures. Dr. Wallace reported financial relationships with Boston Scientific, CDX Diagnostics, ClearNote Health, Cosmo, Digma Medical, Endiatx, Endostart, Fujifilm, Medtronic, Ohealio, Surgical Automations, Venn Biosciences and Virgo.
This article is from the July 2025 print issue.