- Nobel laureate Omar Yaghi on turning air into water for all University of California, Berkeley
- Device that can extract 1,000 liters of clean water a day from desert air revealed by 2025 Nobel Prize winner — claimed to work in desert air with 20% humidity or lower, delivering off-grid ‘personalized water’ Tom’s Hardware
- Meet Evelyn N. Wang: The scientist who wants to make every home produce its own water The Times of India
- Who is Omar Yaghi? This Nobel Prize winner made a device that pulls 1,000 litres of water from desert Air Moneycontrol.com
- New technology extracts drinking water from dry desert air Earth.com
Author: admin
-
Nobel laureate Omar Yaghi on turning air into water for all – University of California, Berkeley
-
Iran Hits Key US Radar, Deepening Gulf Missile Defense Woes – Bloomberg.com
- Iran Hits Key US Radar, Deepening Gulf Missile Defense Woes Bloomberg.com
- Radar bases housing key US missile interceptor hit in Jordan, Saudi Arabia, and UAE, satellite images show CNN
- Iran Strikes U.S. Military Communication Infrastructure in…
Continue Reading
-
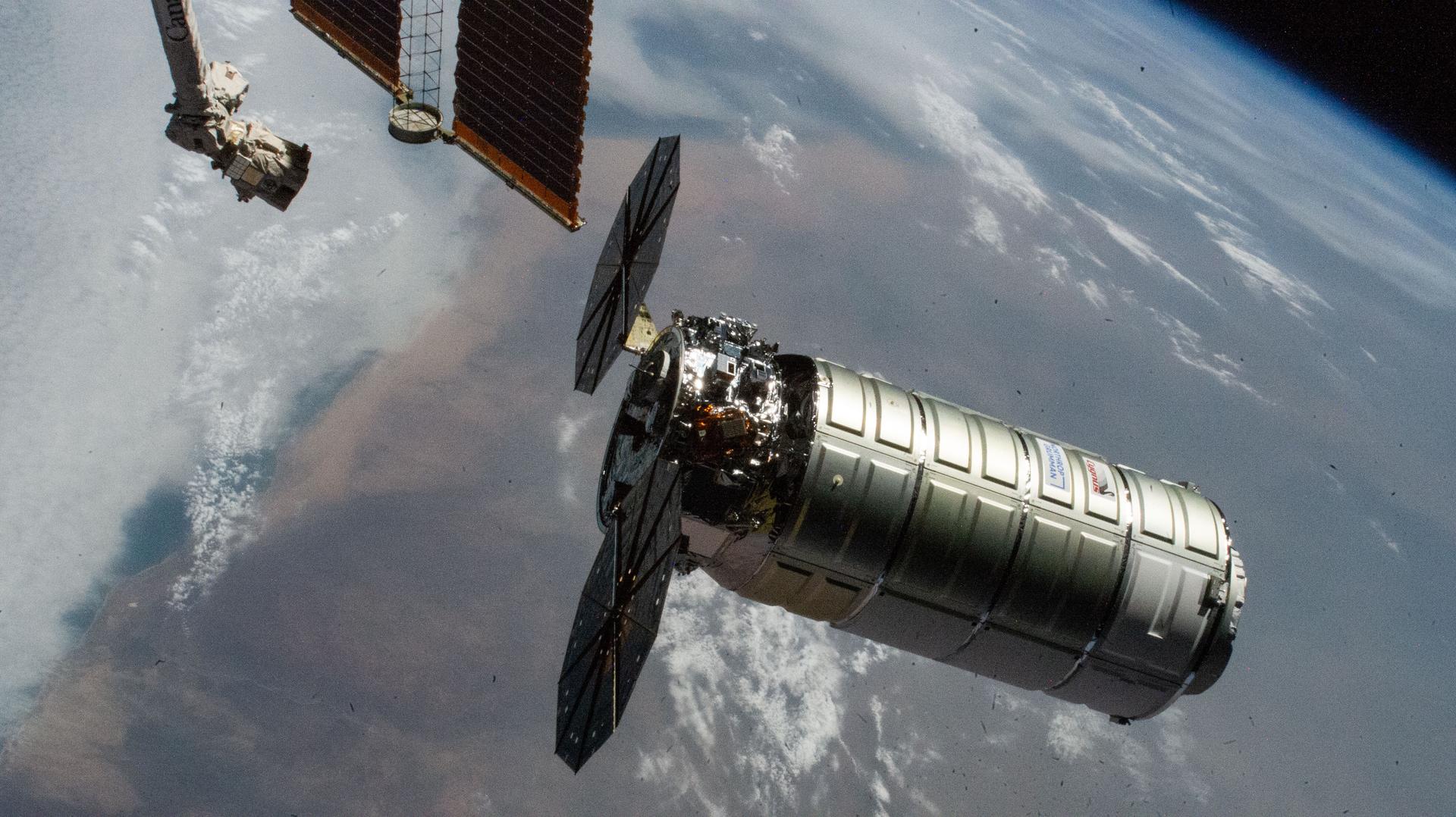
NASA Invites Media to Northrop Grumman CRS-24 Station Resupply Launch
Media accreditation is open for the next launch to deliver NASA science investigations, supplies, and equipment to the International Space Station. A Northrop Grumman Cygnus XL spacecraft will launch in April to the orbital laboratory on a…
Continue Reading
-
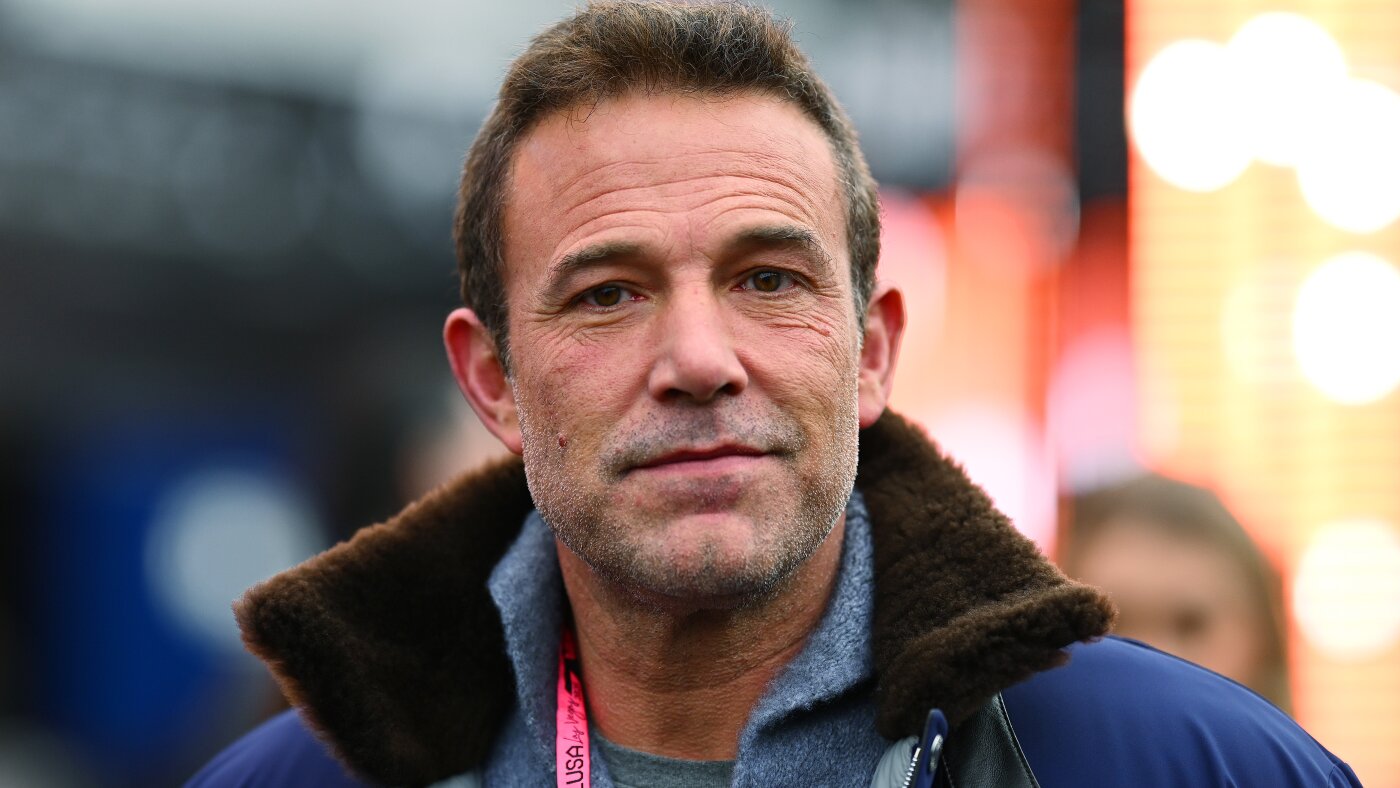
Netflix strikes deal with Ben Affleck’s InterPositive AI company : NPR
Hollywood A-lister Ben Affleck says his company InterPositive’s AI tools “take out all the logistical, difficult, technical…
Continue Reading
-

Scientists grow chickpeas in ‘moon dirt’
Scientists working to cultivate the field of extraterrestrial agriculture have grown chickpeas in dirt made mostly of simulated lunar soil, a step toward enabling astronauts on long-term moon missions to produce their own food.
Researchers said…
Continue Reading
-

All results and medallists from Milano Cortina 2026 – Full list
The Milano Cortina 2026 Paralympic Winter Games are underway, taking place from 6-15 March.
Over 600 athletes from 55 nations will compete at the Winter Games, in what is the 50th anniversary of the first edition in Örnsköldsvik, Sweden….
Continue Reading
-
From rapper to Prime Minister? Former musician emerges as contender in Nepal elections
Shah, widely known by his stage name “Balen,” first gained national recognition as a rapper before transitioning into politics. In recent years, he rose to prominence after being elected mayor of Kathmandu, the country’s…
Continue Reading
-

David Malukas Earns First Career NTT P1 Award at Phoenix
The stage is set for an even bigger breakthrough for David Malukas after he earned his first career NTT P1 Award in qualifying Friday for the Good Ranchers 250 at Phoenix Raceway.
Malukas’ first pole is paving the fastest path for…
Continue Reading
-

40,000-Year-Old Ice Age Symbols May Be First Step in Writing

The mammoth figurine from Vogelherd Cave. (Photo: University of Tübingen / Hildegard Jensen CC BY 4.0)
Long before cities, agriculture, or record keeping, Ice Age humans carved small lines and dots into ivory and bone….
Continue Reading
-
Iran's UN envoy says 1,332 Iranian civilians killed in war – Reuters
- Iran’s UN envoy says 1,332 Iranian civilians killed in war Reuters
- How the world has reacted to US and Israeli strikes on Iran BBC
- ITUC urges immediate ceasefire and renewed peace talks in the Middle East International Trade Union Confederation
Continue Reading