For decades, scientists have tried to replace the insulin-producing cells destroyed in type 1 diabetes. But even when new cells are transplanted, the immune system often attacks them again.
A new strategy may help solve that problem. Researchers…

For decades, scientists have tried to replace the insulin-producing cells destroyed in type 1 diabetes. But even when new cells are transplanted, the immune system often attacks them again.
A new strategy may help solve that problem. Researchers…

[Editor’s Note: Follow Khaleej Times live blog amid US-Israel-Iran war for the latest regional developments.]
Dubai confirmed that debris which fell during an aerial interception resulted in the death of one person. The incident occurred on…

USWNT vs. COLOMBIA
Date: March 7, 2026
Venue: Sports Illustrated Stadium, N.J.
Broadcast: TNT, truTV and HBO Max in English and in Spanish on Universo and Peacock
Radio: Westwood One in English and Futból de Primera in Spanish
Official Kickoff Time:…
Last year, OpenAI cofounder and former exec Andrej Karpathy coined the term “vibe coding,” a…

RUSSELLVILLE, Ark. – Following a dominant individual performance that led No. 26 Harding to a team…
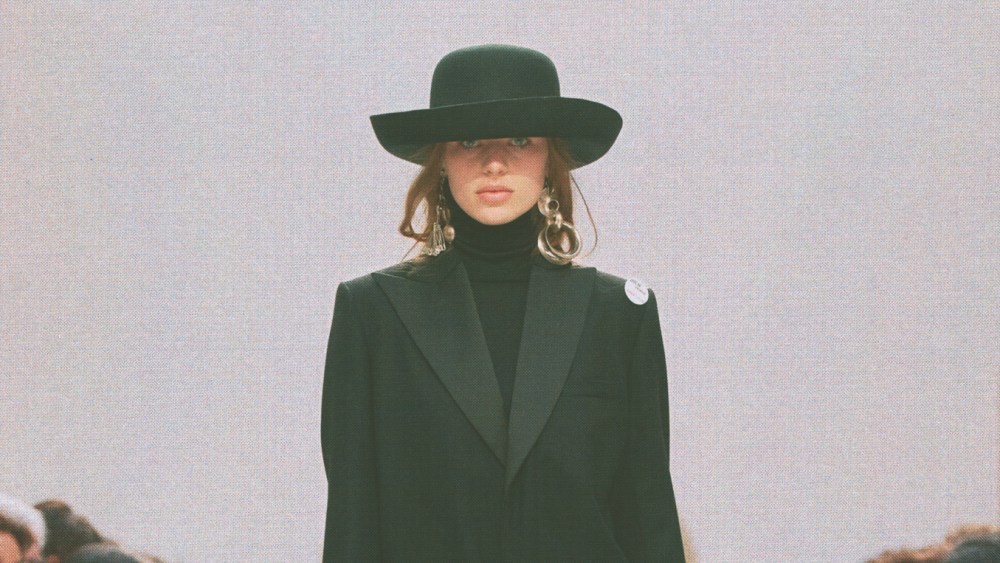
Staging his third show as artistic director of Celine, Michael Rider has crystallized his fashion sweet spot as classics “with bite.”
It’s a trenchant way to sum up his magnificent clothes, which are familiar, often sober and…
