Aim
To understand the association between personality traits, SE, and SM in women with GDM and test whether social support mediates this relationship based on the social cognitive theory.
Design and setting
In this multicentre cross-sectional study, both on-site and online investigations were conducted between 22 February and 28 November 2023. Initially, trained investigators explained the purpose, significance, and survey guidelines on-site. Subsequently, quick response codes linking to the online questionnaire were distributed for participants to fill out via the social media platform WeChat. To prevent duplication, each IP address was permitted a single entry. No time constraint was imposed for questionnaire completion, but all sections were required to be filled out prior to submission. On-site investigators then verified the completeness of each questionnaire and acknowledged participants’ contributions. Midway through the questionnaire, we inserted a question asking, ‘Did you provide truthful answers?’ Responses indicating ‘no’ were excluded during data cleaning.
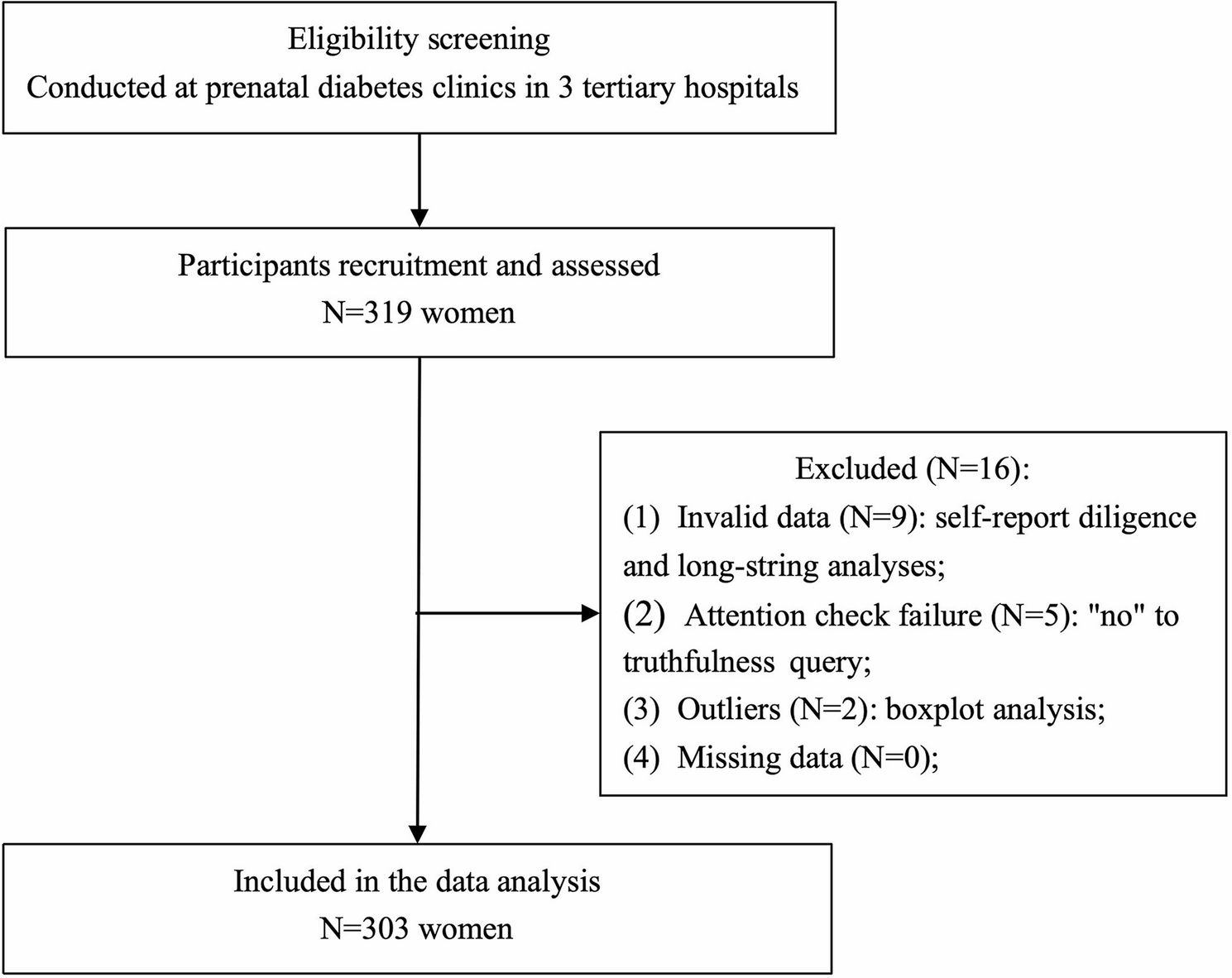
Participants were recruited through convenience sampling at three tertiary maternity hospitals in Fujian province, southeast China. These hospitals recorded more than 10,000 births in 2023, and recruitment was conducted via prenatal diabetes outpatient clinics. This study was approved by the Provincial Maternity and Child Health Hospital Ethics Committee (No. 2022YJ073; December 20, 2022). The study protocol complied with the Declaration of Helsinki. Data were collected anonymously and used solely only for research purposes. Participants received an invitation letter at the beginning of the questionnaire and were informed that they could withdraw at any time. Participants clicking ‘Agree, Next’ indicate their agreement to participate. Questionnaire quality was ensured through self-report diligence and long-string analyses to exclude invalid submissions. Figure 1 summarizes the participant recruitment process.
The participant recruitment process
Participants
Inclusion criteria were as follows: (1) adults aged 18 years or older; (2) diagnosed with GDM through a 75 g oral glucose tolerance test where at least one of the following thresholds was met: fasting blood glucose ≥ 92 mg/dL, 1 h blood glucose ≥ 180 mg/dL, 2 h blood glucose ≥ 153 mg/dL [30]; (3) full-term singleton pregnancy; and (4) cognitive ability to independently complete questionnaires. As a subset of women requires pharmacologic therapy when glycemic control cannot be maintained through lifestyle modifications [31], we excluded this group to avoid potential confounding by medication efficacy. Similarly, individuals with other pregnancy-related complications or comorbidities were excluded to ensure clarity of results.
The sample size was calculated using two-sided confidence intervals for one proportion using the PASS 2021 Sample Size Software for Windows, based on a good SM rate of 25.69% in Chinese women with GDM [32]. A sample size of 313 was required to achieve reasonable estimates with a 95% confidence interval and a 10% margin of error.
Measures
Demographic characteristics
The participants’ demographic characteristics collected included age, education, employment status, place of residence, household income, method of medical payment, and pre-pregnancy body mass index (pre-pregnancy BMI, calculated by dividing a woman’s weight at conceptionin kilogram (kg) by the square of the height in meters [33], and was classified into four categories based on the Chinese criteria [34]: underweight [BMI < 18.5 kg/m2], healthy weight [18.5–23.9 kg/m2], overweight [24.0–27.9 kg/m2], and obesity [≥ 28.0 kg/m2]), planned conception (couples made conscious choices about the timing of conception through active planning and preparation), method of conception (specific ways to achieve pregnancy), parity (the number of offspring a woman has born), history of abortion (spontaneous miscar- riage, elective termination of pregnancy, or either), history of prematurity (born prior to 37 weeks’ gestation), and family history of diabetes(defined as diabetes in parents or siblings).
Chinese big five personality inventory brief version
The Chinese Big Five Personality Inventory (Brief Version) (CBF-PI-B) was designed to assess personality traits. Wang et al. [35] developed a simplified version of this scale, adapted from the NEO Personality Inventory [36]. It comprises 40 items rated on a Likert scale from 0 to 5, measuring five personality dimensions. Scoring higher on a dimension indicates that the respondent is more likely to exhibit that trait. It has demonstrated good validity and reliability with Cronbach’s alpha values above 0.75. Its internal consistency reliabilities range from 0.764 to 0.814, and test-retest reliabilities over ten weeks vary from 0.672 to 0.811. The CBF-PI-B has been widely utilised in various Chinese populations [37, 38].
General self-efficacy scale
The General Self-Efficacy Scale (GSES) measures an individual’s overall efficacy, reflecting self-confidence in facing setbacks or difficulties, and is one of the most widely used instruments. Developed by Schwarzer et al. in 1981 [39], this scale consists of 10 items, each rated on a four-point Likert scale. The higher the score, the stronger the self-confidence. The Cronbach’s alpha coefficients of the GSES in different countries range from 0.75 to 0.94, and the retest reliability ranges from 0.55 to 0.75 [39].
Self-management scale for Chinese gestational diabetes mellitus
The Self-management Scale for Chinese Gestational Diabetes Mellitus (SMS-GDM) developed by Zhang et al. [40] assesses the SM behaviour of patients with gestational diabetes. Traditional diabetes SM tools, which include oral hypoglycemic agents, smoking, and foot care, are less applicable to pregnant women with GDM. This instrument is the first Chinese version of a GDM self-management evaluation scale. It includes 32 forward-scored items, each rated from 1 to 5 points. It evaluates four dimensions: SM awareness, pregnancy SM, glycaemic SM, and resource utilisation. The standard score is calculated by dividing the raw total score by the highest possible score and multiplying it by 100. This scoring classifies SM levels into < 60 points for poor SM, 60–80 points for moderate SM, and > 80 points for good SM. It exhibits a Cronbach’s alpha coefficient of 0.939, Spearman-Brown coefficient of 0.780, test-retest reliability of 0.903, and content validity of 0.927.
Perceived social support scale
Developed by Zimet et al. in 1988 [41], the Perceived Social Support Scale (PSSS) comprises 12 items across three dimensions: family support, friend support, and support from a significant other. Using a seven-point Likert scale, the respondents were asked to rank the items according to their perceived social support, with higher scores indicating greater perceived support. This scale demonstrated good reliability with a Cronbach’s alpha of 0.87. This scale was found to be a reliable scale for pregnant women with GDM [42].
Data analysis
Data cleaning and statistical analysis were conducted using SPSS (version 25.0 for Windows; IBM Corp., Armonk, NY, USA). Descriptive statistics were utilised, with categorical variables reported as frequencies and percentages. The Shapiro-Wilk test assessed the normality of the distribution. Student’s t-test and a one-way analysis of variance were applied to analyse factors individually. A Spearman correlation analysis was used to examine the relationships between variables. Duplicate data and data with missing information were excluded. Outlier detection, facilitated by boxplot analysis, was employed to eliminate anomalous data interference.
A structural equation model (SEM) was constructed in AMOS (version 24.0 for Windows; IBM Corp., Armonk, NY, USA) to perform a path analysis of personality traits, social support, and SE influencing SM in GDM. Fit indices, including the chi-squared to degrees of freedom ratio (CMIN/DF) < 3, goodness-of-fit index (GFI) > 0.90, normed fit index (NFI) > 0.90, incremental fit index (IFI) > 0.90, comparative fit index (CFI) > 0.90, and the root mean square error of approximation (RMSEA) < 0.080, were examined to determine whether the assumed model fit the observed data. The Bias-Corrected Bootstrap method tested for mediating effects and repeated random sampling was used to draw 5000 bootstrap samples from the original dataset to form an approximate sampling distribution. A 95% confidence interval was used to assess the presence of a mediating effect. Statistical significance was set at P < 0.05.