- CM approves ‘Punjab Rehmat Card’ for widows, orphans Business Recorder
- Grant for widows, orphans approved The Express Tribune
- CM Maryam approves ‘Rehmat Card Scheme’ for widows, orphans Dunya News
- Punjab unveils Rahmat Card to support widows…
Author: admin
-
CM approves ‘Punjab Rehmat Card’ for widows, orphans – Business Recorder
-

Advancing Chile’s mining sector through sustainable water solutions
Located in the country’s Atacama Desert, Chile’s Antofagasta region is considered one of the world’s premier copper-producing hubs, but it faces a pressing challenge: freshwater scarcity.
This shortage affects both local communities and the continued growth of the mining industry.
As Antofagasta Minerals, a Chilean copper mining group, looked to expand its Centinela mining district, the need for a sustainable water solution that would preserve essential continental water resources without the need for desalination1 became paramount.
To address the challenge, Almar Water Solutions, a global water infrastructure developer, and Transelec, a leading provider of high-voltage systems in Chile, formed the Aguas Esperanza consortium. Together, they agreed to a $US1.5 billion critical water transportation system to support the expansion of Centinela.
This partnership included the acquisition and operation of an existing 144-kilometre seawater pipeline and the construction of a second pipeline of equal length, enabling the extraction of an additional 144,000 tonnes of copper, 3,500 tonnes of molybdenum, and 130,000 ounces of gold annually.1
At the heart of the project is an innovative approach: transporting more than 1,100 litres of seawater per second from the Pacific coast to the mine site.1 By using seawater instead of scarce inland supplies, the project safeguards local aquifers and sets a new standard for environmentally responsible mining. It also advances Antofagasta’s commitment to source 90 per cent of its mining division’s water from seawater, recycled or reused sources by 2025,2 helping secure the region’s future and promote sustainable growth.
Continue Reading
-
PMD predicts dry weather in most parts of country – RADIO PAKISTAN
- PMD predicts dry weather in most parts of country RADIO PAKISTAN
- Rain and Thunderstorms Predicted Across Pakistan ProPakistani
- Dry weather expected across most parts of Pakistan: Met Office Business Recorder
- When March begins to feel like…
Continue Reading
-

Trial aims to improve family communication about inherited colorectal cancer risk
In time for Colorectal Cancer Awareness Month in March, the Alliance for Clinical Trials in Oncology has launched a new clinical study aimed at helping improve how patients with colorectal cancer share information about the genetic…
Continue Reading
-
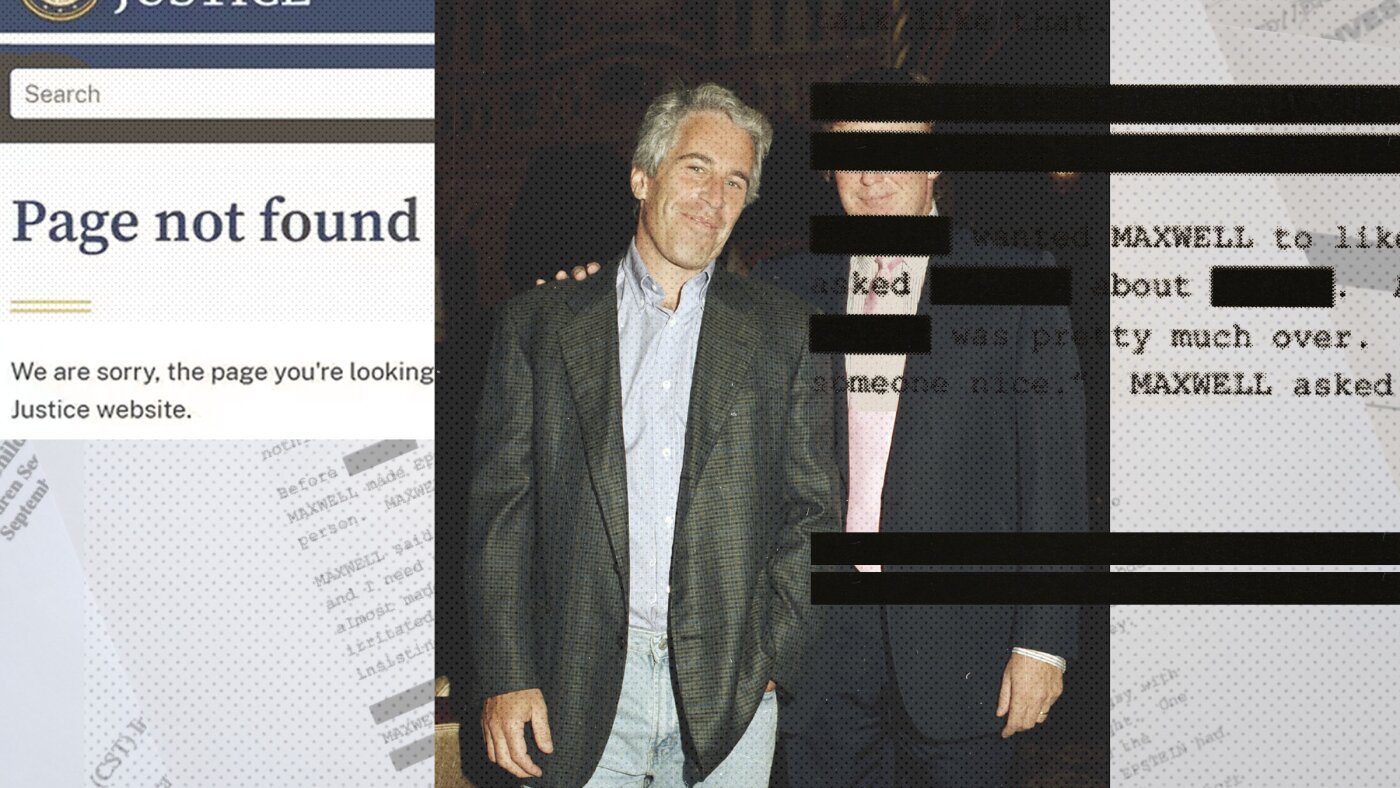
Justice Department posts more Epstein files related to accusations about Trump : NPR
An NPR investigation finds the Justice Department has removed or withheld Epstein files related to sexual abuse accusations…
Continue Reading
-

When Will Iran War End? Trump Says He Has ‘No Time Limits’, But Lays Out Objectives Behind Attack | World News
Last Updated:
Detailing several objectives behind the attack on Iran, Trump said, “They can’t have a nuclear weapon. That’s number one, two, and three.”


")

US President Donald Trump. (AFP)
“I have no time limits,” said US…
Continue Reading
-
Gulf carriers resume limited flights, but missile fire fuels uncertainty – Reuters
- Gulf carriers resume limited flights, but missile fire fuels uncertainty Reuters
- US–Israel war on Iran enters day 7: Dubai Airports handles 1,140 flights in 84 hours, UAE warns against sensitive videos Gulf News
- More than 100 Emirates flights…
Continue Reading
-

Combination therapy can reduce harmful effects of senescent cells in diabetic kidney disease
Mayo Clinic researchers have identified a drug-and-supplement combination therapy that is capable of reducing the harmful effects of senescent cells – also known as “zombie cells” – in diabetic kidney disease. In eBioMedicine,…
Continue Reading