- PM Shehbaz lauds Pakistan military’s professionalism.
- PM reiterates resolve to…
Author: admin
-
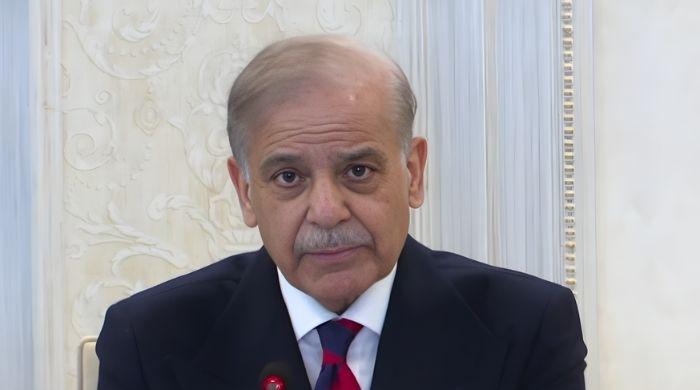
Pakistan in talks with multiple countries over fighter jet sales: PM Shehbaz
Prime Minister Shehbaz Sharif addresses federal cabinet meeting in Islamabad, January 14, 2026. — Screengrab via YouTube/Geo News -

‘Umair 7:11 minutes viral video Pakistan’ running wild after 19-minute viral video; What could be the connection
What makes people inclined to click is the…
Continue Reading
-

Exclusive: US withdrawing some troops from key Middle East bases as precaution, US official says
WASHINGTON, Jan 14 (Reuters) – The United States is withdrawing some personnel from key bases in the region as a precaution given heightened regional tensions, a U.S. official told Reuters on Wednesday, speaking on condition of anonymity.
The…
Continue Reading
-

Radical Museums | S3E4: Nelson Cummins
Radical Museums | S3E4: Nelson Cummins – Museums Association
…Continue Reading
-

Only the Poets to be supported by unsigned act at £1 Brixton gig
A band will give an unsigned group or artist a supporting slot at a legendary London venue when they play a sold-out gig where all tickets cost £1.
Only the Poets, from Reading, Berkshire, and Banbury, Oxfordshire, charged £1 for their first gig…
Continue Reading
-

From a new flagship space telescope to lunar exploration, global cooperation – and competition – will make 2026 an exciting year for space – The Conversation
- From a new flagship space telescope to lunar exploration, global cooperation – and competition – will make 2026 an exciting year for space The Conversation
- What’s on the horizon for space exploration in 2026? MSN
- This Week In Space podcast:…
Continue Reading
-

Could ChatGPT convince you to buy something? Threat of manipulation looms as AI companies gear up to sell ads
Eighteen months ago, it was plausible that artificial intelligence might take a different path than social media. Back then, AI’s development hadn’t consolidated under a small number of big tech firms. Nor had it capitalized on consumer…
Continue Reading
-
‘Some powers’ want Sindh’s rights and resources transferred to Islamabad, alleges Bilawal – Dawn
- ‘Some powers’ want Sindh’s rights and resources transferred to Islamabad, alleges Bilawal Dawn
- Certain forces seek to seize Sindh’s resources under governance pretext: Bilawal Geo News
- Bilawal accuses ‘some forces’ of rolling back…
Continue Reading
-
Pakistan, Bahrain seek deeper trade and security ties as President Zardari receives top award – Arab News
- Pakistan, Bahrain seek deeper trade and security ties as President Zardari receives top award Arab News
- President Zardari meets Bahrain’s king in Manama, discusses defence cooperation, regional and global matters Dawn
- Pakistan committed to…
Continue Reading
-

Immediate answers needed as Iran warship confusion continues
South Africans are entitled to clear answers about the role of foreign warships in Exercise Will for Peace 2026. Instead, what we have seen is confusion, contradiction and secrecy.
Yesterday the SANDF posted that four naval vessels would take…
Continue Reading