Amid Iran chaos, US treasury issues 30-day waiver to let Indian refiners buy Russian oil
One beneficiary of the chaos in the Persian Gulf appears to be Russia, since the US treasury secretary, Scott Bessent, just announced that the US has issued a…

One beneficiary of the chaos in the Persian Gulf appears to be Russia, since the US treasury secretary, Scott Bessent, just announced that the US has issued a…


The powerful Swampert is coming back into Pokémon Scarlet and Pokémon Violet 7-star Tera Raid Battles. The Mud Fish Pokémon will appear at black Tera Raid crystals from Friday, 6 March 2026, at 00:00 UTC to Thursday, 12 March 2026, at 23:59 UTC. The Swampert appearing during this event has Poison as its Tera Type. Be prepared—this Pokémon is a formidable foe, and it’s got the Mightiest Mark to prove it! Work together with your friends to topple this powerful Tera Pokémon!
Whenever you see a sparkling pillar of light shining from a Tera Raid crystal, you can walk up to the crystal and interact with it to start a Tera Raid Battle with a Tera Pokémon. To find the Tera Pokémon featured in this event, you’ll also need to have downloaded the latest Poké Portal News. To do so, follow these steps:
Select Poké Portal in the X menu.
Select Mystery Gift.
Select Check Poké Portal News.
To challenge Poison–Tera Type Swampert with the Mightiest Mark, Trainers will need to either complete the postgame events that follow the main story or join a 7-star Tera Raid Battle hosted by a Trainer who has completed those events. This special Swampert can be caught only once per save data. You can still participate in Tera Raid Battles against this Swampert if you’ve already caught it to obtain other rewards—including significant amounts of Exp. Candy for leveling up your Pokémon, treasures that can be sold at Pokémon Centers, items for improving your Pokémon’s stats, and Poison Tera Shards for changing your Pokémon’s Tera Type.
After you’ve caught this mighty Swampert, why not bring it home? Catch some of the cute Swampert merch that’s currently available on Pokémon Center!
Introduction
Key takeaways
What is IVF?
IVF and reproductive aging
IVF and timing of menopause
IVF and hormonal/biologic stress
IVF and cardiovascular risk
IVF and cancer risk
Psychological and quality-of-life outcomes
Research gaps and limitations

The ESA’s Mars Express probe has been surveying Mars from orbit for more than twenty years. The way it has mapped the surface using its High Resolution Stereo Camera (HRSC) has drastically changed the way we see the Red Planet. In a…

In the age of streaming slop designed to appeal to as many people mid-Instagram-scroll as possible, there’s something wonderful about a film that’s not afraid to embrace its specificity.
Producer Nastasya Popov’s directorial debut, Idiotka,…

ISLAMABAD (Dunya News) – Another 106 Pakistani citizens stranded in the Middle East have safely returned home through the Taftan border crossing from Iran on Thursday.
Following the Iran-Israel war, the process of…
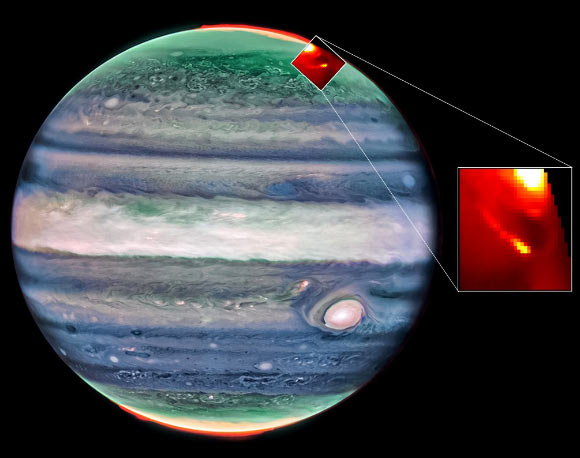
The NASA/ESA/CSA James Webb Space Telescope conducted a clockwise scan around the entire limb of Jupiter, chasing aurora as it rotated into view. This dynamic phenomenon is a result of charged particles traveling down magnetic field lines,…