Paolo Banchero and the Magic are in Charlotte to take on the Hornets on NBA TV as Dell Curry’s jersey is retired.
Recap the best of Thursday’s slate with the NBA.com live blog, featuring all of the meaningful moments, performances,…

Paolo Banchero and the Magic are in Charlotte to take on the Hornets on NBA TV as Dell Curry’s jersey is retired.
Recap the best of Thursday’s slate with the NBA.com live blog, featuring all of the meaningful moments, performances,…
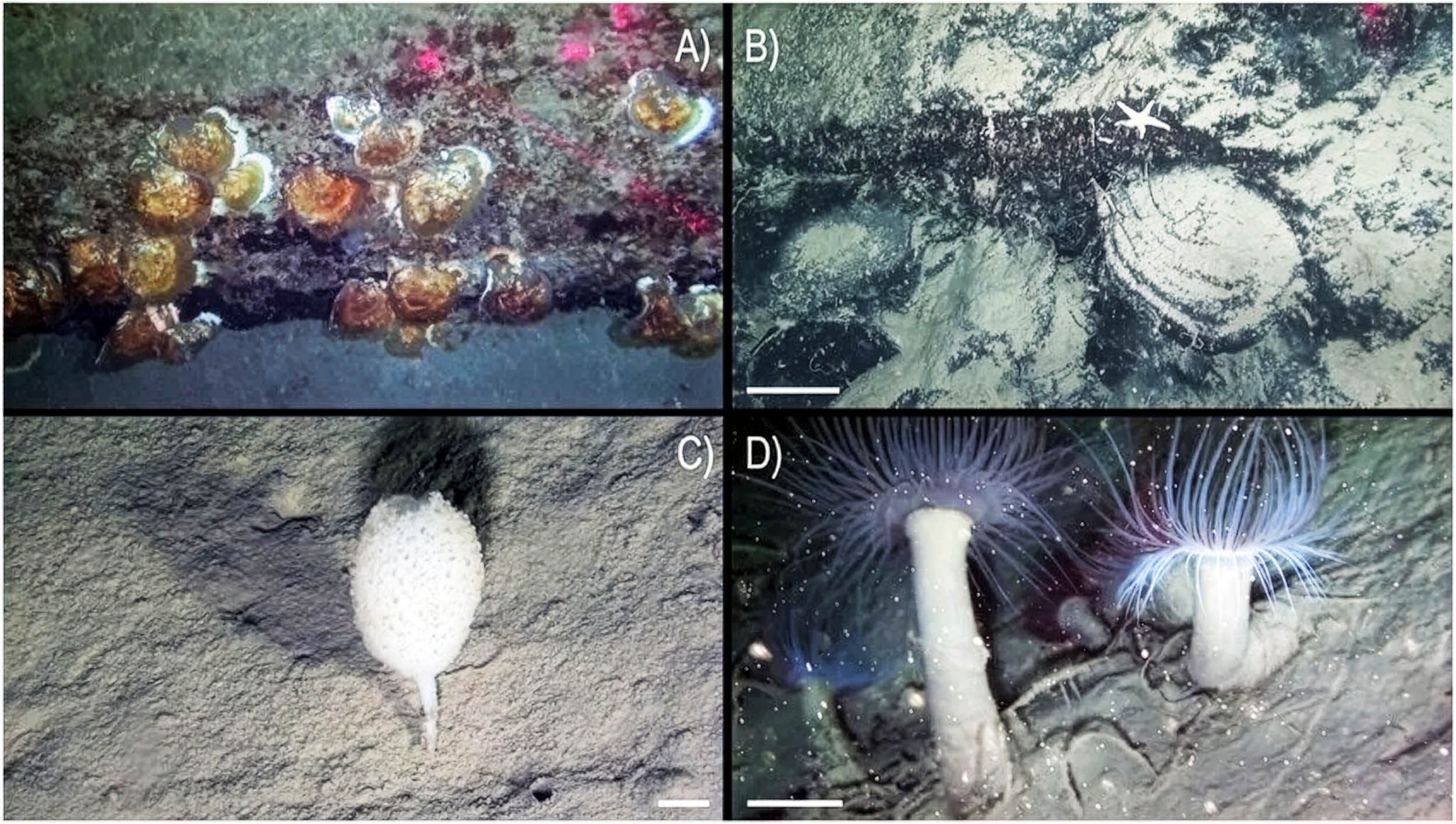
Marine scientists have uncovered a large, ancient coral reef more than 1,640 feet (500 meters) below the Gulf of Naples, off southern Italy.
The finding reveals that one of the Mediterranean’s most familiar coastlines still hides a deep…
For more than a century, dinosaur footprints have been both a gift and a headache. They’re some of the most direct evidence we have of animals moving through real landscapes, but they’re also notoriously hard to interpret.
A footprint is not…

Argentina’s spunkiest duo Ca7riel & Paco Amoroso have checked themselves into a wellness center for their latest album, “Free Spirits.”
Out Thursday, the LP pushes the limits of the duo’s experimentation, combining unpredictable blends…

A highly unusual take on one of Britain’s most iconic small cars is set to appear at auction, as a 1985 Austin Mini converted into a stretch limousine prepares to cross the block later this month.
Originally produced as a compact economy…

Another member of the Duggar family, famous for the TLC series “19 Kids and Counting,” faces allegations of child sex abuse.
Joseph Duggar, the 31-year-old son of Jim Bob and Michelle Duggar and the younger brother of convicted sex offender…

The F-35 fighter jet landed safely and the pilot is in stable condition, CENTCOM spokesman Captain Tim Hawkins said.
An F-35 fighter jet from the United States has made an emergency landing at an airbase in the Middle East after carrying out a…
An exoplanet so light that it would float on water, were there an ocean large enough, is continuing to frustrate astronomers by concealing its closest secrets with a layer of haze thicker than any ever seen on a planet before.
The haze is so…