The main findings of our study are the following: (1) in trans-femoral or trans-axillary TAVI procedures the main access percutaneous closure with ProGlide coupled with CBOT is possible and safe; (2) the unadjusted analysis suggests a possible association between the combined approach and a lower incidence of VARC-3 type ≥ 2 bleeding, RBC transfusions in the first post-procedural 72 h, and AKI; (3) the potential protection against VARC-3 type ≥ 2 bleeding of the combined approach was confirmed in the adjusted analysis; (4) the CBOT group displayed shorter time-to-discharge after TAVI.
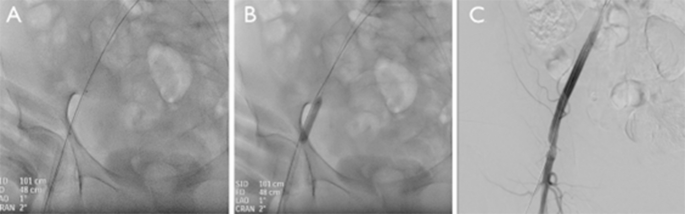
The study explores the use of CBOT as endoclamping technique in addition to ProGlide for the main arterial access closure after TAVI (Fig. 2). To the best of authors knowledge, this is the first real-world comparison of the CBOT performance vs. the standard closure using the ProGlide device.
The crossover balloon occlusion technique (CBOT), in which a balloon is placed in the external iliac artery, upstream of the main TAVI access site, over the 0.018” protection wire, assures complete hemostasis during sheath removal and access closure with the pre-implanted ProGlide. In this multicenter comparative study, 229 consecutive patients treated with TAVI were divided based on the main access closure strategy in two groups: the combined (CBOT + ProGlide) and the ProGlide suture only group. The CBOT + ProGlide treated group presented lower incidence of minor vascular complications, red blood cells transfusions, Valve Academic Research Consortium-3 (VARC-3) type ≥ 2 bleeding and acute kidney injury stages ≥ 2, and reduced LOS. Even after a propensity score matching, the combined approach was associated with fewer major bleedings (CI 0.04–0.99; OR 0.2; p = 0.05). Prospective, pragmatic, randomized trials would be valuable to possibly confirm the clinical benefit of this endoclamping technique.
We purposively restricted the analysis to patients admitted after September 2021 because TAVI represents a rapidly evolving field due to the quick improvement of operators’ expertise and of technological progresses. We thus focused on recent bioprosthetic devices with reduced sheath size and high deliverability; as a proof, most of the procedures were performed with 14 Fr devices which represent the best technology currently available10,23,24. However, even if a dramatic reduction in vascular complications and bleeding rates has been observed with newer generation devices25, to date the incidence of major bleeding during TAVI is still reported to be 4.3–11.3%, and its management remains difficult11,12,14,26. Major bleeding, major vascular complications, and transfusions unfavorably impact on patients’ short- and long-term clinical outcomes, including all-cause death11,12,13,15. In this study, the incidence of major vascular complications in the overall population was 0.9%, which confirms the high-level expertise of the two high volume enrolling centers. Minor vascular complications and RBC transfusions occurred in 4.8% and 9.2% of patients, respectively. Notably, although the two groups differed in the prosthetic valves used, the size of the delivery systems, which is a known predictor of vascular complications and bleeding27, was comparable between groups with slight advantage in terms of lower profile observed in the ProGlide treated population (supplementary Table 2).
Interestingly, in the present study most of the transfusions were unrelated to vascular complications (major vascular complications and VARC-3 type ≥ 2 bleeding were 0.9% and 7.4% respectively). As a consequence, the main advantage of CBOT seems to come from the complete occlusion of the artery during the access closure which provides a clean tightening of the pre-implanted ProGlides and an effective temporary hemostasis in cases of ProGlide failure, thus allowing the operator to safely deliver an additional closure device system. Moreover, routinary use of the endoclamping technique can favor the quick management of any complications occurring after the removal of the prosthetic delivery system. These advantages seem to result in reduced bleedings and fewer post-operative transfusions. Notably, the balloon inflation may also eventually reduce the arterial stenosis related to the ProGlide sutures.
Intraoperative bleeding is one of the most consistent contributing factors for AKI development28,29. In turn, a recent meta-analysis suggested that even AKI stage 1 negatively impacts on both the one year and three year survival rates after TAVI30. Yan-biao Liao et al. demonstrated that significant bleedings and number of RBC transfusions predict in a directly proportional manner the incidence of AKI and long term mortality, mainly due to structural and functional alterations in the preserved RBCs and the buildup of pro-inflammatory mediators31. Moreover, a 1.8-fold increased risk of AKI was also associated to anemia after TAVI32. In agreement with the above cited literature, the lower incidence of AKI in the CBOT treated population may reasonably occur as the result of less transfusions and major bleedings observed in this group.
However, because of the non-randomized nature of enrolment, our findings must be interpreted with caution. Purposively, PS matching was used to partly overcome disparities in the baseline clinical profile of the two patients’ groups. The adjusted analysis confirmed the protective role of CBOT against VARC-3 type > 2 bleeding and the correlation between this technique and lower mean hospitalization time. Moreover, a slight tendency to higher incidence of AKI was observed in the ProGlide group after PS-matching, mainly driven by stage 2 and 3 AKI.
Conclusively, these findings represent the first report on a relatively large population of a possible protective effect against bleeding of a routine endoclamping technique adjunctive to conventional sutures. On the other hand, this technique carries an increase in procedural time and costs due to the need for additional devices; future investigations will clarify if the hypothesized reduction in vascular complications and in consequent additional unplanned interventions may ultimately offset in terms of clinical and economic net benefit the above-mentioned drawbacks.
Some limitations of the present study should be acknowledged. Firstly, sample size, despite larger than previous reports, is in absolute terms small. Second, this was a non-randomized study and, even if PS-matching was used to adjusting for potential confounding variables, it was not able to correct for the unmeasured variables. Third, the choice of prostheses was left to the discretion of operators in each institution, and not all of the devices currently in use were included in this study. Finally, patients with severe PAD or significant tortuosity of the iliofemoral axes were excluded from the analysis; thus, the routine application of CBOT was not assessed in these cases.
Furthermore, despite the favorable interplay between novel devices and trans-axillary access, TAVI represents a challenging procedure requiring careful patient selection and management28. –29 As a result, our findings should be regarded only as hypotheses generating and would require and, to authors opinion, deserve further confirmation from a large randomized trial30.