ISLAMABAD (Dunya News) – Another 106 Pakistani citizens stranded in the Middle East have safely returned home through the Taftan border crossing from Iran on Thursday.
Following the Iran-Israel war, the process of…

ISLAMABAD (Dunya News) – Another 106 Pakistani citizens stranded in the Middle East have safely returned home through the Taftan border crossing from Iran on Thursday.
Following the Iran-Israel war, the process of…
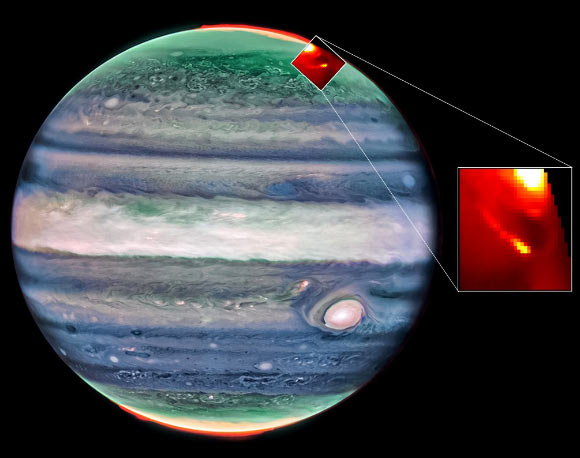
The NASA/ESA/CSA James Webb Space Telescope conducted a clockwise scan around the entire limb of Jupiter, chasing aurora as it rotated into view. This dynamic phenomenon is a result of charged particles traveling down magnetic field lines,…
Curiosity kick-started John Thyfault’s career in science, and it continues motivating him to make new discoveries.
Toward the end of his college football career at Fort Hays State University, Thyfault, Ph.D., hoped to become a strength and…