- Met office forecasts rain & snowfall in various parts of country RADIO PAKISTAN
- First winter rain drenches parts of Karachi Dawn
- First snowfall, rain end dry spell The Express Tribune
- NDMA issues advisory in view of westerly wave Business…
Author: admin
-
Met office forecasts rain & snowfall in various parts of country – RADIO PAKISTAN
-

Gold and silver see rollercoaster end to blockbuster year
“Gold and silver prices are experiencing a notable rise due to the interplay of several economic, investment, and geopolitical factors,” said Rania Gule from trading platform XS.com.
The main driver of the price rises of precious metals, she added, are expectations that the US Federal Reserve will cut interest rates again in 2026. Prices of gold and silver were also buoyed by gold purchases by central banks and investors buying so-called “safe haven” assets due to concerns about global tensions and economic uncertainty.
Dan Coatsworth, head of markets at investment platform AJ Bell, said soaring gold and silver prices had been driven by investors “latching onto precious metals in response to concerns over inflation” as well as volatile stock markets.
“The market backdrop looks unchanged as we move into 2026,” he added.
Mr Coatsworth said high government debt in the UK and US, as well as Donald Trump’s tariffs and nerves over a potential AI bubble, would encourage investors to “stay bullish on gold and silver”.
But he warned sharp gains for the assets in 2025 make them vulnerable to a sharp pullback next year.
He said: “If financial markets go through a difficult patch, investors looking to liquidate positions might first reach for assets that have delivered strong gains in the past year or so, or ones that are easy to sell. Gold ticks both boxes.”
Ms Gule said she expects gold to continue to rise in 2026 but “at a more stable pace compared to the record highs observed in 2025”.
Also this year, central banks around the world added hundreds of tons of gold to their reserves, according to the World Gold Council trade association.
Daniel Takieddine, co-founder of investment firm Sky Links Capital Group, points to “supply tightness and industrial demand” for helping to push up the price of silver.
China, which is the world’s second biggest producer of silver, has said it would restrict the export of the precious metal.
In October, China’s Ministry of Commerce announced new restrictions on exports of silver as well as the metals tungsten and antimony to “to step up the protection of resources and the environment”.
Responding to a post on social media about Chinese government restrictions on silver exports, Tesla boss Elon Musk said: “This is not good. Silver is needed in many industrial processes.”
Mr Takieddine also highlighted the large amounts of money that have flowed into the precious metals market through investments like exchange-traded funds (ETFs).
ETFs are baskets of investments that trade on a stock exchange like a single stock. They can be seen as a convenient way to trade precious metals as investors do not have to take possession of physical bullion.
Silver also has the potential to rise again in the coming year, said Mr Takieddine. But he warns “rallies may be followed by sharper corrections.”
Continue Reading
-
Latvia makes playoffs with win – IIHF
- Latvia makes playoffs with win IIHF
- Tuesday night notes Station Nation
- Massive matchups with knockout round implications set for Day 5 of the World Juniors Puck Prose
- 2026 WJC Day 5 RECAP: Baltic Jubilation, Teutonic Humiliation Stanley Cup of…
Continue Reading
-

Gold and silver see rollercoaster end to blockbuster year
Gold and silver have seen a rollercoaster end to a year in which their prices are on track to record their biggest annual gains since 1979.
The price of gold soared by more than 60% this year to hit a record high of more than $4,549 (£3,378) an ounce before falling after Christmas to stand at about $4,330 on New Year’s Eve.
At the same time, silver was trading at about $71 an ounce after hitting an all-time high of $83.62 on Monday.
This year’s gains were driven by several factors including expectations of more interest rate cuts, gold purchases by central banks and investors buying so-called “safe haven” assets due to concerns about global tensions and economic uncertainty.
“Gold and silver prices are experiencing a notable rise due to the interplay of several economic, investment, and geopolitical factors,” said Rania Gule from trading platform XS.com.
The main driver of the price rises of precious metals, she added, are expectations that the US Federal Reserve will cut interest rates again in 2026.
Also this year, central banks around the world added hundreds of tons of gold to their reserves, according to the World Gold Council trade association.
Daniel Takieddine, co-founder of investment firm Sky Links Capital Group, points to “supply tightness and industrial demand” for helping to push up the price of silver.
China, which is the world’s second biggest producer of silver, has said it would restrict the export of the precious metal.
In October, China’s Ministry of Commerce announced new restrictions on exports of silver as well as the metals tungsten and antimony to “to step up the protection of resources and the environment”.
Responding to a post on social media about Chinese government restrictions on silver exports, Tesla boss Elon Musk said: “This is not good. Silver is needed in many industrial processes.”
Mr Takieddine also highlighted the large amounts of money that have flowed into the precious metals market through investments like exchange-traded funds (ETFs).
ETFs are baskets of investments that trade on a stock exchange like a single stock. They can be seen as a convenient way to trade precious metals as investors do not have to take possession of physical bullion.
Ms Gule said she expects gold to continue to rise in 2026 but “at a more stable pace compared to the record highs observed in 2025”.
Silver also has the potential to rise again in the coming year, said Mr Takieddine. But he warns “rallies may be followed by sharper corrections.”
Continue Reading
-
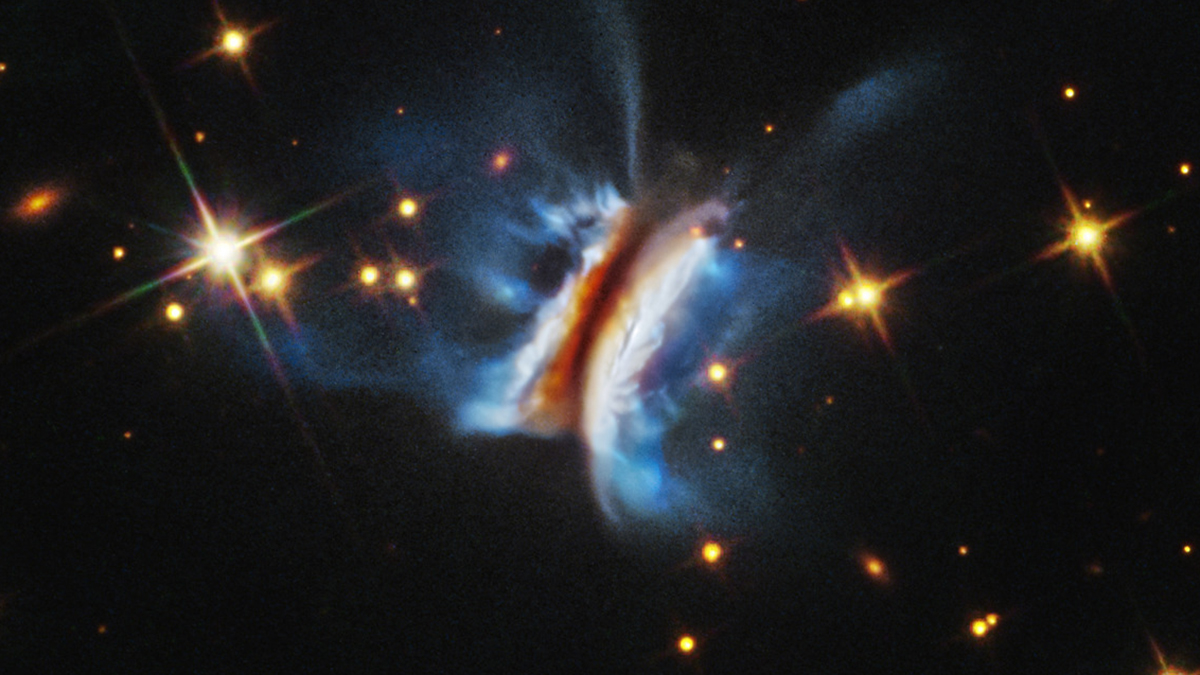
Hubble Reveals Extreme Chaos Inside ‘Dracula’s Sandwich’ : ScienceAlert
As a young star develops, so too does a protoplanetary disk of dust and gas around it, ready to birth new planets. Scientists have just discovered more about IRAS 23077+6707, the largest protoplanetary disk ever observed by a telescope.
First…
Continue Reading
-
Illinois 30-28 Tennessee (Dec 30, 2025) Game Recap – ESPN
- Illinois 30-28 Tennessee (Dec 30, 2025) Game Recap ESPN
- Where to watch Tennessee vs Illinois in the Music City Bowl streaming free today; TV Channel, time, odds OregonLive.com
- Nashville Braces for Influx of 50,000 Fans at Nissan Stadium for Music…
Continue Reading
-
Illinois 30-28 Tennessee (Dec 30, 2025) Game Recap – ESPN
- Illinois 30-28 Tennessee (Dec 30, 2025) Game Recap ESPN
- Tennessee and Illinois set for Music City Bowl with each team missing starters Citizen Tribune
- Nashville Braces for Influx of 50,000 Fans at Nissan Stadium for Music City Bowl Hoodline
Continue Reading
-

Dupilumab-Induced Cerebral Infarction Secondary to Hypoperfusion in an
Introduction
Bullous pemphigoid is a chronic, subepidermal autoimmune blistering disorder, the pathogenesis involves autoantibodies targeting hemidesmosomal proteins BP180 and BP230, which are essential for dermal–epidermal adhesion.1 Patients…
Continue Reading
-

Lucas: FSU Rapid Reactions – University of North Carolina Athletics
By Adam Lucas1. Carolina started slow but then cruised over Florida State, 79-66. The Heels are now 65-8 in ACC home openers and are 10-0 at the Smith Center this year.
2. Caleb Wilson, Caleb Wilson, Caleb Wilson. There will be much more about…
Continue Reading
-
Euphorbia neriifolia L. extract protects against cardiomyocyte injury and heart failure
Announcing a new publication for Acta Materia Medica journal. Heart failure (HF) remains a major global health challenge with limited therapeutic options, thus prompting the search for novel cardioprotective agents among traditional…
Continue Reading