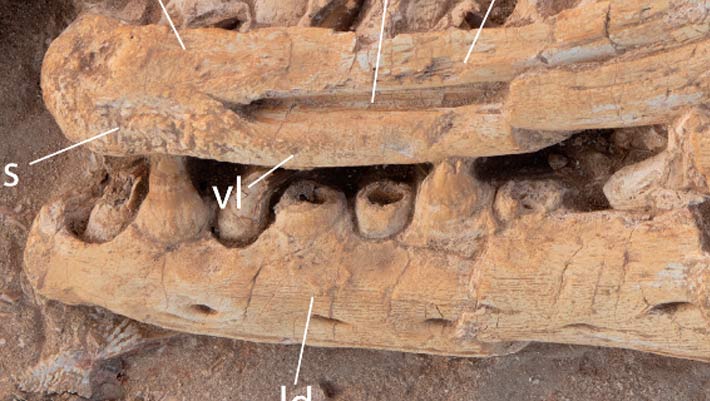
Paleontologists have identified a new, giant species of the mosasaur genus Pluridens from the Late Cretaceous phosphate deposits of Morocco. Named Pluridens imelaki, the species belonged to a group of relatively slender-jawed mosasaurs and may…
Author: admin
-

1,979 Pakistanis arrive via Taftan
Safe passage: People walk into Pakistan via the Taftan border crossing amid ongoing US-Israel strikes on Iran. Photo: AFP
…Continue Reading
-

Scientists say most of what you do each day happens on autopilot
A new study by researchers from the University of Surrey, the University of South Carolina, and Central Queensland University suggests that much of what we do each day is guided by habit rather than deliberate decision making.
The research,…
Continue Reading
-
Artificial intelligence, greening of occupational structure and total factor energy efficiency
Acemoglu D (2018) Artificial intelligence, automation and work. National Bureau of Economic Research Working Paper, No. w24196
Acemoglu D, Restrepo P (2019) Automation and new tasks: How technology displaces and reinstates labor. J Econ Perspect 33(2):3–30
Acemoglu D, Restrepo P (2020) Robots and jobs: Evidence from US labor markets. J Political Econ 128(6):2188–2244
Acemoglu D (2021) Harms of AI. National Bureau of Economic Research Working Paper, No. w29247
Acemoglu D, Autor D, Dorn D, Hanson GH, Price B (2016) Import competition and the great US employment sag of the 2000s. J Labor Econ 34(S1):S141–S198
Acemoglu D, Autor D, Hazell J, Restrepo P (2022) Artificial intelligence and jobs: Evidence from online vacancies. J Labor Econ 40(S1):S293 S340
Altonji JG, Elder TE, Taber CR (2005) Selection on observed and unobserved variables: Assessing the effectiveness of Catholic schools. J Political Econ 113(1):151–184
Antonopoulos I, Robu V, Couraud B, Kirli D, Norbu S, Kiprakis A, Wattam S (2020) Artificial intelligence and machine learning approaches to energy demand side response: A systematic review. Renew Sustain Energy Rev 130:109899
Autor DH, Levy F, Murnane RJ (2003) The skill content of recent technological change: An empirical exploration. Q J Econ 118(4):1279–1333
Autor DH, Dorn D (2013) The growth of low-skill service jobs and the polarization of the US labor market. Am Econ Rev 103(5):1553–1597
Babina T, Fedyk A, He AX, Hodson J (2023) Firm investments in artificial intelligence technologies and changes in workforcecomposition. National Bureau of Economic Research Working Paper, No. w31325
Barbieri N, Marzucchi A, Rizzo U (2023) Green technologies, interdependencies, and policy. J Environ Econ Manag 118:102791
Berrone P, Fosfuri A, Gelabert L, Gomez Mejia LR (2013) Necessity as the mother of ‘green’ inventions: Institutional pressures and environmental innovations. Strategic Manag J 34(8):891–909
Bocken NMP, de Pauw I, Bakker C, van der Grinten B (2016) Product design and business model strategies for a circular economy. J Ind Prod Eng 33(5):308–320
Bose BK (2017) Artificial intelligence techniques in smart grid and renewable energy systems some example applications. Proc IEEE 105(11):2262–2273
Bowen A, Kuralbayeva K, Tipoe EL (2018) Characterising green employment: The impacts of ‘greening’on workforce composition. Energy Econ 72:263–275
Cainelli G, D’Amato A, Mazzanti M (2020) Resource efficient eco innovations for a circular economy: Evidence from EU firms. Res Policy 49(1):103827
Centobelli P, Cerchione R, Chiaroni D, Del Vecchio P, Urbinati A (2022) Blockchain technology for bridging trust, traceability and transparency in circular supply chain. Inf Manag 59(3):103508
Chen M, Wang X, Zhang Z (2024) How can the digital economy reduce carbon emissions? Empirical evidence from China. PLoS One 19(6):e0303582
Consoli D, Marin G, Marzucchi A, Vona F (2016) Do green jobs differ from non green jobs in terms of skills and human capital? Res Policy 45(5):1046–1060
Curtis EM (2018) Who loses under cap and trade programs? The labor market effects of the NOx budget trading program. Rev Econ Stat 100(1):151–166
Curtis EM, O’Kane L, Park RJ (2024) Workers and the green energy transition: Evidence from 300 million job transitions. Environ Energy Policy Econ 5(1):127–161
Darendeli A, Law KKF, Shen M (2022) Green new hiring. Rev Acc Stud 27(3):986–1037
Dauth W, Findeisen S, Suedekum J, Woessner N (2021) The adjustment of labor markets to robots. J Eur Econ Assoc 19(6):3104–3153
De Jesus A, Mendonça S (2018) Lost in transition? Drivers and barriers in the eco innovation road to the circular economy. Ecol Econ 145:75–89
Deming DJ (2017) The growing importance of social skills in the labor market. Q J Econ 132(4):1593–1640
Elliott RJR, Kuai W, Maddison D, Ozgen C (2024) Eco innovation and (green) employment: A task based approach to measuring the composition of work in firms. J Environ Econ Manag 127:103015
Fang VW, Tian X, Tice S (2014) Does stock liquidity enhance or impede firm innovation? J Financ 69(5):2085–2125
Geissdoerfer M, Savaget P, Bocken NMP, Hultink EJ (2017) The circular economy—A new sustainability paradigm? J Clean Prod 143:757–768
Ghisetti C, Marzucchi A, Montresor S (2015) The open eco innovation mode: An empirical investigation of eleven European countries. Res Policy 44(5):1080–1093
Grüning P (2025) Fiscal, environmental, and bank regulation policies in a small open economy for the green transition. Resour Energy Econ 82:101493
Isogawa D, Nishikawa K, Ohashi H (2012) Innovation height and firm performance: Using innovation survey from Japan (RIETI Discussion Paper Series 12 E 077). Research Institute of Economy, Trade and Industry
Kerr WR, Kominers SD (2015) Agglomerative forces and cluster shapes. Rev Econ Stat 97(4):877–899
Lachenmaier S, Rottmann H (2011) Effects of innovation on employment: A dynamic panel analysis. Int J Ind Organ 29(2):210–220
Lim Z, Sun Y, Xing C, Liu J, He Y, Zhou Y, Zhang G (2022) Artificial intelligence powered large scale renewable integrations in multi energy systems for carbon neutrality transition: Challenges and future perspectives. Energy AI 10:100196
Lundgren T, Marklund PO, Zhang S (2016) Industrial energy demand and energy efficiency, Evidence from Sweden. Resour Energy Econ 43:130–152
Marin G, Vona F (2019) Climate policies and skill biased employment dynamics: Evidence from EU countries. J Environ Econ Manag 98:102253
Martin G (2019). Sustainability prospects for autonomous vehicles: Environmental, social, and urban. Routledge
Mehmood MU, Chun D, Zeeshan, Han H, Jeon G, Chen K (2019) A review of the applications of artificial intelligence and big data to buildings for energy efficiency and a comfortable indoor living environment. Energy Build 202:109383
Morgenstern RD, Pizer WA, Shih JS (2002) Jobs versus the environment: An industry level perspective. J Environ Econ Manag 43(3):412–436
Ounifi HA, Gherbi A, Kara N (2022) Deep machine learning based power usage effectiveness prediction for sustainable cloud infrastructures. Sustain Energy Technol Assess 52:101967
Popp D, Vona F, Marin G, Chen Z (2020) The employment impact of green fiscal push: Evidence from the American Recovery and Reinvestment Act. National Bureau of Economic Research Working Paper, No. w27321
Pu B, Lu L, Tan J, Ping J, Wu C (2023) Impact of digital economy on energy supply chain efficiency: Evidence from Chinese energy enterprises. Energies 16(1):157–174
Stock JH, Yogo M (2002) Testing for weak instruments in linear IV regression (NBER Technical Working Paper No. 0284). National Bureau of Economic Research
Sunder J, Sunder SV, Zhang J (2017) Pilot CEOs and corporate innovation. J Financial Econ 123(1):209–224
Tianren L, Sufeng H (2024) Does Digital Industrial Technology Integration reduce corporate carbon emissions? Environ Res 257:119313
Topalova P (2004) Trade liberalization, poverty and inequality: Evidence from Indian districts (NBER Working Paper No. 11614). National Bureau of Economic Research
Vinuesa R, Azizpour H, Leite I, Balaam M, Dignum V, Domisch S, Felländer A, Langhans SD, Tegmark M, Fuso Nerini F (2020) The role of artificial intelligence in achieving the Sustainable Development Goals. Nat Commun 11(1):233
Vona F, Marin G, Consoli D (2019) Measures, drivers and effects of green employment: evidence from US local labor markets, 2006–2014. J Econ Geogr 19(5):1021–1048
Vona F, Marin G, Consoli D, Popp D (2018) Environmental regulation and green skills: An empirical exploration. J Assoc Environ Resour Economists 5(4):713–753
Walker WR (2013) The transitional costs of sectoral reallocation: Evidence from the Clean Air Act and the workforce. Q J Econ128(4):1787–1835
Wu H, Wu Z, Wu H, Tang C, Zhang Z (2025) Policy intervention, digital village and micro modern energy use: evidence from the China Family Panel Studies (CFPS). Econ Change Restruct 58(4):72
Xu H, Li Y, Lin W, Wang H (2024) ESG and customer stability: a perspective based on external and internal supervision and reputation mechanisms. Humanit Soc Sci Commun 11:981
Yu Y, Zhang N (2021) Low-carbon city pilot and carbon emission efficiency: Quasi-experimental evidence from China. Energy Econ 96:105125
Zhang Z, Wu H, Zhang Y, Hu S, Pan Y, Feng Y (2024) Does digital global value chain participation reduce energy resilience? Evidence from 49 countries worldwide. Technol Forecast Soc Change 208:123712
Zhang Z, Zhang Y, Wu H, Song S, Pan Y, Feng Y (2024) Dual effects of automation on economy and environment: evidence from A-share listed enterprises in China. China Econ Rev 88:102308
Zhang Z, Zhang Y, Zhao M, Muttarak R, Feng Y (2023) What is the global causality among renewable energy consumption, financial development, and public health? New perspective of mineral energy substitution. Resour Policy 85:104036
Zhang Z, Zhao M, Chen Y, Song MC, Gao Y, Feng Y (2025) The nexus between energy legislation, energy transition, and energy resilience: Evidence from 55 countries worldwide. Energy 324:135906
Continue Reading
-

Pipeline potential of mini lab-grown organs – Opinion
[Photo/IC]
Chronic diseases have become the leading global health challenge, accounting for over 70 percent of deaths worldwide, a burden that continues to grow with aging populations and shifting…
Continue Reading
-

IRIS Dena: The final voyage of the Iranian warship sunk by the US
Under the Second Geneva Convention, countries at war are required to take “all possible measures” to rescue wounded or shipwrecked sailors after a naval attack. In practice, however, this duty applies only if a rescue can be attempted without…
Continue Reading
-

New antiretrovirals in the pipeline could be part of twice-yearly HIV treatment
aidsmap news story
Three experimental injectable antiretrovirals – a novel capsid inhibitor and two next-generation integrase inhibitors – could be components of future long-acting HIV treatment regimens, according to study results presented…
Continue Reading
-

Who is Balen Shah? Nepal’s rapper-mayor poised to become PM
- Shah’s rise challenges Nepal’s traditional political elite
- Shah’s popularity driven by social media and youth connection
- His party’s manifesto promises job creation and economic growth
After Nepal’s historic youth-led uprising last September killed…
Continue Reading
-

Who Made This Song? Platforms Start to Label AI Music
An artificial intelligence (AI)-generated country song reached No. 1 on Billboard’s Country Digital Song Sales chart last fall, and few listeners knew the song was created by a machine.
Continue Reading
-

Britney Spears Dui Arrest: Britney Spears’ DUI arrest prompts a response from ex-husband Sam Asghari as pop star faces fresh legal trouble | English Movie News
Britney Spears’ recent DUI arrest has drawn quick attention from her ex-husband Sam Asghari, who offered measured words on the matter. The pop icon’s legal trouble unfolded late on March 4, sparking concern among fans and former loved ones…
Continue Reading