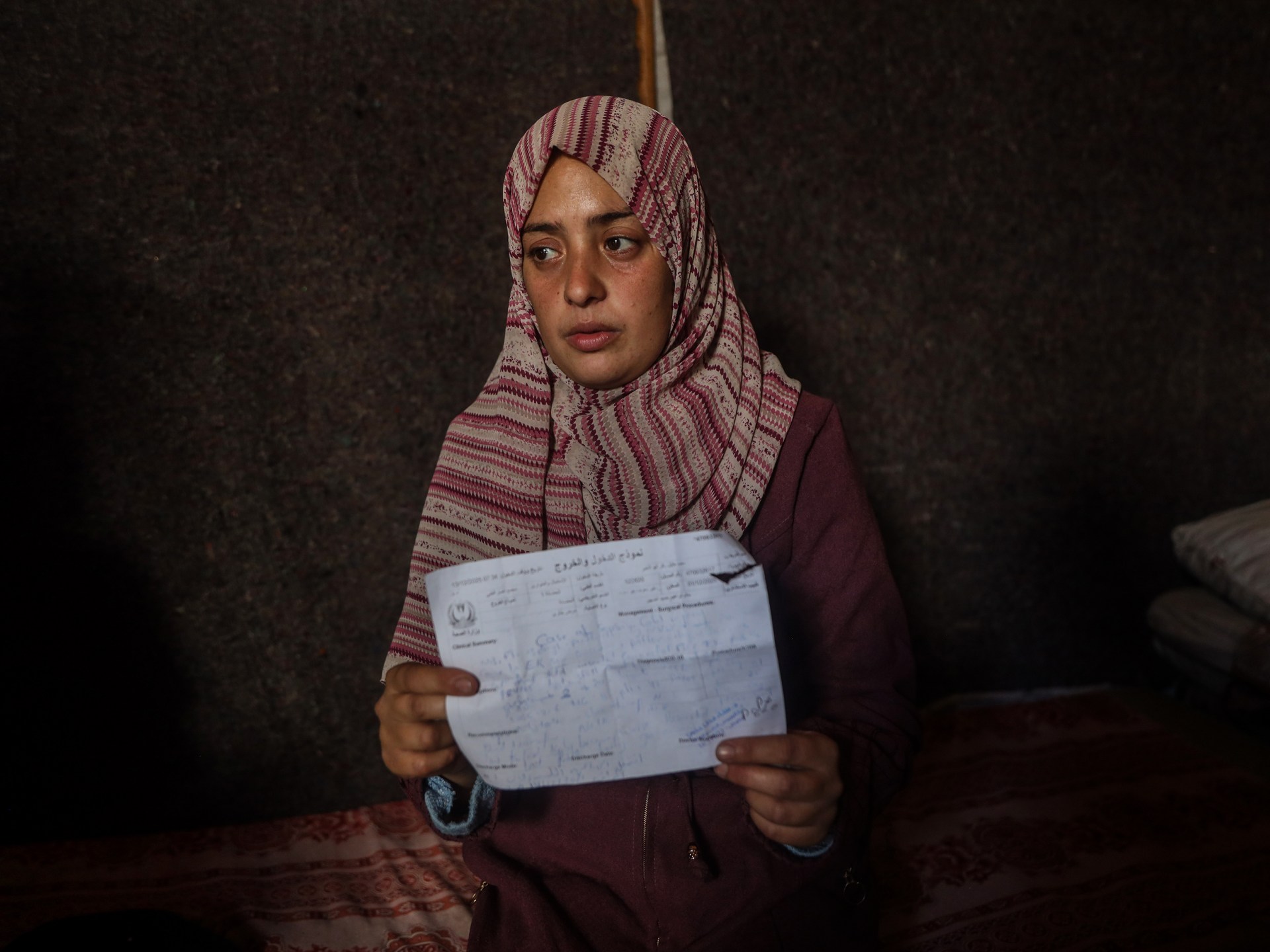
Khan Younis, Gaza Strip – With a pale face and unrelenting tears, Eman Abu al-Khair sits inside her tent, clutching a small bag of her infant’s clothes. Her newborn had died of hypothermia the day before.
The devastated mother, 34-years-old,…
Khan Younis, Gaza Strip – With a pale face and unrelenting tears, Eman Abu al-Khair sits inside her tent, clutching a small bag of her infant’s clothes. Her newborn had died of hypothermia the day before.
The devastated mother, 34-years-old,…



The Housemaid by Freida McFadden claimed the title of this year’s most unputdownable fiction title in the UK, with Kindle readers crowning it the most read fiction title of the year. Meanwhile, thrilling reads The Boyfriend, also by McFadden,…
Leipzig is the only BMW Group plant that produces BMW and MINI models on the same line – including all drive variants: combustion, hybrid, electric. This flexibility is a logistical masterpiece, comparable to a stage where a different…

Researchers in a recent study have identified alarming trends among adults who…
This release contains certain forward-looking statements, including “forward-looking” statements made within the meaning of the U.S. Private Securities Litigation Reform Act of 1995. These statements are often, but…

Minister calls for a shift towards innovation, commercialisation, and industry linkages
Minister for Planning Development & Special Initiatives Ahsan Iqbal. PHOTO: APP

A third of UK citizens have used artificial intelligence for emotional support, companionship or social interaction, according to the government’s AI security body.
The AI Security Institute (AISI) said nearly one in 10 people used systems like…
The 2026 EE BAFTA Film Awards will air on Sunday 22 February 2026 on BBC One and iPlayer
Photos available here
Photo credit: BAFTA / Charlie Clift
London, 18 December 2025: BAFTA has today announced…