Medical Express Severe COVID-19 and influenza infections prime the lungs for cancer and can accelerate the disease’s development, but vaccination heads off those harmful effects, new research…
Author: admin
-

The U.S. and allies announce plans to tap emergency oil reserves; missile strikes continue throughout the Middle East
The United States and its allies announced steps to ease rising oil prices on Wednesday as the war with Iran continued to create chaos in the global oil market amid ongoing missile attacks throughout the Middle East.
Three ships were struck near…
Continue Reading
-

The Strait Is Closed, the Story Keeps Changing, and You’re Paying for It All
There’s a particular kind of dread that sets in when you’re watching an official tweet get deleted in real time.
On Tuesday, the Energy Secretary posted that the U.S. Navy had successfully escorted an oil tanker through the Strait of…
Continue Reading
-

Why did U.S. bombings cause ‘acid rain’ to fall in Iran? An atmospheric scientist explains
This article originally appeared on The Conversation.
Reports are emerging of black rain falling over parts of Iran in the hours after U.S.-Israeli airstrikes on oil depots on the weekend, with some outlets describing it as “
Continue Reading
-
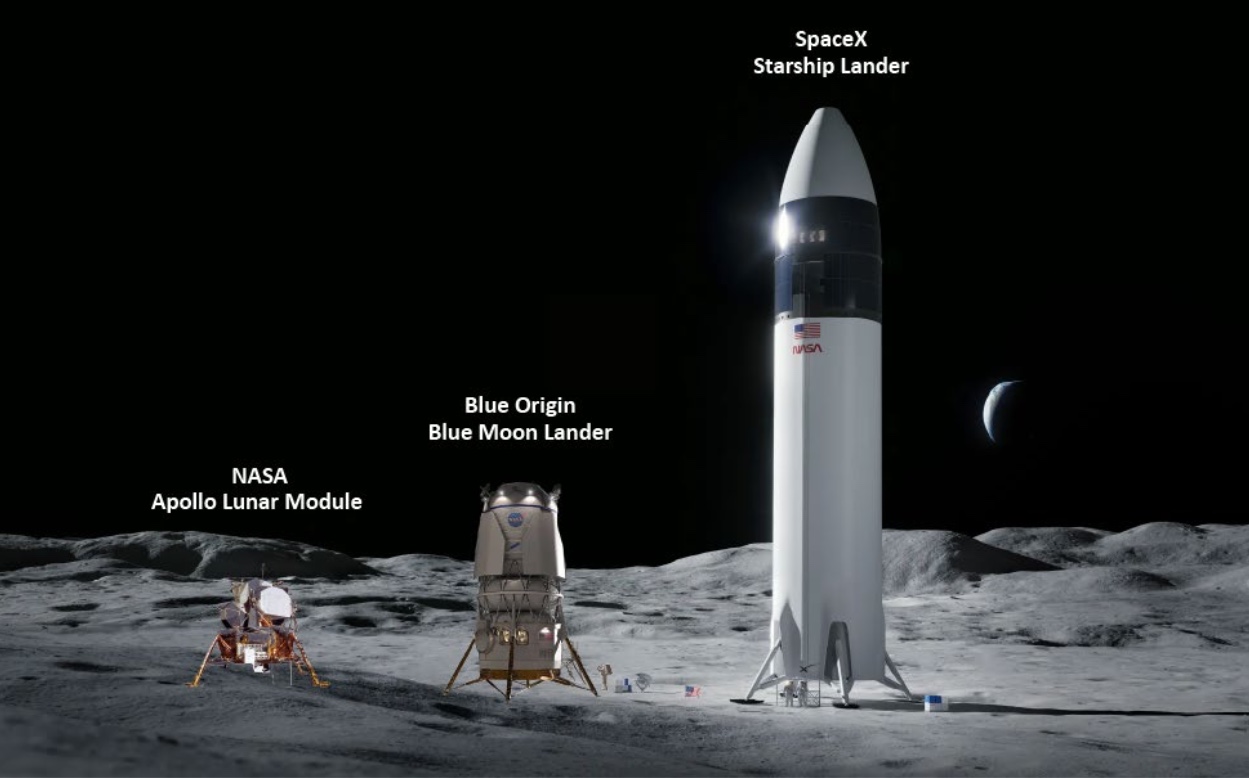
Report criticizes delays in Artemis lunar lander development
WASHINGTON — NASA’s approach to managing the development of crewed lunar landers for Artemis has successfully controlled costs but not schedule, raising questions about NASA’s desire to accelerate those efforts.
NASA’s Office…
Continue Reading
-

Scientists Can Finally Explain Rare Blood Clots Linked to COVID Vaccines | The Transmission
Science Alert COVID vaccines saved millions of lives, but months into the rollout, a small number of people began developing dangerous blood clots in unusual parts of the body.
These only happened after vaccines that used a modified…
Continue Reading
-

Angelina Jolie’s kids support mother after she makes ‘inevitable’ future decision
Angelina Jolie is seemingly planning a major future move….
Continue Reading
-

Conan O’Brien says addressing politics at Oscars is a ‘dance’
The big question surrounding last year’s Academy Awards was whether the show would address the L.A. wildfires, which had rattled the city mere months prior.
This year, the elephant in the room is the ongoing Iran war, which like last year’s…
Continue Reading
-

Galaxy Buds4 Series Elevates Call Clarity with HD Voice – Samsung Newsroom Canada
HD voice cuts background noise and captures every word
At the recent Galaxy Unpacked event, Samsung Electronics introduced the most advanced Galaxy Buds to date. Galaxy Buds4 Series sound as good…
Continue Reading
