- Fitch Rates Borouge Group International ‘A-(EXP)’; Outlook Stable Fitch Ratings
- OMV agreed with ADNOC on delay of BGI listing, exchange offer and capital increase TradingView
- ADNOC and OMV are set to complete chemicals mega-merger by end of March marketscreener.com
- ADNOC, OMV Advance Formation Of Borouge Group International AG UrduPoint
- UAE’s Adnoc, OMV advance formation of Borouge Group International AG – statement marketscreener.com
Author: admin
-
Fitch Rates Borouge Group International 'A-(EXP)'; Outlook Stable – Fitch Ratings
-
H5N1 in marine mammals is spreading: Research tallies over 50,000 seals and sea lions killed along South America's coast – Phys.org
- H5N1 in marine mammals is spreading: Research tallies over 50,000 seals and sea lions killed along South America’s coast Phys.org
- More animals die from H5N1 avian flu at Ano Nuevo State Park in California CIDRAP
- Deadly virus detected in new Bay…
Continue Reading
-
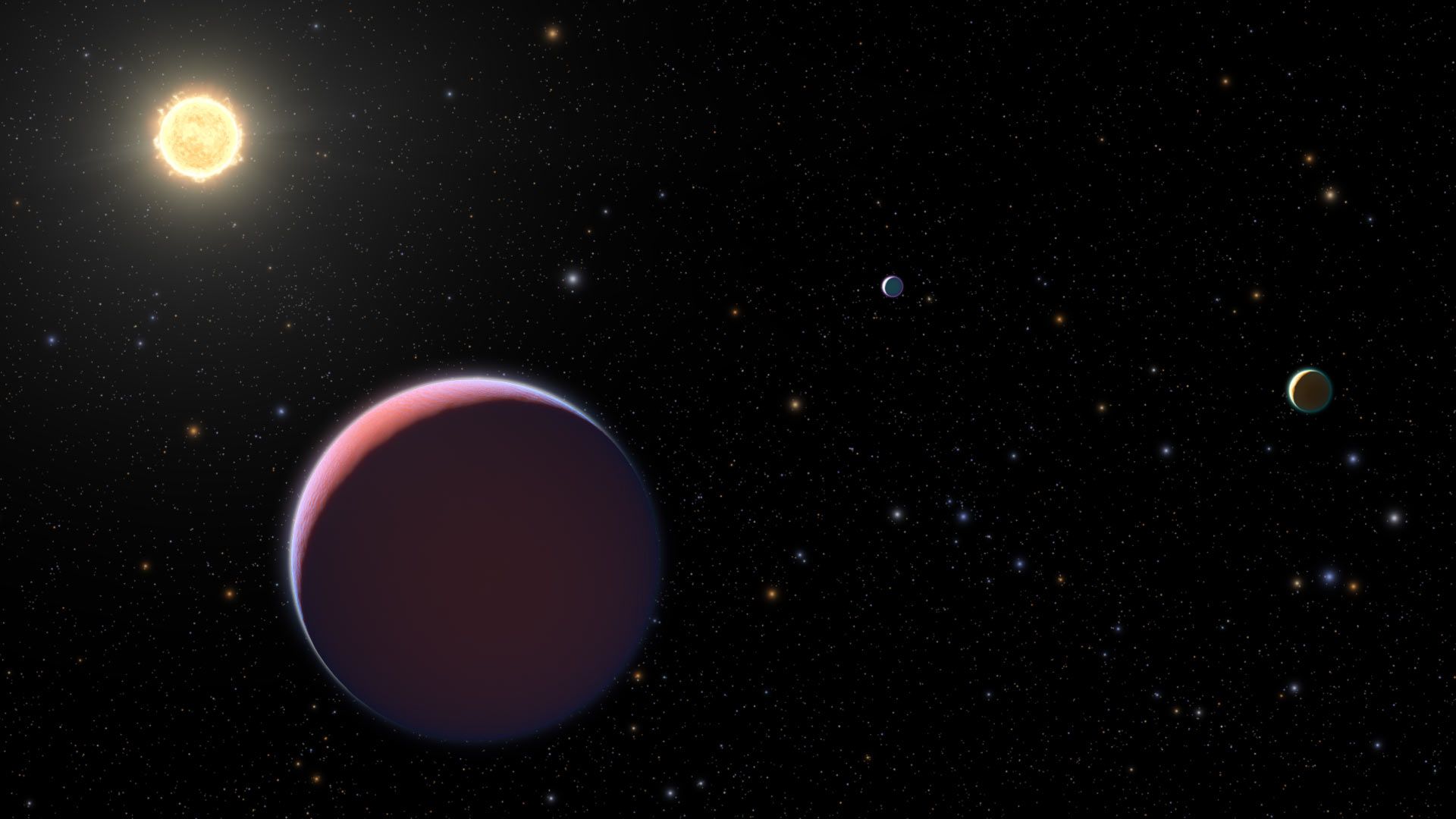
These cotton candy exoplanets hide behind a haze even the James Webb Space Telescope can’t penetrate
An exoplanet so light that it would float on water, were there an ocean large enough, is continuing to frustrate astronomers by concealing its closest secrets with a layer of haze thicker than any ever seen on a planet before.
The haze is so…
Continue Reading
-
Computational Model Predicts Telomere Length from Images of Routine Histopathology Slides – Genetic Engineering and Biotechnology News
- Computational Model Predicts Telomere Length from Images of Routine Histopathology Slides Genetic Engineering and Biotechnology News
- Computational Model Measures Key Aging Metric From Routine Biopsies | Newswise Newswise
- AI Model Predicts…
Continue Reading
-
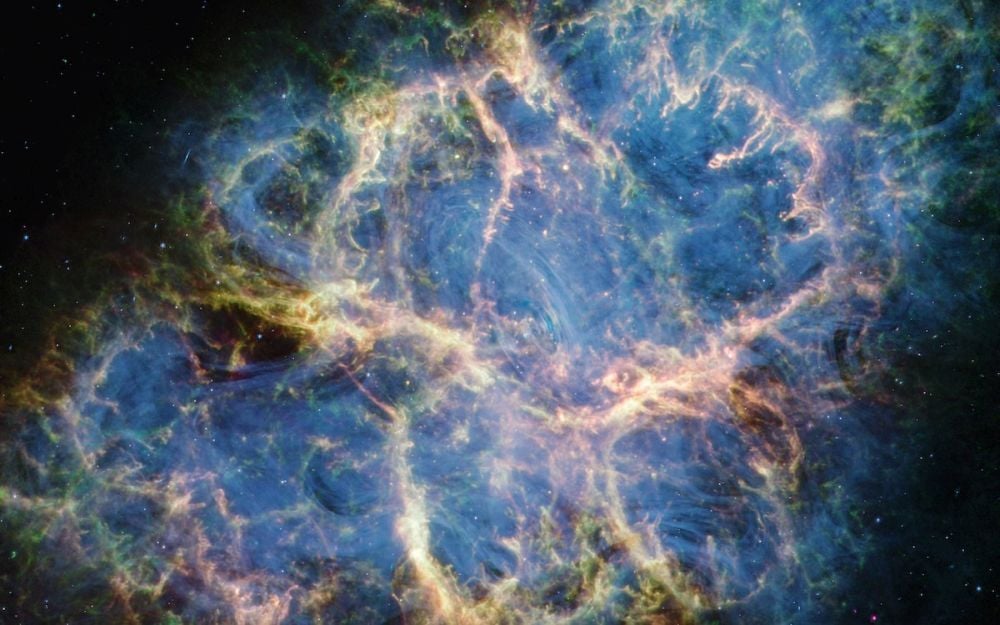
The Crab Pulsar’s Puzzling Emissions Finally Explained.
Most objects that astronomers and astrophysicists study have existed for billions of years. Things like supermassive black holes, the Milky Way galaxy, even the Sun and the Earth predate humanity by billions of years.
But not the Crab…
Continue Reading
-

NASA could send robots and rovers to the moon once a month next year
The NASA administrator said the space agency wants to increase its presence on the moon with robot landers.
While it hasn’t been formally announced, Administrator Jared Isaacman said in an interview on
Continue Reading
-

Scientists record longest ever underwater timelapse. What is reveals is astonishing
There’s something surprisingly soothing about watching fish and other aquatic animals quietly going about their business in another part of the world. That’s probably why projects such as the Fish Doorbell and Beluga Cam have gained such…
Continue Reading
-

Aston Martin’s Adrian Newey to step down as team leader – sources
Adrian Newey is set to step back from his team leadership role at Aston Martin to focus solely on technical matters, sources have confirmed to ESPN.
Newey became managing technical partner and shareholder in Aston Martin’s F1 team in March 2025,
Continue Reading
-

‘Bachelorette’ Canceled by ABC Amid Taylor Frankie Paul Investigation
Season 22 of “The Bachelorette” has been canceled amid a police investigation involving its lead, reality TV star Taylor Frankie Paul.
On March 19, just three days before the reality dating show was set to premiere on ABC, the network’s…
Continue Reading
-

Elaine Welteroth Designs Davis Frames for Look Optic Collaboration
Look Optic has added a new personality to its roster of collaborators.
BirthFund founder, journalist and author Elaine Welteroth has designed a new frame shape called the Davis, which is available via Look Optic’s website…
Continue Reading