
On June 2, 2023, Ajike Owens, a 35-year-old Black mother of four, was fatally shot by her 58-year-old white neighbor, Susan Lorincz. The deadly altercation marked the end of a two-year saga of responses from Marion County police to calls from…
Author: admin
-

Scientists discover rare exoplanet orbiting two suns | Northwest & National News
Scientists discover rare exoplanet orbiting two suns | Northwest & National News | nbcrightnow.com
We recognize you are attempting to access this website from a country…
Continue Reading
-
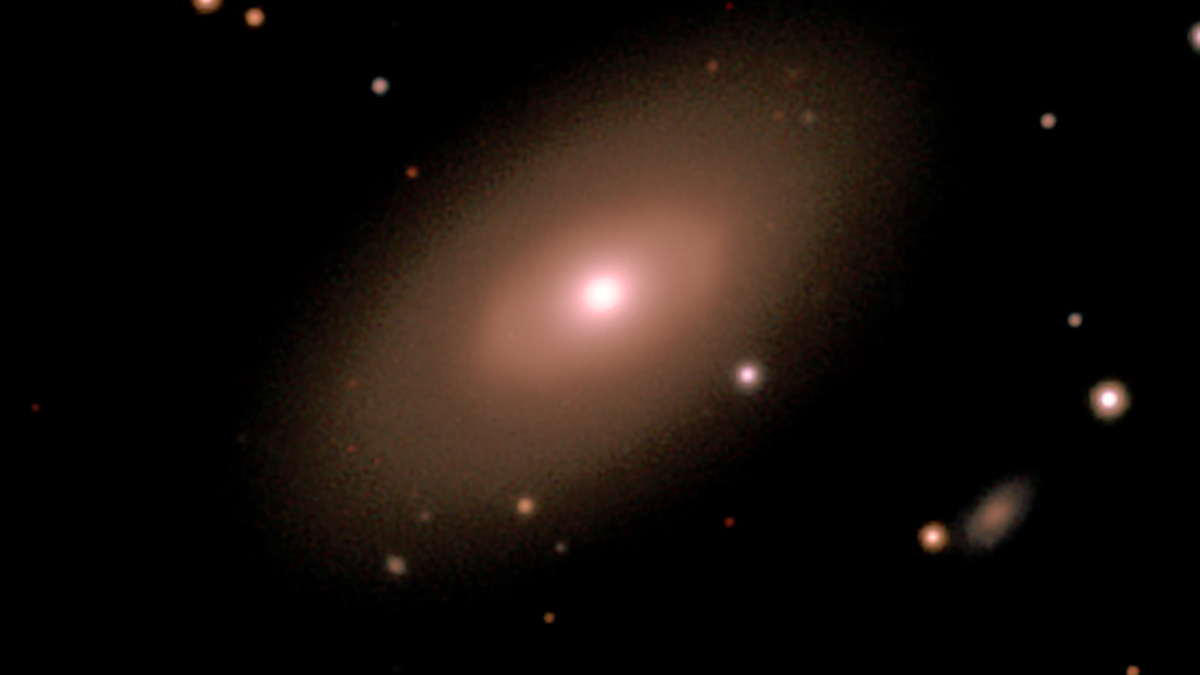
NASA’s Chandra finds small galaxies buck the black – @theU
Most smaller galaxies may not have supermassive black holes in their centers, according to a new study using NASA’s Chandra X-ray Observatory. This contrasts with other studies that suggested nearly every galaxy has one of these…
Continue Reading
-

New treatment slows down Huntington’s disease for the first time
For the first time, doctors have watched a treatment slow the course of Huntington’s disease in people, instead of just easing symptoms. In a small international trial, people who received an experimental, one-time treatment called AMT 130…
Continue Reading
-
Why does Netflix want to buy Warner Bros? To copy, not kill, traditional TV
The recent news that Netflix has agreed to buy part of Warner Bros Discovery (WBD) for US$83 billion (£61.8 billion), followed by Paramount Global’s hostile counterbid to acquire WBD in its entirety for US US$108.4 billion, has triggered…
Continue Reading
-

McDermott’s UK expansion at a crossroads after sole antitrust partner departs
Omar Shah has left McDermott Will & Schulte just six months after he joined the partnership in London.
…
Continue Reading
-
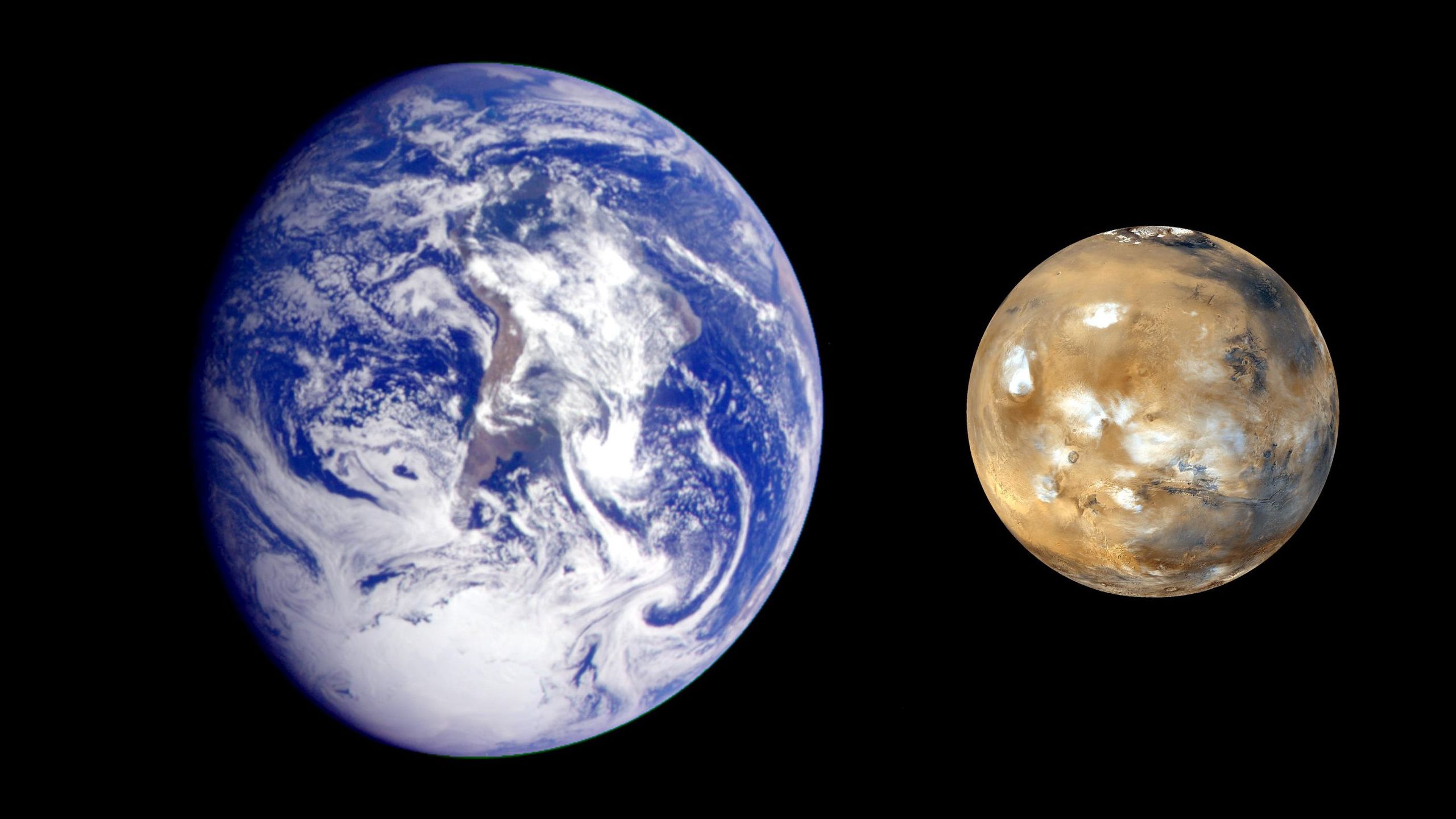
Time moves faster on Mars — proving Einstein right and posing new challenges for crewed missions
Scientists have found that time moves slightly faster on the Red Planet than it does on Earth. Clocks on Mars tick, on average, 0.477 milliseconds (477 microseconds) faster over 24 hours when measured from Earth compared with time recorded on…
Continue Reading
-

Marcus Rashford shows his social commitment
Barça’s English forward Marcus Rashford had the opportunity to visit two FC Barcelona Foundation projects today. Both were in Barcelona, and the first was Escola Vedruna, located in the Raval neighbourhood, followed by Centre Comunitari El…
Continue Reading
-
PTI divided over sit-ins outside Adiala jail; KP CM again denied meeting with Imran – Dawn
- PTI divided over sit-ins outside Adiala jail; KP CM again denied meeting with Imran Dawn
- KP CM fires fresh salvo at authorities after being denied meeting with Imran Khan for ’10th time’ Geo News
- KP CM again denied meeting with leader as PTI…
Continue Reading
-

Study finds sharp rise in prescriptions for stimulant medications used to treat ADHD
A new Ontario-based study has found a significant rise in prescriptions for stimulant medications used to treat attention-deficit/hyperactivity disorder (ADHD), particularly among adults and females. The study, published in JAMA…
Continue Reading