Insecticide resistance reflects adaptive evolutionary dynamics, where selective pressure favors the survival and proliferation of resistant genotypes, where sensitive individuals are gradually eliminated under the continuous action of…
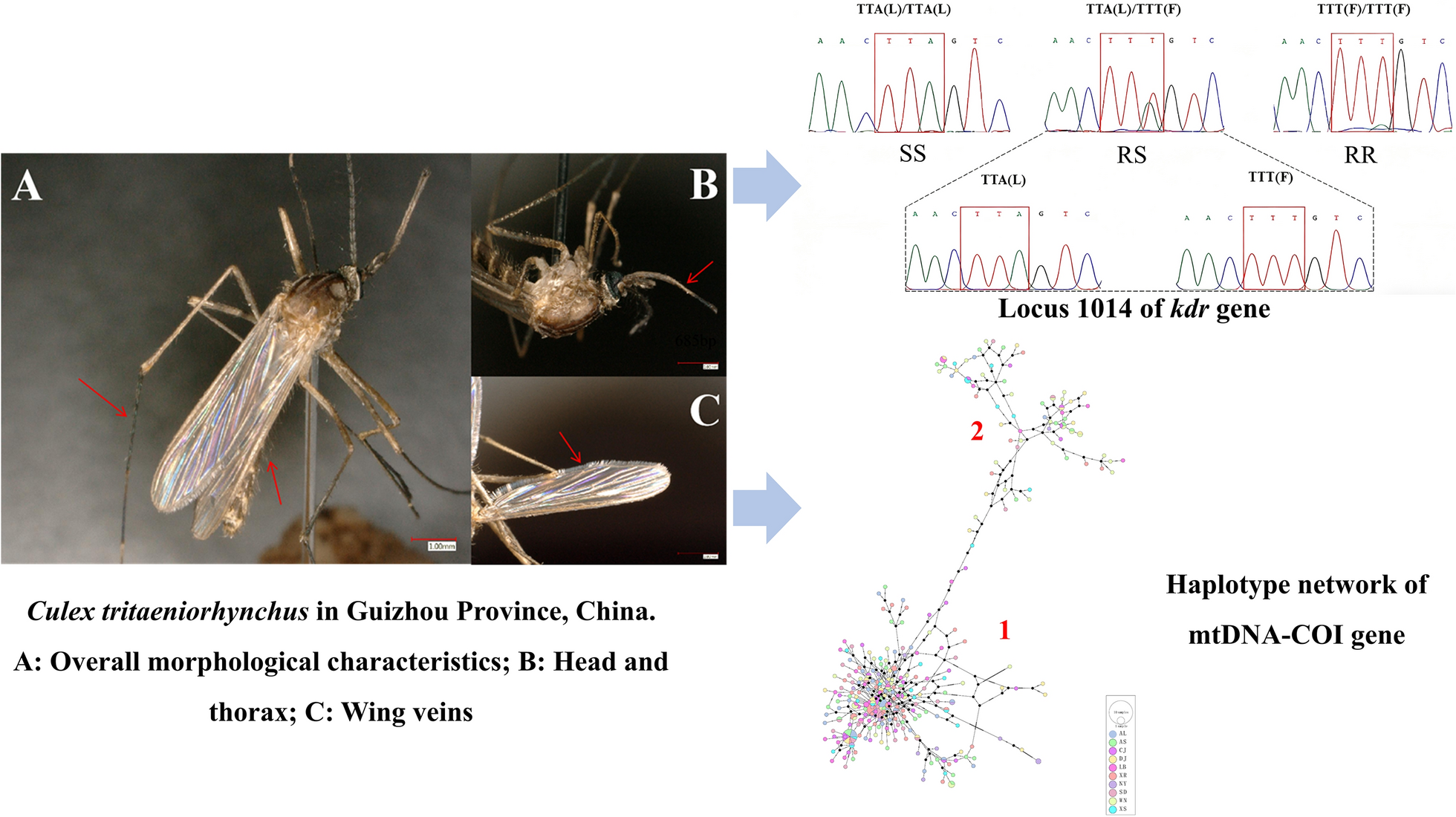
Mutation in the knockdown resistance gene and population genetic structure in Culex tritaeniorhynchus from Guizhou Province | Parasites & Vectors