ANI |
Updated: Nov 13, 2025 09:25 IST
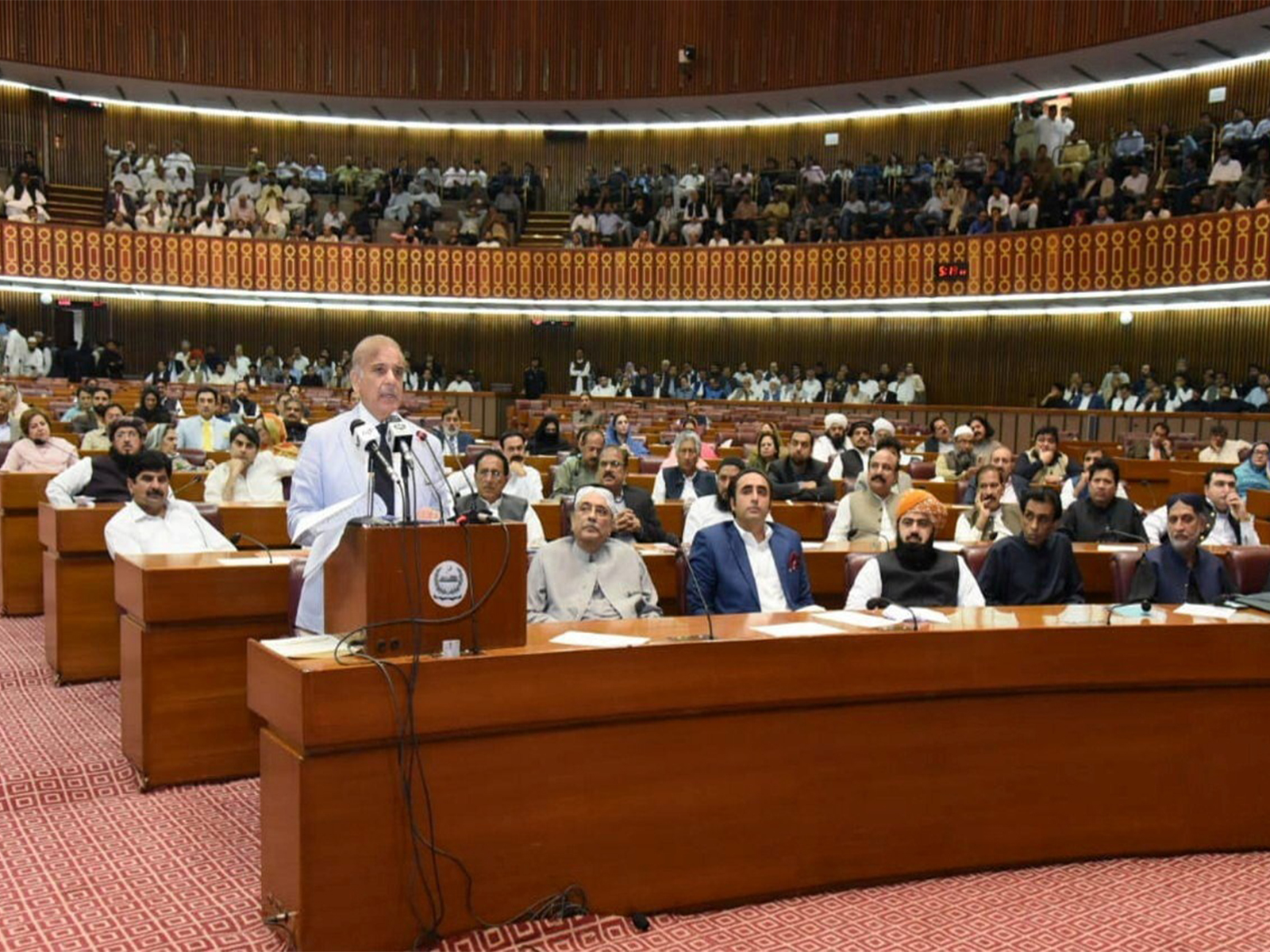
Islamabad [
This request seems a bit unusual, so we need to confirm that you’re human. Please press and hold the button until it turns completely green. Thank you for your cooperation!
BEIRUT, Nov. 12 (Xinhua) — The United Nations Interim Force in Lebanon (UNIFIL) began restoring and reinstalling blue boundary markers along the Blue Line…
Google has decided to loosen some of its recently introduced rules regarding registration of Android developers and their apps, but isn’t rushing to deliver the modest changes it plans.
The company has long required developers of apps sold in…

This post was originally published on NCSOFT.com and is republished here with permission.
NCSOFT Kicks Off G-Star 2025 with Surprise Announcement and Trailer Showcasing Horizon’s Signature Hunting Action and Advanced Combat…

The US House of Representatives voted to pass the funding bill to end the longest government shutdown in US history. Trump signed the bill into law on Wednesday night.
The legislation comes in the wake of a Senate-brokered compromise in which a…

With the government reopened, some federal employees and contractors are expected to return to work as soon as Thursday morning. However, the full impact of the…