General characteristics of malignancy-PJP patients
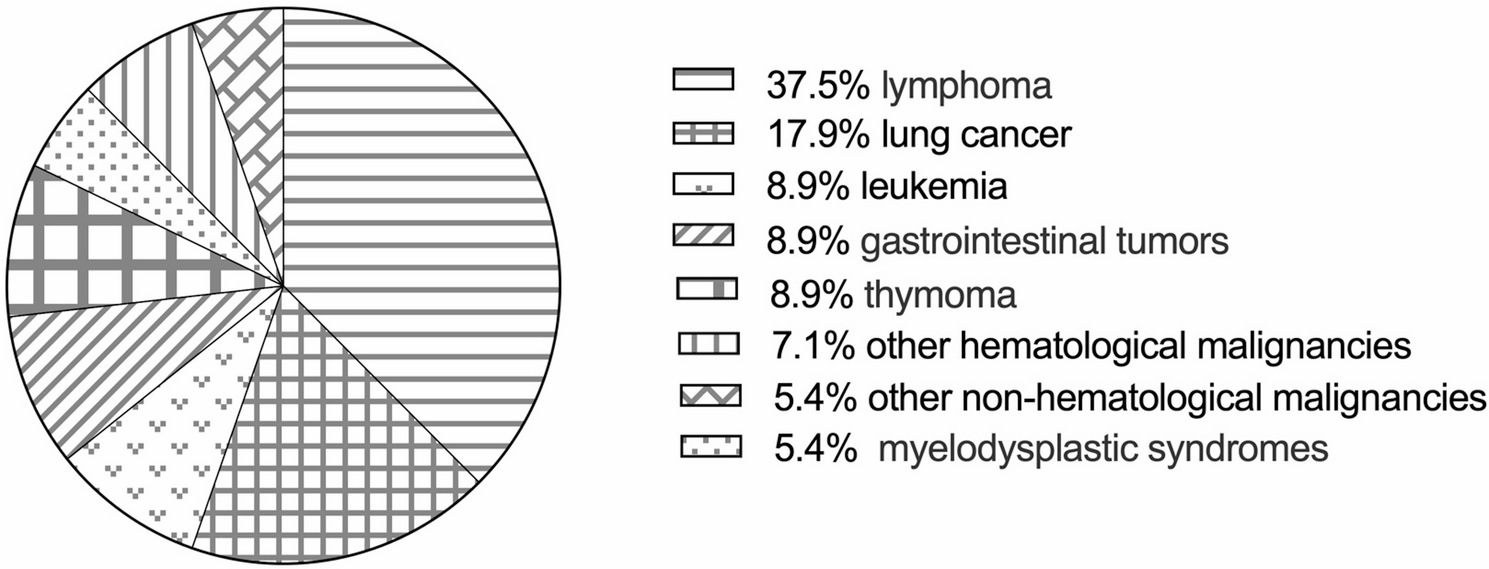
Fifty-six patients with an identified diagnosis of malignancy-PJP were enrolled in our study after a detailed medical record review. Thirty-four patients were male (60.7%), 22 patients were female (39.3%), and the mean age was 63 (52, 68) years. The underlying malignancies are shown in Fig. 1. Most patients had solid malignancies (45, 80.4%), and 11 (19.6%) had non-solid malignancies. According to the involved system, 23 (41.1%) patients had non-hematological malignancies, and 33 (58.9%) had hematological malignancies.
The underlying malignancies of enrolled 56 malignancy-PJP patients. Other hematological malignancies: multiple myeloma and aplastic anemia; other non-hematological malignancies: prostate cancer, nasopharyngeal cancer, and breast cancer
The main clinical manifestations of PJP were fever (52, 92.9%), cough (47, 83.9%), expectoration (41, 73.2%), and dyspnea (47, 83.9%). Bilateral (56, 100%), ground-glass opacities (GGOs) (48, 85.7%), and patches (45, 80.4%) were the most common chest CT manifestations. Consolidations (24, 42.9%), nodular (24, 42.9%), and pleural thickening (32, 57.1%) were observed on some chest CTs of patients with malignancy-PJP. Low peripheral CD4+ T-cell [125.0 (66.0, 207.0)/µL] counts were common in patients with malignancy-PJP.
Some patients were complicated with other infections, such as CMV (25, 44.6%), bacterial HAP (23, 41.1%), oral candida infection (6, 10.7%), aspergillus infection (6, 10.7%), and Nocardia infection (2, 3.6%). Most patients experienced respiratory failure (47, 83.9%), approximately half of the patients needed intensive care unit (ICU) support, and 29 patients (51.8%) died.
After PJP diagnosis, most patients (50, 89.3%) were prescribed 15 mg/kg/d trimethoprim-sulfamethoxazole (TMP-SMX). More than one-third of our patients (21, 37.5%) were also prescribed a combination of second-line anti-PJP medications, such as caspofungin, clindamycin and primaquine.
Differences in the clinical characteristics and prognosis between PJP patients with non-hematological and hematological malignancies
According to the involved system, the 56 patients were divided into a non-hematological malignancy group and a hematological malignancy group. The differences in clinical characteristics, laboratory test results (Table 1) and imaging findings (Table 2) between the two groups were analyzed.
There were no significant differences in age, sex or comorbidities between the two groups. Compared with patients in the non-hematological malignancy group, more patients in the hematological malignancy group needed invasive mechanical ventilation support (60.6% vs. 43.5%, p = 0.03). Patients in the hematological malignancy group were more prone to respiratory failure and higher mortality, but the difference was not statistically significant. The time from diagnosis of oncological disease to PJP infection [72 (38.0, 112.5) days vs. 153 (92.5, 223.5) days, p < 0.01] and the time from chemotherapy to PJP infection [79.0 (46.5, 415.5) days vs. 229.0 (116.0, 677.5) days, p = 0.04] were shorter in the hematological malignancy group than in the non-hematological malignancy group. In terms of chest CT features, pleural thickening was more common in the non-hematological malignancy group than in the hematological malignancy group (73.9% vs. 45.5%, p = 0.03). However, there were no significant differences in the minimal albumin level, peripheral lymphocyte count or inflammatory marker levels between the two groups.
Differences between the survival and non-survival groups of patients with malignancy-PJP
The 56 patients were divided into a survival group (27 patients) and a non-survival group (29 patients) according to their clinical outcome. Compared with those in the survival group, more patients in the non-survival group were complicated with CMV (62.1% vs. 25.9%, p < 0.01) and bacterial HAP (58.6% vs. 22.2%, p < 0.01). However, there were no significant differences in clinical symptoms, chest CT features, chemotherapy before PJP infection or anti-PJP treatment between the two groups.
In terms of laboratory test results, in the non-survival group, the peripheral lymphocyte count [0.4 (0.3, 0.7) × 109/L vs. 0.8 (0.5, 1.4) × 109/L, p < 0.01], platelet count [138.0 (74.0, 197.5) × 109/L vs. 212.0 (160.8, 265.3) × 109/L, p < 0.01], minimal albumin level [21.7 ± 5.3 g/L vs. 26.6 ± 4.6 g/L, p < 0.001], T-cell count [307.0 (151.0, 377.0)/µL vs. 447.0 (245.5, 920.5)/µL, p = 0.01) and CD4+ T-cell count [123.0 (37.0, 163.0)/µL vs. 146.0 (97.0, 417.0)/µL, p = 0.03] were significantly lower than those in the survival group. However, D-dimer [8.3 (2.0, 15.6) mg/L vs. 1.9 (0.9, 6.3) mg/L, p = 0.01], high-sensitivity C-reactive protein [107.0 (36.3, 191.3) mg/L vs. 42.2 (6.9, 87.0) mg/L, p < 0.01] and lactate dehydrogenase [588.0 (441.0, 789.5) U/L vs. 319.0 (255.0, 481.0) U/L, p < 0.01] levels were greater in the non-survival group than in the survival group.
Prognostic analysis for patients with malignancy-PJP
As shown in Table 3, univariate Cox regression analysis revealed that non-solid malignancies, decreased lymphocyte count, CMV viremia, bacterial HAP, and pneumomediastinum were associated with non-survival. Subsequent multivariate Cox regression analysis revealed that non-solid malignancies (HR = 2.77, χ2 = 4.83, p = 0.03, 95% CI: 1.12–6.89), CMV viremia (HR = 3.33, χ2 = 8.93, p < 0.01, 95% CI: 1.51–7.33), bacterial HAP (HR = 2.21, χ2 = 4.10, p = 0.04, 95% CI: 1.03–4.77) and pneumomediastinum (HR = 2.50, χ2 = 3.96, p < 0.05, 95% CI: 1.01–6.14) were independent risk factors associated with poor survival in patients with malignancy-PJP.
Kaplan‒Meier analysis (Fig. 2) was performed to explore the impact of the different types of underlying malignancies on the cumulative survival of malignancy-PJP patients. The results revealed that there was no significant difference in survival between patients with non-hematological malignancies and those with hematological malignancies. Compared with that of patients with solid malignancies, the survival rate of patients with non-solid malignancies (p < 0.05) was significantly lower.
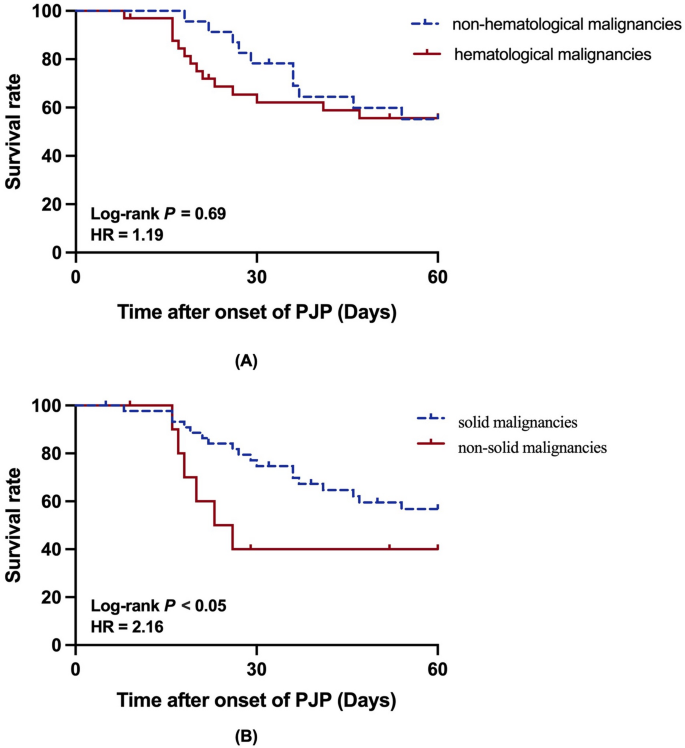
Kaplan-Meier analysis of malignancy-PJP patients on 60-day. A with hematological malignancies and with non-hematological malignancies; B with solid malignancies and with non-solid malignancies