Study design and participants
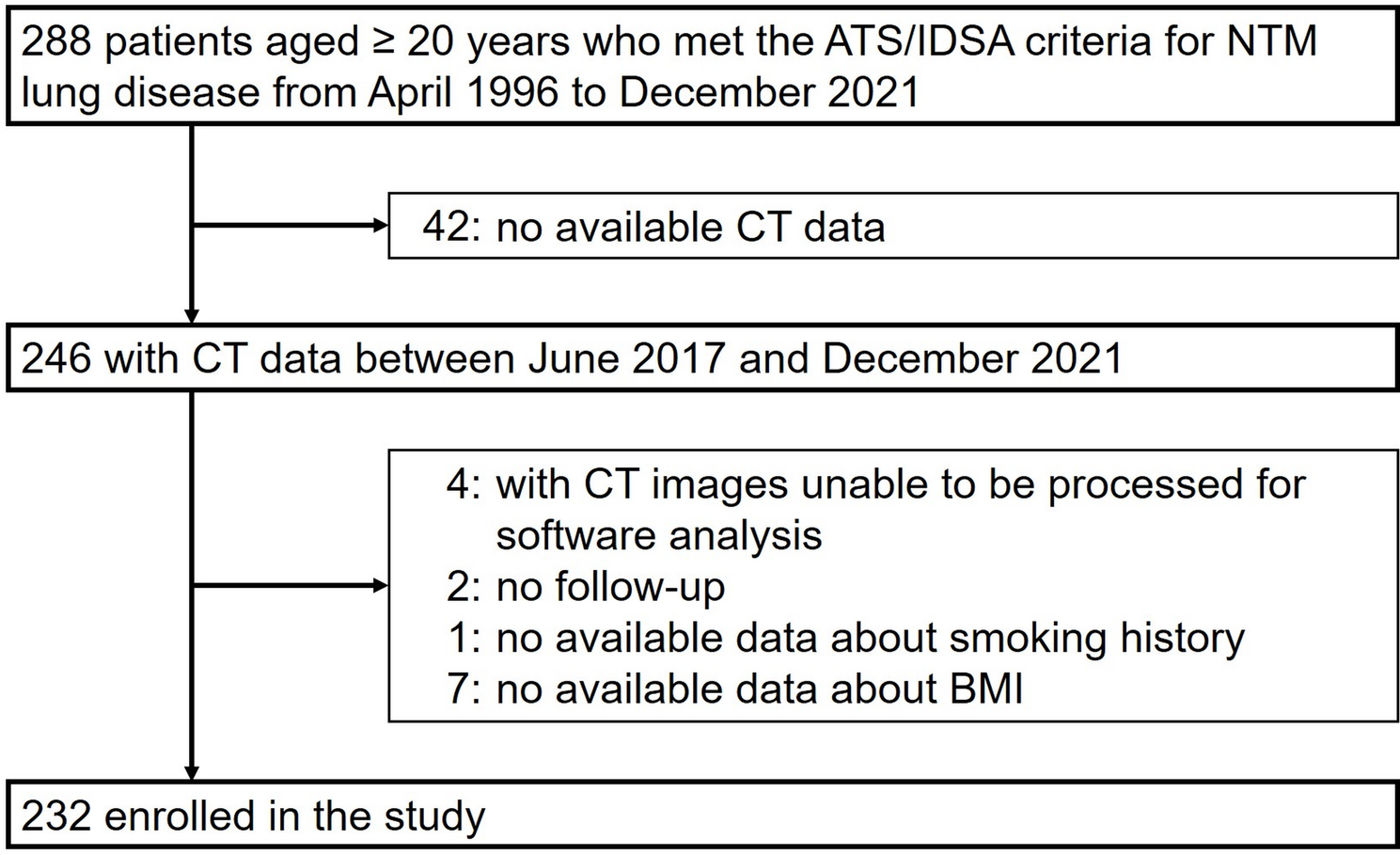
This study was conducted as a longitudinal cohort study through a retrospective review of medical records at NHO Fukuoka National Hospital. We reviewed 288 patients aged ≥ 20 years who met the American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA) diagnostic criteria for MAC lung disease between April 1, 1996, and December 31, 2021 [6]. Of these, we excluded 42 patients with no available data of chest computed tomography (CT) scans between June 1, 2017, and December 31, 2021, 4 patients whose CT image data were unable to be processed for the present analysis by the software, 2 patients without any follow-up medical records after the date of CT scanning, 1 patient with no information concerning smoking history, and 7 patients without body mass index (BMI) data. Hence, the remaining 232 subjects with MAC lung disease were enrolled in the present study (Fig. 1). When multiple CT scans were available during the 2017–2021 period, the earliest scan was used for analysis. The follow-up period was defined as the time from the CT scan to either July 2023 or a maximum of 5 years.
Quantitative CT image analysis
CT examinations were performed with a 160-slice multidetector CT scanner (Aquilion Lightning, Canon Medical Systems, Otawara, Japan) with a slice thickness of 5 mm. Quantitative CT image analyses were performed using dedicated software (AZE Virtual Place, Canon Medical Systems, Otawara, Japan) by a radiologic technologist without prior knowledge of the clinical data. For each patient, the lung field areas (LFAs) were evaluated separately in six domains using three axial CT slices in accordance with the Goddard score assessment protocols—the levels of the upper margin of the aortic arch (right and left upper lung field), the carina (right and left middle lung field), and 1–3 cm above the top of the diaphragm (right and left lower lung field) [13]. To identify the extent of cavitary destruction of the lung, the low-attenuation areas (LAAs) were defined as lung areas below − 950 Hounsfield units (HU), as in previous literature [14], and were also semiautomatically estimated using the same images (see Fig. S1 in Additional file 1) [15]. Mean values of LFA and LAA were calculated and used for the present analyses. The LFA/LAA ratio was computed for each of the six lung fields, and the average of these six values was used in the analysis. When dividing the study subjects into three groups based on the tertile distribution of the mean LFA, the cutoff values were as follows: lowest, ≤ 69.54 cm2 (N = 78); middle, 69.55–85.59 cm2 (N = 77); and highest, ≥ 85.60 cm2 (N = 77). For validation analysis between the mean values of LFA and lung volume (LV), a total of 9 subjects were randomly selected in order to assess LV. LV was calculated with the following 3 steps: at first, the lung plus bronchus volume (LBV) was identified by extracting the area less than − 500 HU. Next, the bronchus volume (BV) was measured by extracting the area less than − 920 HU and by ensuring the continuity of connection to other bronchi. Lastly, the LV was calculated by subtracting the BV from the LBV.
Clinical evaluations
For each case, respiratory physicians reviewed the patient’s medical records and assessed the demographic and clinical characteristics: age, gender, height, weight, smoking history, medical history, and results of mycobacterial cultures. BMI (kg/m2) was calculated as weight divided by squared height. Smoking habit was dichotomized as never smokers and smokers, considering that smoking could have affected emphysematous changes of the lung, appearing as low-attenuation areas (< −950 HU). Antibiotic treatment for MAC disease was defined as the prescription of clarithromycin and/or rifampicin and/or ethambutol. MAC species were categorized into three groups: M. avium group, Mycobacterium intracellulare (M. intracellulare) group, and co-infection group (subjects with both M. avium and M. intracellulare detected).
Statistical analysis
R software version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used to perform all statistical analyses. A two-sided P < 0.05 was considered to indicate statistical significance. For baseline characteristics, the heterogeneity in each variable among the levels of mean LFA was evaluated using the analysis of variance (ANOVA), chi-square test, or Kruskal–Wallis test. Pearson’s correlation coefficient was calculated to assess the correlation between the mean values of LFA and those of LV. Kaplan–Meier curves were constructed to show the survival rate over the follow-up period. The unadjusted and multivariable-adjusted hazard ratios (HRs) with their 95% confidence intervals (95% CIs) according to the levels of mean LFA for all-cause mortality were estimated using a Cox proportional hazards model. Adjustments were made for age, gender, BMI, smoking history, MAC treatment, MAC species, co-infection with NTM other than MAC, and mean LAA, which has been reported as a potential prognostic factor in patients with NTM lung disease [16, 17]. Relevant models were used to evaluate the linear trends in the risk of all-cause death across the tertile classification of mean LFA. We evaluated the ability of mean LFA and mean LAA to predict mortality using receiver operating characteristic curves and estimated the area under the curve (AUC) for each. The AUCs were compared using the DeLong method. The robustness of the main results was tested through sensitivity analyses limiting the subjects to M. avium-positive or M. intracellulare-positive cases individually. Since smoking exposure can accelerate emphysematous change and increase the value of LAA in the lung, stratified analysis was performed by smoking status.
Ethical considerations
The study was approved by the NHO Fukuoka National Hospital Institutional Review Board for Clinical Research (#F5-34). For this study, informed consent has been waived by the NHO Fukuoka National Hospital Institutional Review Board due to the anonymity and retrospective nature of the study. This study was conducted according to the principles of the Declaration of Helsinki.