Punjab’s 80 Ramazan markets received 40 million visitors during the holy month, reflecting massive public reliance on subsidised bazaars for essential commodities.
LAHORE: The Punjab government’s network of 80 Ramazan markets established across…

Punjab’s 80 Ramazan markets received 40 million visitors during the holy month, reflecting massive public reliance on subsidised bazaars for essential commodities.
LAHORE: The Punjab government’s network of 80 Ramazan markets established across…
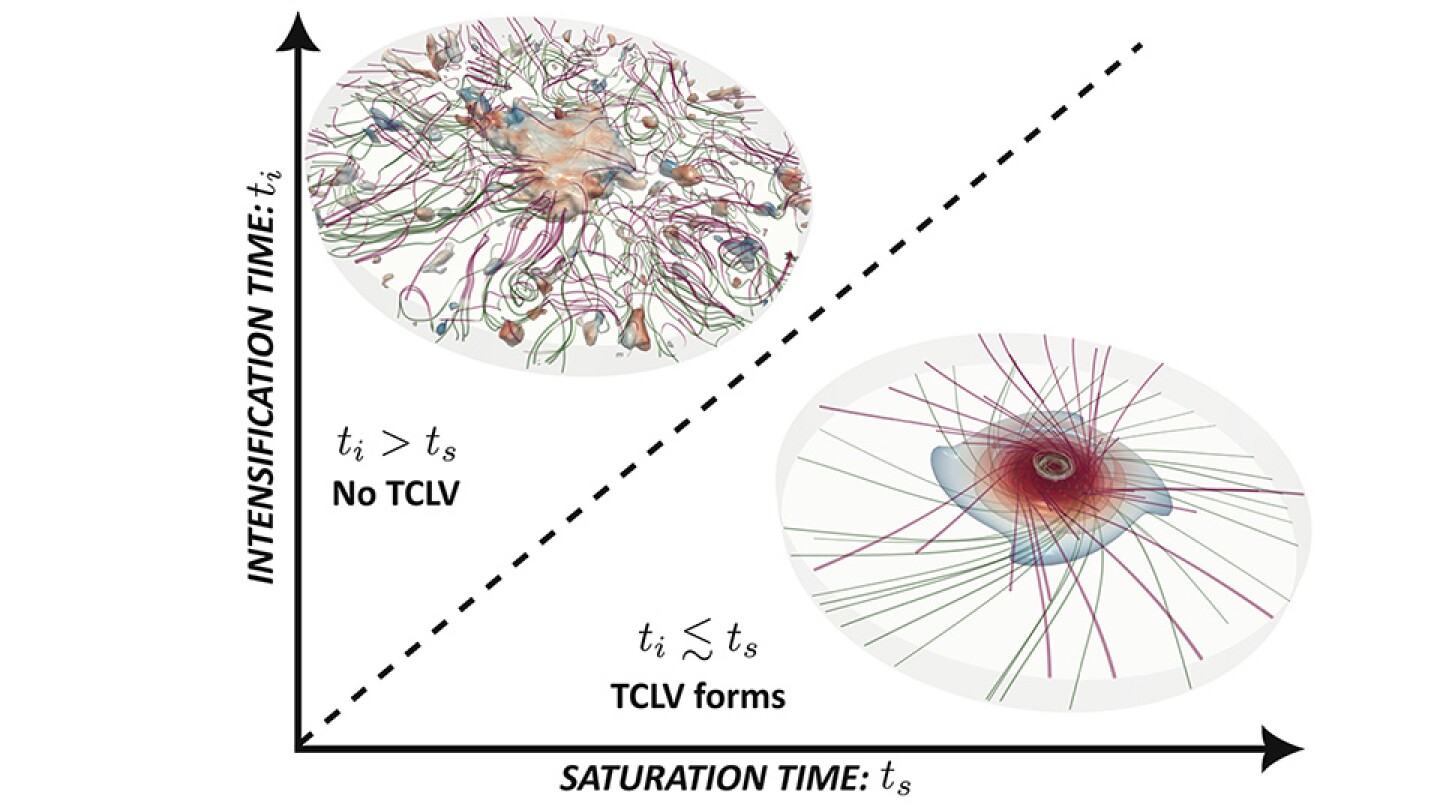
Large-eddy simulations provide a new view into how to produce and study vortices with a central eye and eye wall inside a confined volume.

Teen-driven brand Windsor skipped the models and went straight to the influencers for this year’s prom campaign.
“Prom House” brought together six influencers, including the Clements Twins and TikTokker Faith Marie, to style unique prom…
Methane is a powerful greenhouse gas that is second only to carbon dioxide in driving up global temperatures. But it doesn’t linger in the atmosphere for long thanks to molecules called hydroxyl radicals, which are…
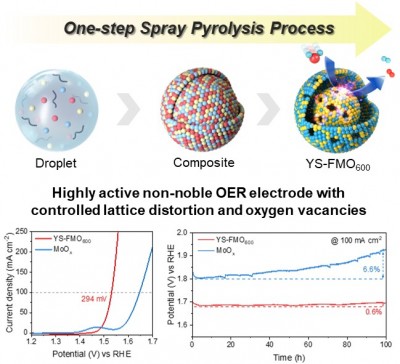
# A novel catalyst design enables simultaneous control of lattice structure and oxygen vacancies in molybdenum oxide through iron (Fe) substitution, with the study selected as a cover article in a leading international…

Stay Connected: Supplying the Globe, JC Contemporary, 10 Hollywood Rd, Central, Hong Kong, until 31 May 2026
The past can be a foreign country, as the saying goes, and for China even recent history can seem stunningly distant. With its two-part…
This week, from 25–28 March 2026, the European AIDS Treatment Group (EATG), together with Ribbon – A Center of Excellence (USA), The Reunion Project (USA), and Realize (Canada), is bringing together a powerful global community in Sitges,…

Our live coverage of conflict in the Middle East continues, as US and Iranian officials give conflicting accounts of talks between…