Patient A
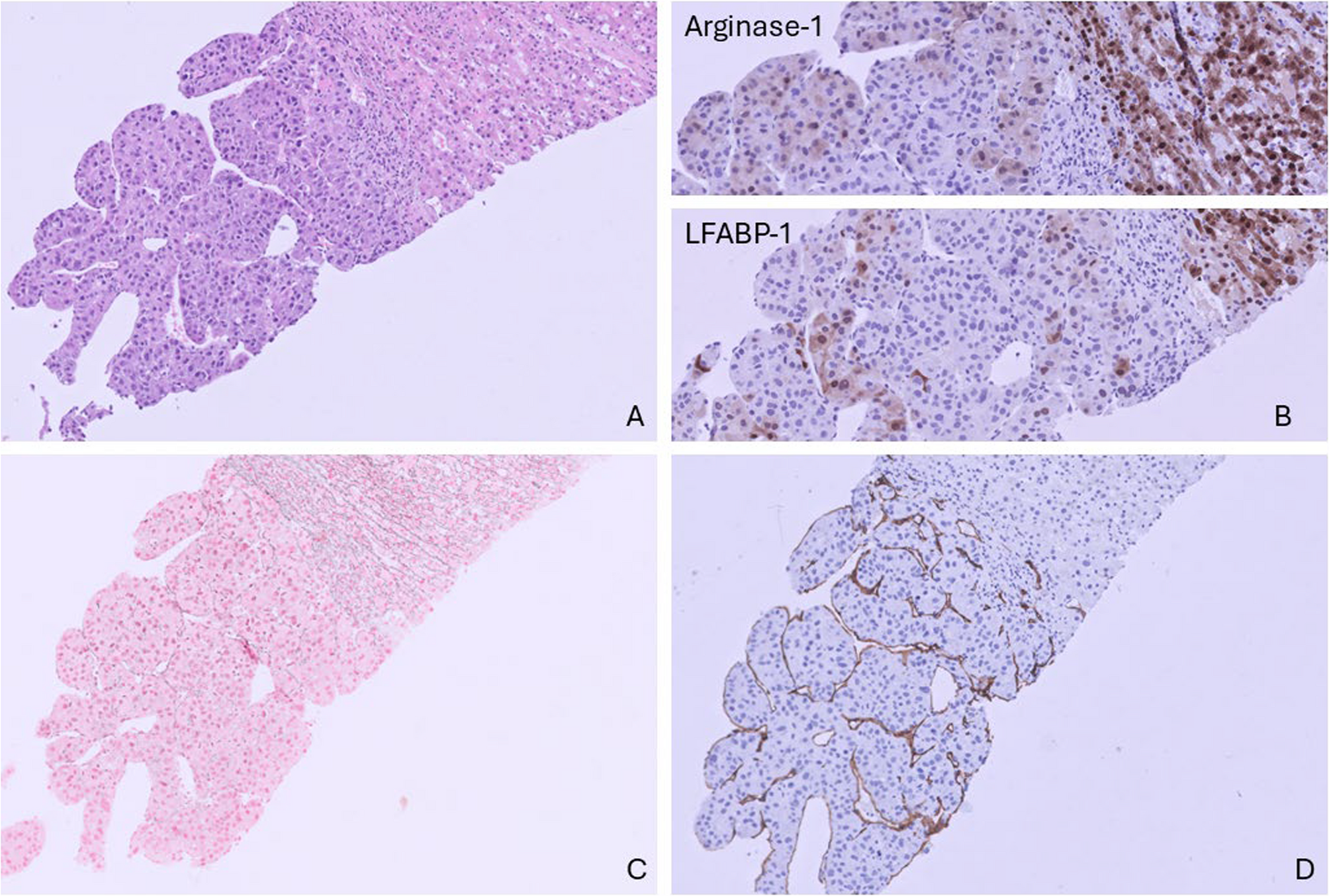
The first patient, an 82-year-old male, was referred to our hospital for the treatment of a solitary liver tumor. He was transferred from another hospital where he was analyzed for abdominal pain and weight loss. Ultrasound revealed a large tumor in the right lobe of the liver. The serum level of alpha-fetoprotein (AFP) was elevated; 59 µg/L. Magnetic resonance imaging (MRI) demonstrated a tumor of 10 cm in diameter in liver segments 5, 7 and 8. There was no history of excessive alcohol intake. Screening blood tests for causal factors of HCC, including hepatitis B and C, were negative. Because of inconclusive imaging results, a histologic biopsy was taken and demonstrated a moderately differentiated hepatocellular carcinoma in a noncirrhotic background (Fig. 1). The tumor had a trabecular growth pattern and comprised of cells with enlarged nuclei with multiple mitotic figures. Hepatocellular origin was further supported by variable cytoplasmic and nuclear expression of Arginase-1 and LFABP-1 (Fig. 1b). The tumor cells were Keratin 18 positive. A canalicular pattern was seen by poly CEA immunohistochemistry. BerEp-4, Keratin 7, 19 and 20 were all negative by additional examination (not shown). Gomori’s silver stain confirmed loss and fragmentation of reticuline fibers (Fig. 1c). The present capillarization of sinusoids was confirmed by CD34 (Fig. 1d).
Liver biopsy showing a moderately differentiated hepatocellular carcinoma in a noncirrhotic background. Standard HE staining, 20X magnification (a). Variable cytoplasmic and nuclear positivity of Arginase-1 and LFABP-1 in the tumor cells (b). Gomori’s silver stain showing fragmentation and loss of the reticuline network (c). Diffuse capillarization of sinusoids confirmed by CD34 stain (d)
The patient refused extensive surgical resection and declined palliative systemic therapy for HCC. To reduce his abdominal complaints, he started using cannabis oil shortly after his diagnosis. The cannabis oil was obtained via an unknown online supplier and the product label stated the oil contained 10% delta-9-tetrahydrocannabinol (THC) and 5% cannabidiol (CBD). He did not experience any side effects using two droplets sublingually three times daily.
Although the patient was sent to the general practitioner for best supportive care after his diagnosis, he was readmitted for oncological follow-up. At this first follow-up after 6 months using the cannabis oil, his abdominal complaints had resolved, and AFP levels were normalized to 2 µg/L. MRI demonstrated regression of the tumor to a size of 5.1 cm. The patient continued the use of cannabis oil, and the tumor continued reducing in size. Approximately two years after the diagnosis, the tumor was undetectable on MRI (Fig. 2A-C). Until today, almost 8 years after diagnosis, the tumor has not been detected again on imaging studies and AFP levels have remained normal.

Contrast-enhanced magnetic resonance (MR) images of an 82-year-old patient with advanced HCC (a) at diagnosis (b) at 6-month follow-up after using cannabis oil (c) at 6 years after diagnosis. Contrast-enhanced computed tomography (CT) images of a 77-year-old patient with advanced HCC (d) at diagnosis (e) at 6-month follow-up after using cannabis oil (f) at almost 4 years follow-up after using cannabis oil. N necrosis, t tumor
Patient B
The second patient, a 77-year-old male was referred to our hospital with undesired weight loss, a liver mass detected on ultrasound, and an AFP of 40,950 µg/L. He had a history of alcohol abuse. Screening blood tests for other causal factors of HCC, including hepatitis B and C, were negative. Computed tomography (CT) studies demonstrated a large tumor of 15.6 cm with central necrosis in liver segments 6, 7 and 8. A second lesion of 2.5 cm was located in segment 5. HCC was diagnosed based on typical imaging characteristics (arterial enhancement with wash-out in the late phase) combined with highly elevated levels of AFP and des-gamma carboxyprothrombin (22,142 AU/L) (Forner et al. 2018). Both tumors were deemed unresectable and the patient refused palliative treatment options for HCC, including selective internal radiotherapy (SIRT). In order to improve appetite and gain weight, he started to use cannabis oil upon diagnosis. The cannabis oil was obtained via an unknown online supplier and the product label stated the oil contained 15% THC and 2% CBD. He did not experience any side effects using 5 droplets sublingually two times daily.
After 3 months using cannabis oil, his clinical condition had improved, and he had gained weight. Upon imaging, the tumors had reduced in size from 15.6 to 9.2 cm in diameter and 2.5 to 1.9 cm, respectively. Afterwards, he continued to use cannabis oil and approximately 15 months after diagnosis the AFP had normalized to 2 µg/L. On CT, no vital tumor tissue was visible anymore, only rest necrosis (Fig. 2D-F). To this day, almost 5 years after diagnosis, imaging studies do not demonstrate any recurrent disease and AFP levels are normal.
In both patients, no significant dietary, lifestyle or other supportive interventions were initiated during the follow-up period aside from the reported use of cannabis oil. Neither patient had a history of recreational or medical cannabis use, nor of other cannabis-related substances, prior to their cancer diagnosis. Although both patients reported no adverse effects, systematic adverse event monitoring was not performed.