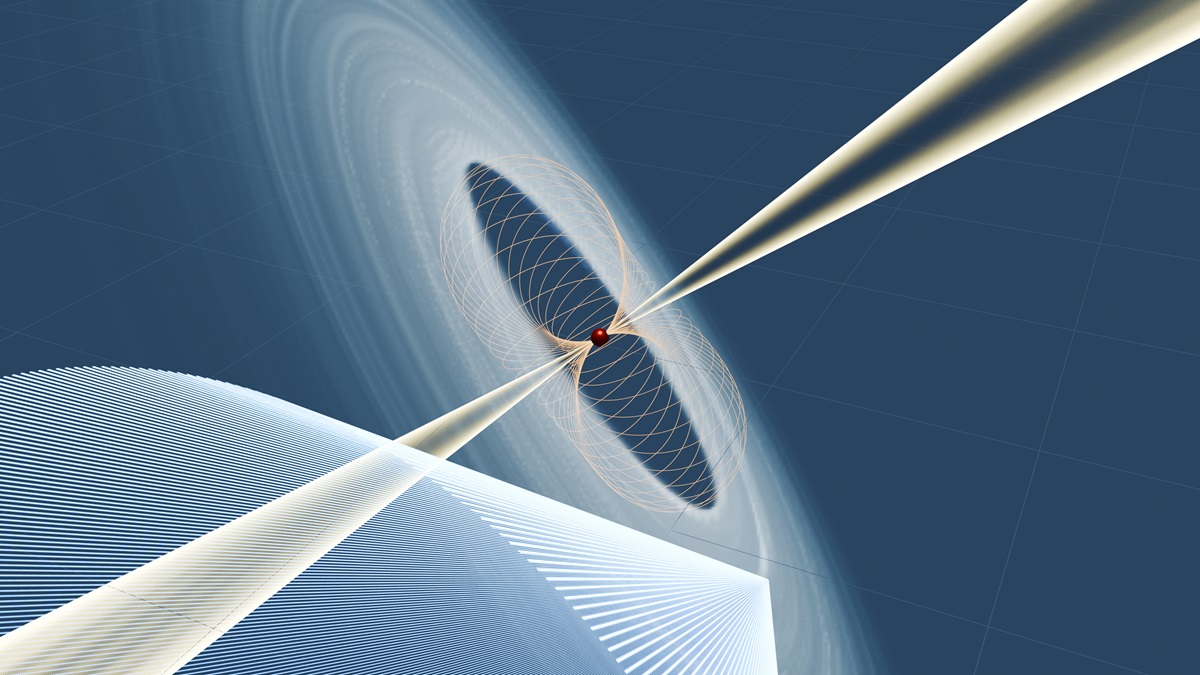
BEIJING, March 26 (Xinhua) — The Technology and Engineering Center for Space Utilization (CSU) of the Chinese Academy of Sciences (CAS) announced on Wednesday that the three-satellite constellation based on the Distant Retrograde Orbit (DRO)…


China sees ‘glimmer of hope’ for peace
China’s foreign minister has said that a “glimmer of hope” for peace has emerged due to moves to stop the war in the Middle East, despite Tehran vowing to keep fighting.
Wang Yi urged dialogue in…