Scientists at the UNC School of Medicine have made a breakthrough in understanding how cells respond to some of the most widely used medicines at the molecular level.
Their study, published in the journal Proceedings of the National Academy of…

Scientists at the UNC School of Medicine have made a breakthrough in understanding how cells respond to some of the most widely used medicines at the molecular level.
Their study, published in the journal Proceedings of the National Academy of…

United States President Donald Trump has repeatedly threatened that Washington could intervene militarily in Iran if there is a violent crackdown on demonstrators amid ongoing protests.
On Wednesday, it emerged that some personnel have been…
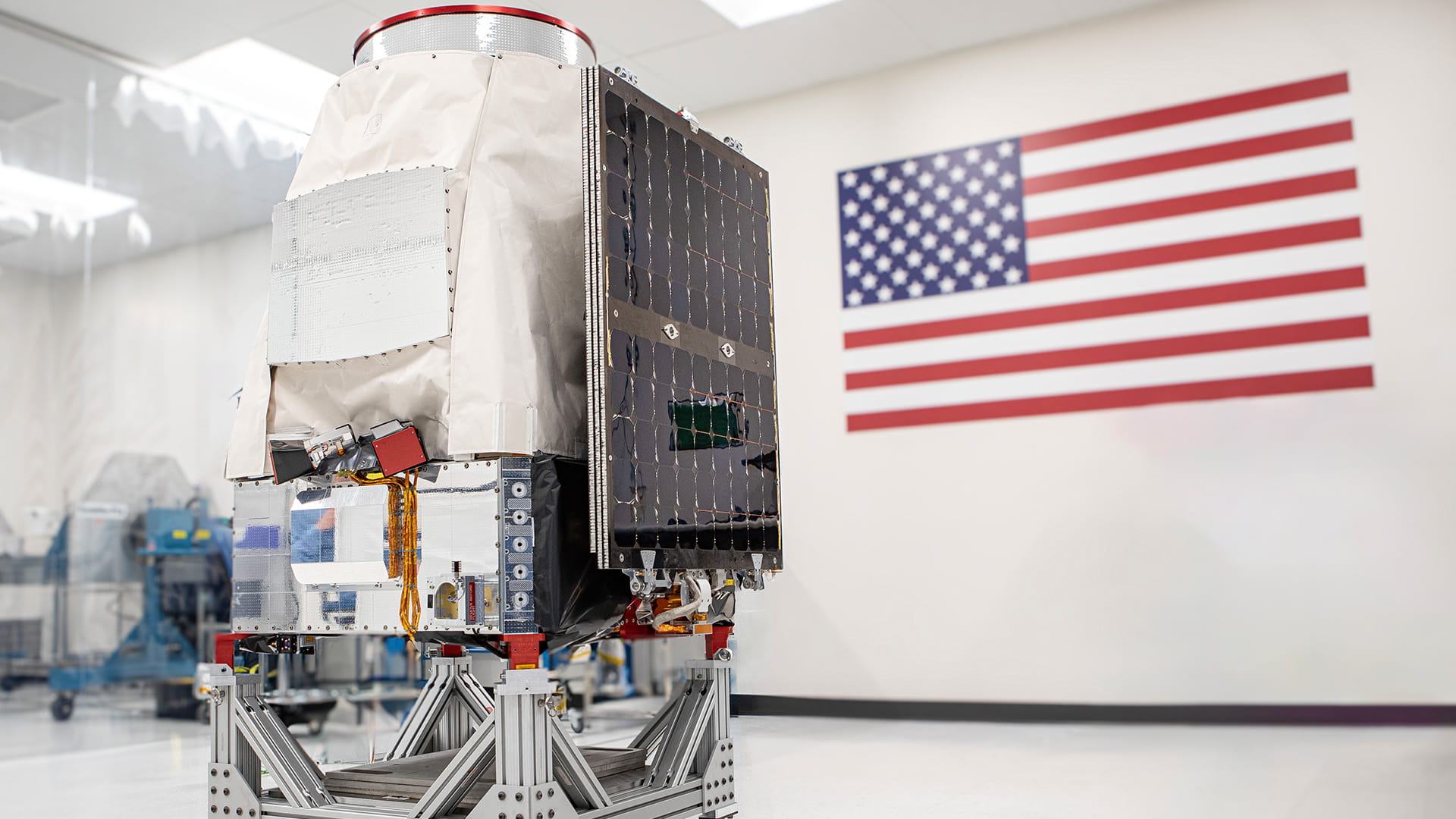
Pandora mission to utilize Saturn-200 minisatellite platform for exoplanet long observations
LAFAYETTE, Colo., Jan. 14, 2026 /PRNewswire/ — A Saturn-200 minisatellite, developed by Blue Canyon Technologies—RTX’s (NYSE: RTX) small satellite…

Apps & Services
Samsung Mobile Gaming Hub introduces personalized discovery and frictionless access, elevating how players enjoy their favorite gaming content on Galaxy devices
1/14/2026

A motorcyclist who died in a crash following a police pursuit is the son of musician and producer Paul Hardcastle, the BBC understands.
Essex Police said officers followed a motorbike on Monday after it failed to stop for them in Ongar High…
URBANA–CHAMPAIGN, Ill.–(BUSINESS WIRE)–Dr. Adil Haider, a globally recognized surgeon-scientist, academic leader, and founder of Boston Health AI, has been appointed as the Inaugural Chief Artificial Intelligence Officer (CAIO) at The…
A fantastic opportunity has opened up for local entrepreneurs to bring refreshments back to one of St Annes’ most popular seafront locations, with Fylde Council inviting expressions of interest for a prime trading spot at North Promenade Car Park.
The prominent site, situated right at the car park entrance next to the beloved Les Dawson memorial and just steps from St Annes Pier, previously hosted a successful ice cream and refreshments vendor that served thousands of visitors each year. Now, the Council is searching for a new operator to breathe life into this vibrant location, enhancing the visitor experience for families, tourists and locals who flock to our beautiful coastline.
The approximately 42 square metre pitch offers tremendous potential for the right business, whether that’s traditional seaside treats, artisan coffee, or other refreshments that complement the promenade’s family-friendly atmosphere. With high footfall throughout the year and particularly during our bustling summer season, this represents a genuine opportunity for a local business to thrive while serving our community.
Councillor Jayne Nixon, Lead Member for Tourism, Leisure and Culture, said: “This is a wonderful chance for someone to establish or expand their business in one of our resort’s prime locations. We’re looking for an operator who shares our vision for creating memorable experiences for visitors while supporting the local economy. The North Promenade is the heart of St Annes’ seafront, and having quality refreshments available here really adds to what makes our coast special.”
The successful operator will receive a fixed-term licence from the Council, with flexible options for year-round or seasonal trading to suit different business models. Applications close at midnight on Monday 23rd February 2026, with decisions expected the following week.
For additional information or to submit an expression of interest, interested parties should find the particulars and register their details here.
Keep up to date with the latest Fylde Council news by following us on social media or subscribing to our newsletter. Any new information will be posted directly through these channels, so if you are following us, you’ll be the first to know.

Islamabad (TDI): Australia has reaffirmed its strong commitment to deepening economic cooperation and maintaining longstanding friendly relations with Pakistan, with a particular focus on mining and other key sectors, during a meeting.
Speaker of…