Robotic colorectal, upper gastrointestinal, and general surgery using the CMR Surgical Versius robotic system was introduced at WHTH in July 2022. All consultant trainers underwent robotic training via the ‘Train the Trainer’ pathway provided by CMR Surgical [12]. This programme, together with the wider CMR Surgical educational platform, has been accredited by the Royal College of Surgeons of England [13]. Once consultants had completed their learning curve with the Versius system, they were approved to train surgical trainees.
A structured pilot programme was subsequently developed to train specialist trainees (ST4–ST8) in robotic console surgery using Versius. Trainees who previously would have been trained laparoscopically were now enrolled into this pilot scheme. Trainees self-nominated for participation based on a stated interest in robotic surgery and were selected from the existing general surgery rotation at WHTH. All had no prior robotic console experience and were scheduled to rotate through WHTH, ensuring compatibility with their standard clinical duties.
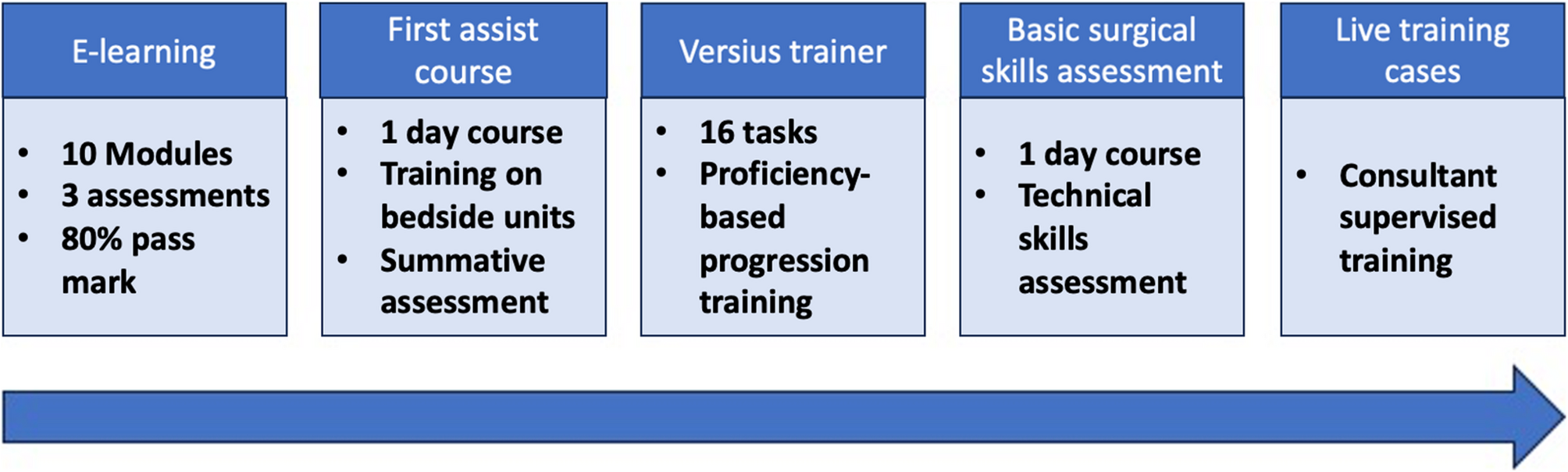
The training programme incorporated the validated consultant proctorship pathway and included sequential steps: online didactic modules, a first-assist course, performance-tracked virtual simulation exercises using the Versius Trainer, basic surgical skills assessment, and supervised training in live operating lists (Fig. 1). Progression through the pathway was contingent on meeting defined benchmarks at each stage, using objective performance metrics. Consultant trainers employed training principles similar to laparoscopic instruction, supplemented by metrics such as overall surgical time, active console time, and volumetric hand motion data to guide mentoring (Fig. 2).
Components of the robotic training programme for trainees

Examples of feedback data from robotic surgery using Versius
Trainees did not receive dedicated time off from service for training. Instead, the programme was embedded into their clinical schedule, with specific course days approved by the rota coordinator and educational supervisor as study leave. E-learning and simulation components were designed to be self-directed and completed during protected time or when clinical duties allowed, ensuring service provision remained unaffected while supporting skill acquisition.
Training pathway
Step 1: E-learning modules
Trainees had to complete 10 e-learning modules with 3 additional assessment modules and a score of 80% was essential to pass the modules. A list of the modules and assessments is outlined in Table 1.
Step 2: first assist course
Trainers from the CMR Surgical professional educational team held a one-day in-person training course for participating trainees. This taught them how to set up Versius as a team, drape the bedside units aseptically, respond appropriately to various alarms and safety features, provide bedside assistance, and clean the equipment. Following this, there was a summative assessment that candidates completed to ensure learning objectives had been achieved.
Step 3: versius trainer
The training on the Versius trainer consists of 16 tasks and is proficiency-based (Table 2). Each task has measurable metrics such as the combined instrument tip path length to reaching the object, combined instrument angular path and combined instruments out of view. The performance in each of these metrics is given a score, these performance scores are compared with benchmarks set to the average performance of experts completing the training tasks [14].
Step 4: basic surgical skills assessment
The basic surgical skills assessment was an in-person dry box session in the laboratory using synthetic models shown in Fig. 3. The aim of this was to develop trainees’ orientation and performance-based metrics. Trainees undertook technical skills-based assignments following a video demonstration and received supervisor feedback during and after the task. The tasks were designed to test the robotic system’s full range of motion and capabilities. These covered 9 types of dissection, suturing, knot-tying and a 360-degree anastomosis. Candidates were scored from analysis of technique and event errors and had unlimited attempts to pass the assessment.
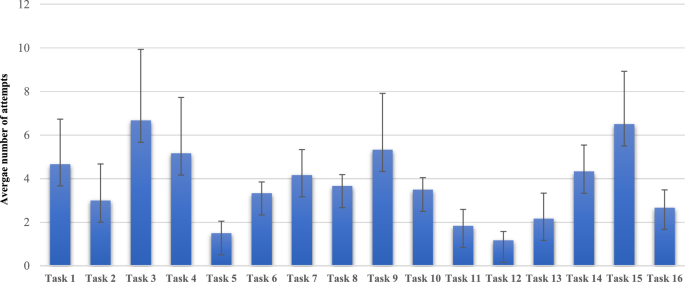
Graph to show the average number of attempts to complete the Versius Trainer tasks
Step 5: live training cases
Trainees subsequently participated in supervised training sessions under the direct guidance of consultant trainers, who provided real-time oversight during robotic procedures. Each operation was deconstructed into key procedural steps, allowing trainees to focus on mastering individual components before progressing to full procedural integration. For instance, anterior resections were taught using a modular approach based on established laparoscopic training frameworks. This included medial-to-lateral dissection, vascular control (ligation of the inferior mesenteric artery and vein), lateral mobilisation of the sigmoid colon, and total mesorectal excision. These structured steps were adapted from conventional laparoscopic paradigms and incorporated into the robotic training curriculum to facilitate progressive and systematic skill development. The modular format also allowed case segmentation based on the trainee’s competence level, ensuring patient safety during early robotic experience. This immersive, structured training approach enabled trainees to safely and effectively develop proficiency as robotic console surgeons [15].
At the end of the course, the trainees completed participation feedback forms, one for the first assist course and another for the basic surgical skills assessment. The questionnaire used was obtained online via the Royal College of Surgeons (RCS) website [16]. This was an RCS-developed questionnaire with the items in the questionnaire reflecting the College’s Education Standards.
Statistical analysis
One-way analysis of variance (ANOVA) was used to assess differences between tasks and trainees on the Versius Trainer. Data were analysed using IBM SPSS Statistics (Version 29).