Employee Celebrations Continue to Celebrate Eight Decades of Dedication and Innovation
PORTLAND, Ore., Dec. 11, 2025 /PRNewswire/ — DSC®, a global leader in high-performance foam innovation, proudly…

Employee Celebrations Continue to Celebrate Eight Decades of Dedication and Innovation
PORTLAND, Ore., Dec. 11, 2025 /PRNewswire/ — DSC®, a global leader in high-performance foam innovation, proudly…
President Donald Trump has launched a scheme offering fast-tracked US visas to wealthy foreigners who can pay at least $1m (£750,000).
The card will give buyers a “direct path to Citizenship for all qualified and vetted people. SO EXCITING! Our…

WASHINGTON (TNND) — The medical community is still reeling after a federal advisory panel voted to end the automatic Hepatitis B vaccine at birth, a recommendation that has been in place for more than 30 years. Most of the public-health debate…

TOKYO, December 11, 2025—Canon Inc. today announced that it has reported to Amazon that certain toner cartridges sold on Amazon infringe Canon’s patents and requested the removal of such listings from Amazon.com.
In its reports to Amazon, Canon identified, among others, the product offerings shown in the table below and alleged that the cartridges sold under these offerings infringe Canon’s U.S. Patent No. 12,321,128. Canon requested that Amazon remove these product offerings from Amazon.com.
At the time of this announcement, the product offerings listed above were no longer available on Amazon.com.
Canon engages in extensive research and development so that it can deliver innovative and valuable products to customers all over the world. Through its research and development efforts, Canon has obtained a large and robust portfolio of patents. In order to protect its many innovations, Canon enforces its patents against various toner cartridge designs that Canon believes infringe its patent rights.
Throughout the development, sales and marketing process, Canon respects the intellectual property of other companies and individuals and expects others to similarly respect Canon’s intellectual property rights. Canon remains committed to pursuing legal enforcement against those who do not respect Canon’s intellectual property.
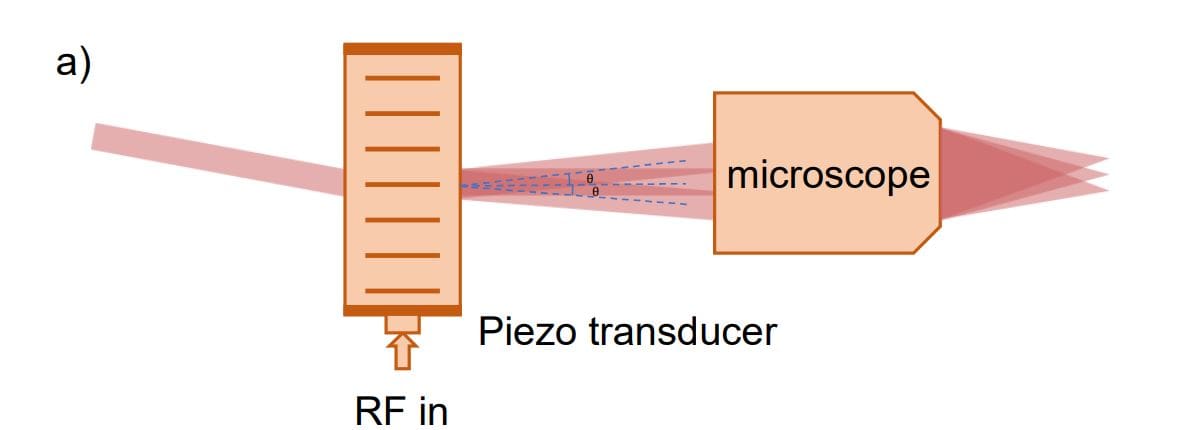
Creating large, precisely controlled arrays of optical tweezers represents a significant hurdle in developing practical quantum technologies, and researchers are continually seeking ways to increase the number of traps available. Yuqing Wang,…
By elevating ketone-driven energy pathways inside CD8+ T cells, dietary restriction steers them away from exhaustion and toward potent tumour-fighting states, unlocking stronger responses to immunotherapy in preclinical models.
Continue Reading

Pharmacy Times: Many patients first received PARP inhibitors in later lines of therapy. What role can pharmacists play in ensuring earlier recognition of eligible patients and optimizing PARPi sequencing?
Siddhartha Yadav, M.B.B.S., M.D.: Great…
You don’t have permission to access “http://www.spglobal.com/market-intelligence/en/news-insights/articles/2025/12/ldc-exits-iglu-great-point-acquires-majority-stake-in-lenis-group-96042492” on this server.
Reference #18.daa0d517.1765422385.333cfc2a
https://errors.edgesuite.net/18.daa0d517.1765422385.333cfc2a

The human small intestine absorbs nutrients while protecting us from potentially harmful microbes. One of the cell types that plays a key role in this protection is the microfold cell, or M cell. These cells detect bacteria and…