Add your e-mail address to receive free newsletters from SCIRP.
Zheng, R. et al. Cancer incidence and mortality in China, 2016. J. Natl. Cancer Center 2(1), 1–9 (2022).
Dag, A. Z., Akcam, Z., Kibis, E., Simsek, S. & Delen, D. A probabilistic data…

The green loan will be used to finance the development, construction and operation of a multibuilding data center. The financing has also been structured to comply with green loan principles, with proceeds to be applied towards the development satisfying key eligibility criteria.
The financing is bespoke with structural features customary for large scale project financings in the data center sector. This transaction represents continued growth of the digital infrastructure sector in Thailand.
The Baker McKenzie team was led by Viroj Piyawattanametha (Head of Energy & Infrastructure, Bangkok) and Tatcha Thumpramoth (Partner, Energy & Infrastructure, Bangkok), with key contributions from Hongrat Jungwanitchakun, Roypim Ransigutta and Panisa Daochai.

Imagine a song about the noisy centre of Amsterdam turning magically into chocolate, prompting children to go wild and eat it. The edifice then melts away, once you get the train from Amsterdam Lelylaan to Haarlemmermeer. This is the story of…
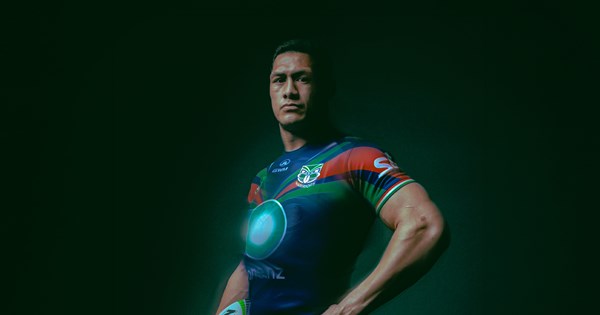
Winger Alofi’ana Khan-Pereira and second rower Marata Niukore are the two players omitted from the One New Zealand Warriors’ extended squad 24 hours out from Friday night’s round two NRL clash against Canberra at Go Media Stadium (8.00pm…

The Pakistan Airports Authority (PAA) has introduced a new facility to enhance passenger services at Islamabad International Airport with the launch of a currency exchange counter in the international arrivals lounge.
The facility was formally…

On International Women’s Day 2026, Niko Partners, as a certified woman-owned business, would like to commemorate how women shift industries, cultures, and economies. In this article, we will explore Asia’s women-oriented games market to…

The night before hosting her traditional power-hour for the female nominees of the Academy Awards, Diane von Furstenberg had a brain wave: these need-to-know stars needed stars. A quick trip to the craft store saved the day. “Next year, we’ll…

Kate Winslet is reportedly in talks to join the cast of ‘Lord of the Rings: Hunt for Gollum’, directed by Andy Serkis. The film will expand on the Middle-earth universe, with Peter Jackson producing.
LONDON: Academy Award-winning actress Kate…