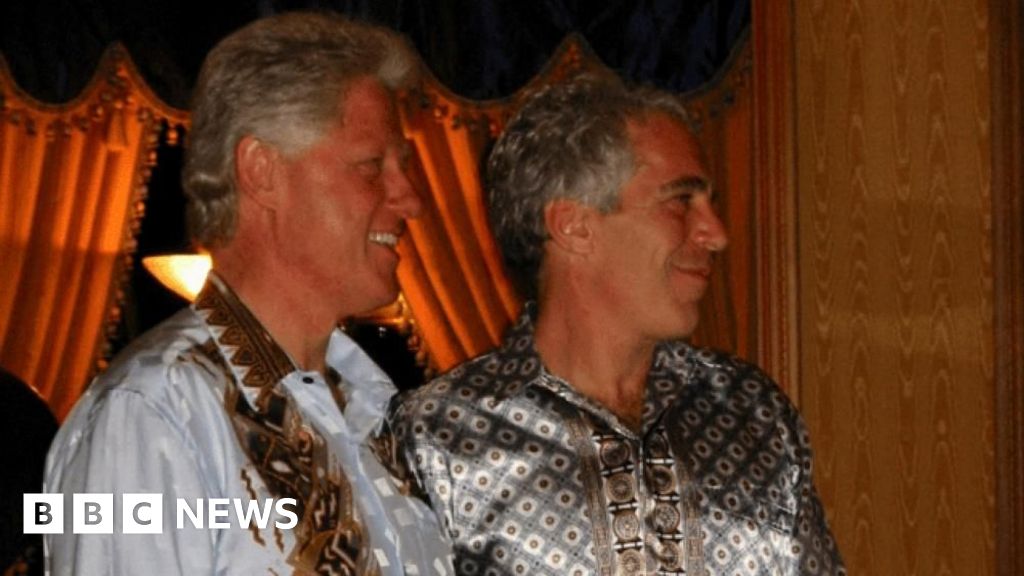
A Republican lawmaker is vowing to begin contempt-of-Congress proceedings against former President Bill Clinton after he failed to show up on Tuesday to testify before a committee investigating Jeffrey Epstein.
House Oversight Committee Chairman…
A Republican lawmaker is vowing to begin contempt-of-Congress proceedings against former President Bill Clinton after he failed to show up on Tuesday to testify before a committee investigating Jeffrey Epstein.
House Oversight Committee Chairman…

SAN ANTONIO – Editor’s note: This story was published through a partnership between KSAT and Live From the Southside, a local and Latina-owned magazine that works to improve & expand community relationships through promoting events, stories…

You may think that the goal of movie studios is to churn out as many sequels as quickly as possible, but there’s so much more strategy that goes into sequel production than what meets the eye.
In the latest episode of The Aha!…

In her tenure at Elmbrook Swim Club and Brookfield East, Wanezek made her mark early. At only 12 years old, she was making waves in her national National Age Group.
The transition from the small community of swimmers at the high school level in…
To safely host the Orlando Magic 5K & Kids’ Run event, the following roads will be closed at the times indicated.
Event Staging:

As waves of protests have tested the Iranian regime’s ability to manage dissent, the country with arguably the most to gain has been waiting in the wings, reluctant to intervene even when its regional…
KANSAS CITY, Mo. – Mid-America Christian (Okla.) junior forward Taliah Lee was voted as NAIA Women’s Basketball Defensive Player of the Week after back-to-back wins that…

Webcasts | January 13, 2026
Join partners from our Consumer Protection and White Collar Defense & Investigations Practice Groups for a recorded webcast on emerging consumer protection enforcement trends. The panel explores the intersection of U.S. Department of Justice and Federal Trade Commission enforcement priorities, the expanding role of State Attorneys General, and key developments at the nexus of consumer protection and data privacy. The discussion highlights what companies should expect in the evolving enforcement landscape and strategies for mitigating risk.
MCLE CREDIT INFORMATION:
This program has been approved for credit in accordance with the requirements of the New York State Continuing Legal Education Board for a maximum of 1.0 credit hour, of which 1.0 credit hour may be applied toward the areas of professional practice requirement. This course is approved for transitional/non-transitional credit.
Gibson, Dunn & Crutcher LLP certifies that this activity has been approved for MCLE credit by the State Bar of California in the amount of 1.0 hour.
Gibson, Dunn & Crutcher LLP is authorized by the Solicitors Regulation Authority to provide in-house CPD training. This program is approved for CPD credit in the amount of 1.0 hour. Regulated by the Solicitors Regulation Authority (Number 324652).
Neither the Connecticut Judicial Branch nor the Commission on Minimum Continuing Legal Education approve or accredit CLE providers or activities. It is the opinion of this provider that this activity qualifies for up to 1.0 hour toward your annual CLE requirement in Connecticut, including 0 hour(s) of ethics/professionalism.
Application for approval is pending with the Colorado, Illinois, Texas, Virginia, and Washington State Bars.
PANELISTS:
Gustav Eyler is a partner in Gibson Dunn’s Washington, D.C. office and Co-Chair of the firm’s FDA & Health Care and Consumer Protection Practice Groups. Leveraging years of experience as Director of the U.S. DOJ Consumer Protection Branch — where he led enforcement actions involving drugs, medical devices, food, deceptive marketing, and public health statutes — he defends clients in government investigations and counsels on the design and implementation of compliance programs.
Amanda M. Aycock is a partner in Gibson Dunn’s New York office who represents multinational companies and senior executives in complex litigation, regulatory investigations, and crisis matters. Her cross-disciplinary practice spans consumer protection, data privacy and cybersecurity, white-collar defense, and enforcement actions brought by state attorneys general and federal regulators, including high-stakes consumer and regulatory investigations.
Ryan T. Bergsieker is a partner in Gibson Dunn’s Denver office and a former federal cybercrimes prosecutor whose practice focuses on government investigations, complex civil litigation, and cybersecurity and data privacy counseling. He represents clients in high-stakes enforcement matters with the Department of Justice, Federal Trade Commission, Consumer Financial Protection Bureau, and state attorneys general, with deep expertise in federal, state, and international consumer protection, privacy, and cybersecurity laws.
Debra Wong Yang is a partner in Gibson Dunn’s Los Angeles office and Chair of the firm’s Crisis Management Practice Group. Debra has a strong background in addressing and resolving problems across the white collar litigation spectrum, including through corporate and individual representations, internal investigations, crisis management and compliance. She previously served as the U.S. Attorney for the Central District of California, where she led significant criminal prosecutions and enforcement initiatives.
© 2026 Gibson, Dunn & Crutcher LLP. All rights reserved. For contact and other information, please visit us at www.gibsondunn.com.
Attorney Advertising: These materials were prepared for general informational purposes only based on information available at the time of publication and are not intended as, do not constitute, and should not be relied upon as, legal advice or a legal opinion on any specific facts or circumstances. Gibson Dunn (and its affiliates, attorneys, and employees) shall not have any liability in connection with any use of these materials. The sharing of these materials does not establish an attorney-client relationship with the recipient and should not be relied upon as an alternative for advice from qualified counsel. Please note that facts and circumstances may vary, and prior results do not guarantee a similar outcome.