Your request was blocked by our Web Application Firewall for security reasons.
Please try the following steps:
- Clear cookies for this site
- Try…
Your request was blocked by our Web Application Firewall for security reasons.
Please try the following steps:
“Interestingly, the liquid crystals in LCEs can reorient their microstructure alignment when they’re pulled or stressed,” said study principal investigator Lihua Jin, an associate professor of mechanical and aerospace engineering at the…
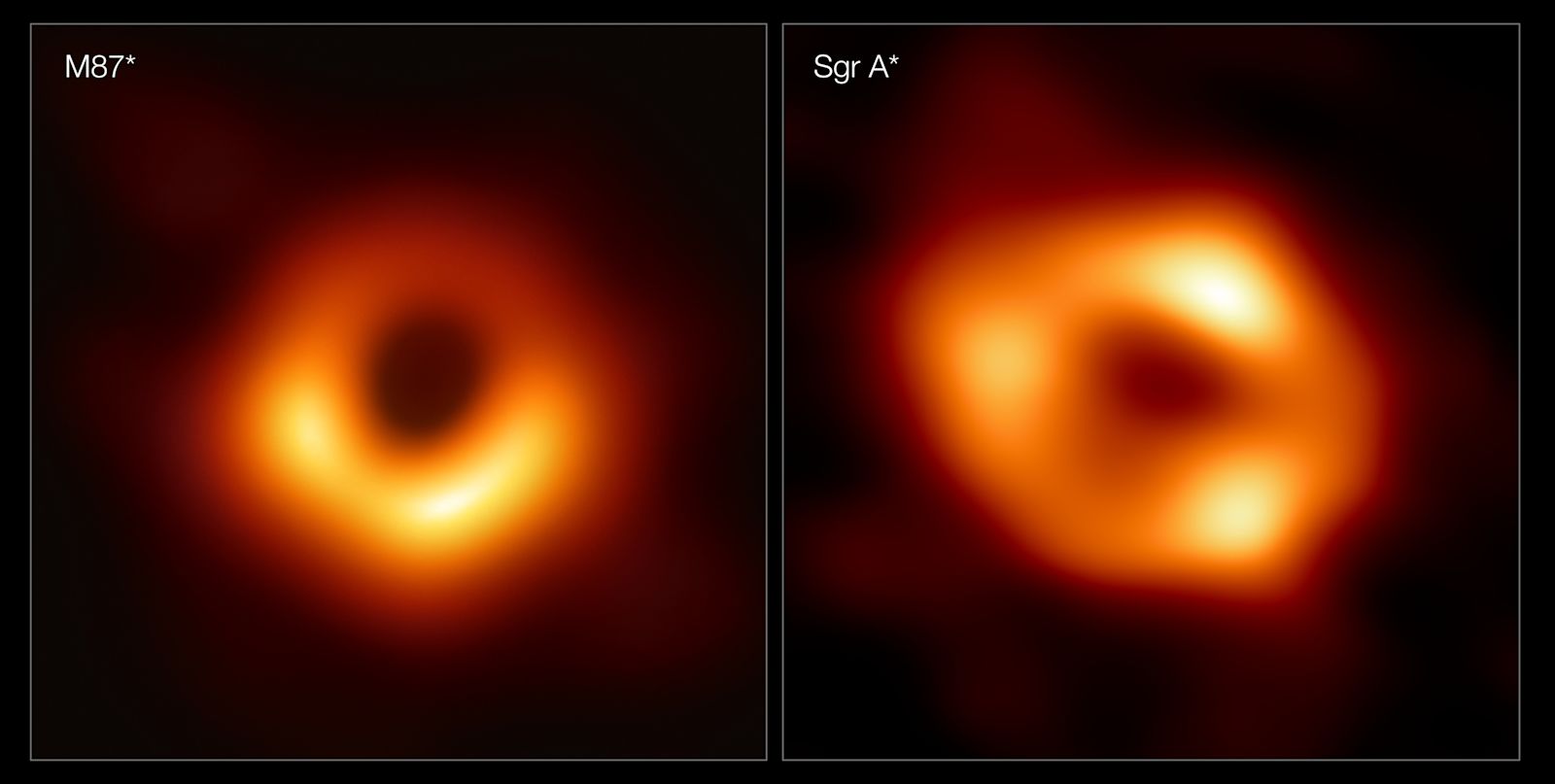
A multimillion-pound research project will see some of the world’s leading experts use artificial intelligence to create the first-ever 3D movies of black holes.
Kazunori Akiyama is joining Heriot-Watt University for the TomoGrav project, which…
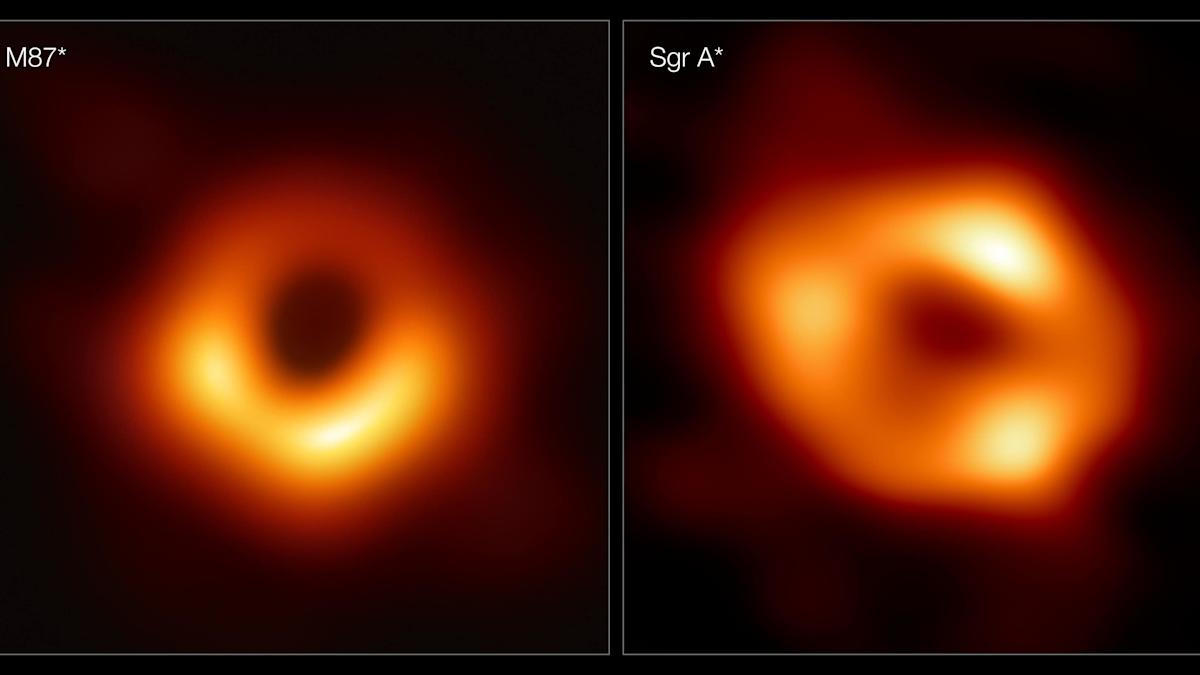
A multimillion-pound research project will see some of the world’s leading experts use artificial intelligence to create the first-ever 3D movies of black holes.
Kazunori Akiyama is joining Heriot-Watt University for the TomoGrav project,…

Toni Connor and Luke SprouleBBC News NI
 Family handout
Family handoutThe family of a County Down pensioner who was found unresponsive after being given the wrong medication by domiciliary carers have…
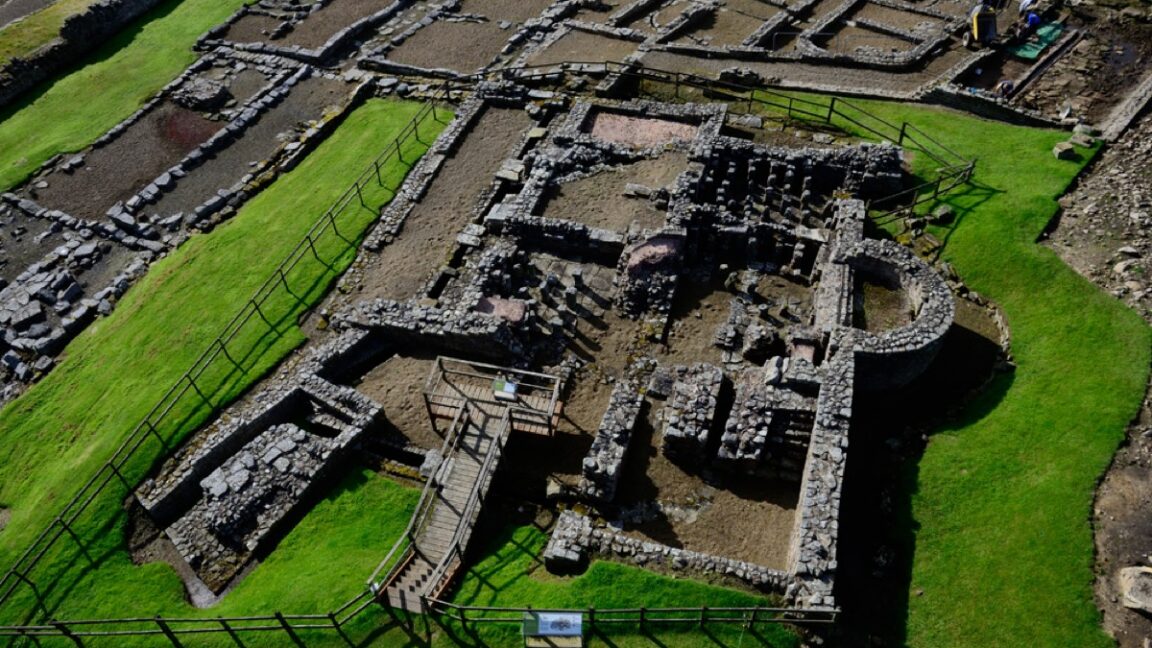
It probably sucked to be a Roman soldier guarding Hadrian’s Wall circa the third century CE. W.H. Auden imagined the likely harsh conditions in his poem “Roman Wall Blues,” in which a…

Jonathan HeadSouth East Asia correspondent in Cambodia
 BBC
BBCThe costs of the border war between Thailand and Cambodia are cruelly obvious in the hospital in…

A former Nascar driver and his family were among the seven people killed in a plane crash at a regional airport in North Carolina, the car-racing organisation has said.
A highway patrol spokesman said people on the ground confirmed that Greg…