This study’s results showed that prehospital IBP measurement in critically ill patients is feasible even for teams with limited exposure to critically ill patients in a wide range of emergency indications. The frequency of complications associated with the puncture appears to be negligible. Cardiovascular failure and the need for airway management with catecholamine administration were the most common reasons for arterial cannulation. Here in particular, pronounced hypotension is to be expected, which has fatal consequences and requires continuous monitoring of blood pressure and therapy [16].
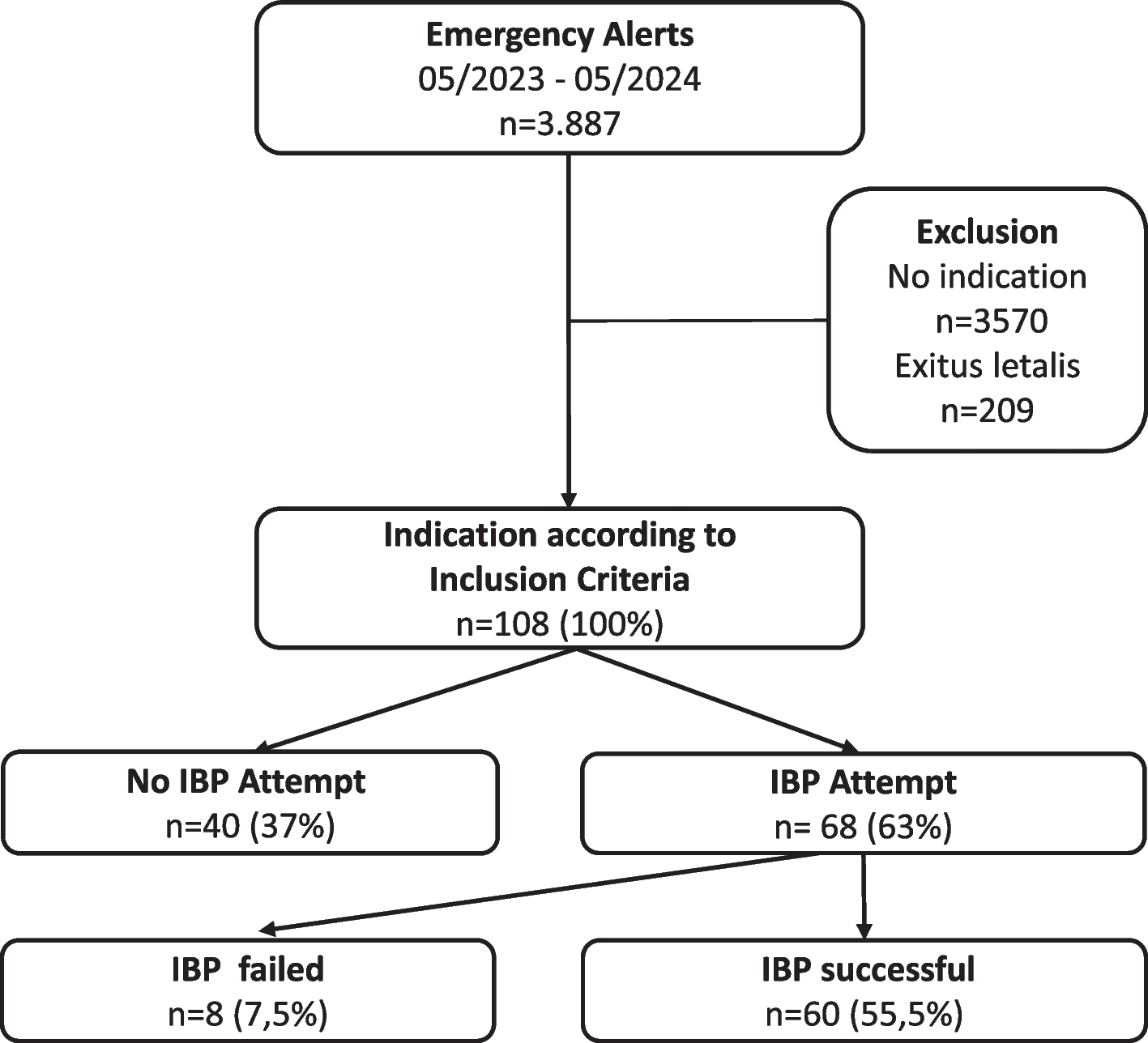
Overall, the frequency of prehospital arterial puncture in our patients was very low: an indication for invasive blood pressure measurement was only given in every 35th emergency call. Strict IBP criteria confronted a broadly dispatched emergency physicians by the German indication catalog for emergency medical services 2023 [15]. This low-threshold dispatch model for emergency physicians is controversial and contributes to a lack of routine in managing critically ill patients. That could be a reason why arterial punctures were not performed in about one third of the emergencies in which IBP measurement was indicated.
Since the high non-IBP attempt rates were not attributable to years of work experience and we are investigating a new procedure, the rarity of the indication may have an influence on the attempt rates. IBP attempts were often forgotten due to their rarity. Since Butterfield et al. reported an increase in IBP rate over time as teams have become more familiar with the technique [13], lack of routine and high rates of decision against IBP might only be temporally. Motivation to perform the IBP may also have influenced the low IBP rates: two physicians accounted for 13 unattempted punctures, representing one-third of all missed puncture opportunities.
In nursing homes, we had a significantly lower rate of IBP attempts, but we saw no difference in age distribution between the groups. Beside that elderly trauma patients are under-triage [17], this result might be due to the judged futility.
The selected IBP procedure depended on the experience of the team members. The advantage of direct puncture is possibly the time advantage, since we do not use sterile gloves and covers. The Seldinger technique offers the advantage of easier puncture with the disadvantage of longer preparation, a sterile approach and requires adequate skills. It is widely accepted, that direct puncture is more demanding and associated with higher failure rate [18]. In opposite to the literature, our prehospital data showed a higher failure rate in the Seldinger technique. Because emergency physicians could freely select the puncture method, a selection bias is likely: in cases with poor vascular access and anticipated difficulties, they tended to choose the Seldinger technique, which may explain its higher failure rate. Nevertheless, the overall rate of failure rate was low and comparable to other studies [11, 12]. Our data showed that, despite this new procedure, the focus remained on life-saving measures and that teams with limited exposure to critically ill patients also discontinue the effort according to protocol. As outlined in the protocol, during the initial two months, the arterial pressure system was prepared every morning by the crew to reduce the procedure time. After considering the ecological aspects of not using the system 8 out of 10 times, we switched to the strategy of preparing the system on-scene. Assembling the IBP system gives team members with limited prior exposure a valuable opportunity to familiarize themselves with its components. In EMS systems that encounter critically ill patients more frequently, the preparation at the beginning of the shift with 24 h shelf life can reduce on scene time.
The IBP measurement results in an average time delay of about 7.5 min. The time delay is significant even when adjusting all tested confounders. It remains unclear whether the calculated delay is due to puncture attempts, or due to unmeasured confounders: our IBP times are not measured but calculated on the difference in total on-scene time (difference between documented arrival time at the patient’s site and departure time to the target clinic). Measured times suggest that the IBP alone are unlikely to prolong the overall prehospital interval with a mean preparation time of 3 min and cannulation time of 2 min [12]. Further studies must show whether the time difference is also detectable in larger patient collectives and if the delay has a negative impact on outcome. In the study, it was up to the medical team to decide whether IBP had a positive impact on the outcome. For this reason, arterial puncture was often not performed due to the priority of transport and short transportation times.
It must be considered whether this time advantage outweighs the potential risk of hypotension. Every provider should be aware that non-invasive blood pressure measurement has a low accuracy in hypotensive patients, especially in the prehospital settings [6, 7]. IBP measurement can be advantageous if correctly indicated, even if time plays a decisive role. Even a time delay of 7.4 min may not affect the outcome of patients. Of course, this must be considered on an individual basis, and more measures could be detrimental to trauma patients [19]. In our study polytrauma patients most frequently had leading TBI symptoms. In patients with severe TBI, prehospital hypotension has a negative effect on mortality, but time on scene does not [20] and the time to CT with prehospital IBP and intrahospital IBP were equivalent [21]. These findings are likewise reproducible in intubated patients presenting with suspected stroke [22]. It remains to be seen whether IBP measurement reduces the cumulative time with hypotension to hospital admission and whether it affects the outcome.
In our opinion, the advantages of prehospital IBP measurement in critically ill patients are the direct monitoring of fluid or catecholamine therapy, the visibility of the effects of malignant cardiac arrhythmia on blood pressure and aiding in decision-making. A synergistic combination with prehospital blood-gas analysis could unlock additional therapeutic options. We recommend preclinical arterial puncture in critically ill patients who require airway management or when severe hypotension with volume or catecholamine administration is expected. A therapeutic consequence should always be present and the focus of the measure, as a time delay must be expected. Arterial puncture during CPR should only be performed once all essential advanced life support interventions have been initiated. We emphasize that teams must be familiar with material and technique, because otherwise a high inhibition threshold will often prevent arterial punctures despite indication.