Tue 13/1/2026
Minister News
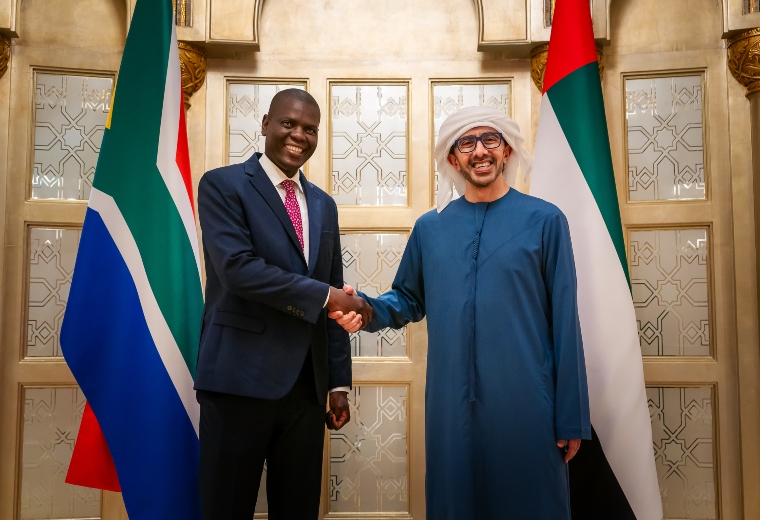
Abdullah bin Zayed, South African Minister of International Relations & Cooperation discuss enhancing ties
H.H. Sheikh Abdullah bin Zayed Al…

Tue 13/1/2026
Minister News
H.H. Sheikh Abdullah bin Zayed Al…
WASHINGTON, D.C. – Congressman Gus Bilirakis (FL-12), Chairman of the Subcommittee on Commerce, Manufacturing, and Trade, delivered the following opening statement at today’s hearing titled Examining Legislative Options to Strengthen Motor Vehicle Safety, Ensure Consumer Choice and Affordability, and Cement U.S. Automotive Leadership.
Subcommittee Chairman Bilirakis’s opening statement as prepared for delivery:
“Good afternoon, everyone, and welcome. Today we will be examining legislation aimed at modernizing motor vehicle safety. Thank you to our witnesses for joining us.
“Whether it is protecting our kids online or ensuring the safety of the cars in our driveways, we have always understood that there is no partisan way to save lives. In 2024, nearly 40,000 people died on our roadways.
“We often talk about these numbers as statistics, but every single one of them represents an empty chair at a dinner table. We cannot accept this as the cost of doing business.
“That is why we must focus on solutions to strengthen motor vehicle safety and empower NHTSA to succeed in its mission to save lives. I would like to highlight several solutions to bolster motor vehicle safety and enable innovation.
“First, we are considering a bipartisan discussion draft of the SELF-DRIVE Act, which establishes a federal framework for the safety deployment of autonomous vehicles. I want to commend Mr. Latta and Ms. Dingell for their hard work over many years to produce this discussion draft.
“AVs are not just a luxury; they can be a lifeline. By reducing human error, which causes the vast majority of crashes, we can prevent tragedies before they happen. AVs can also empower seniors and people with disabilities to be mobile and regain their independence.
“This legislation is also necessary to successfully compete against communist China, who are seeking to flood the world with Chinese self-driving technology. We cannot let America fall behind.
“Second, we are considering the Motor Vehicle Modernization Act, which makes substantial reforms to NHTSA to improve the agency’s operations, ensure the agency is accountable to Congress, and empower the agency to better advance automotive safety and innovation.
“These include reforms to NHTSA’s New Car Assessment Program, which provides market incentives for automakers to compete on safety.
“The bill ensures accountability to providing Congress and stakeholders a defined roadmap of the agency’s research and rulemaking priorities. The bill also revamps NHTSA’s general exemption process to allow for the deployment novel vehicle technologies so America can lead in safety and innovation.
“Finally, as we consider proposals to ensure motor vehicle safety, we must keep in the mind the high costs of motor vehicles, which reached a record high of $50,000 for an average new vehicle. If consumers cannot afford new vehicles, they will not be able to take advantage of the innovative safety features in these vehicles, which will have adverse impacts on highway safety.
“I am confident that, working together, we can advance legislation that prioritizes safety and American automotive leadership. I look forward to hearing from our witnesses on how we can achieve that dream together.”
###
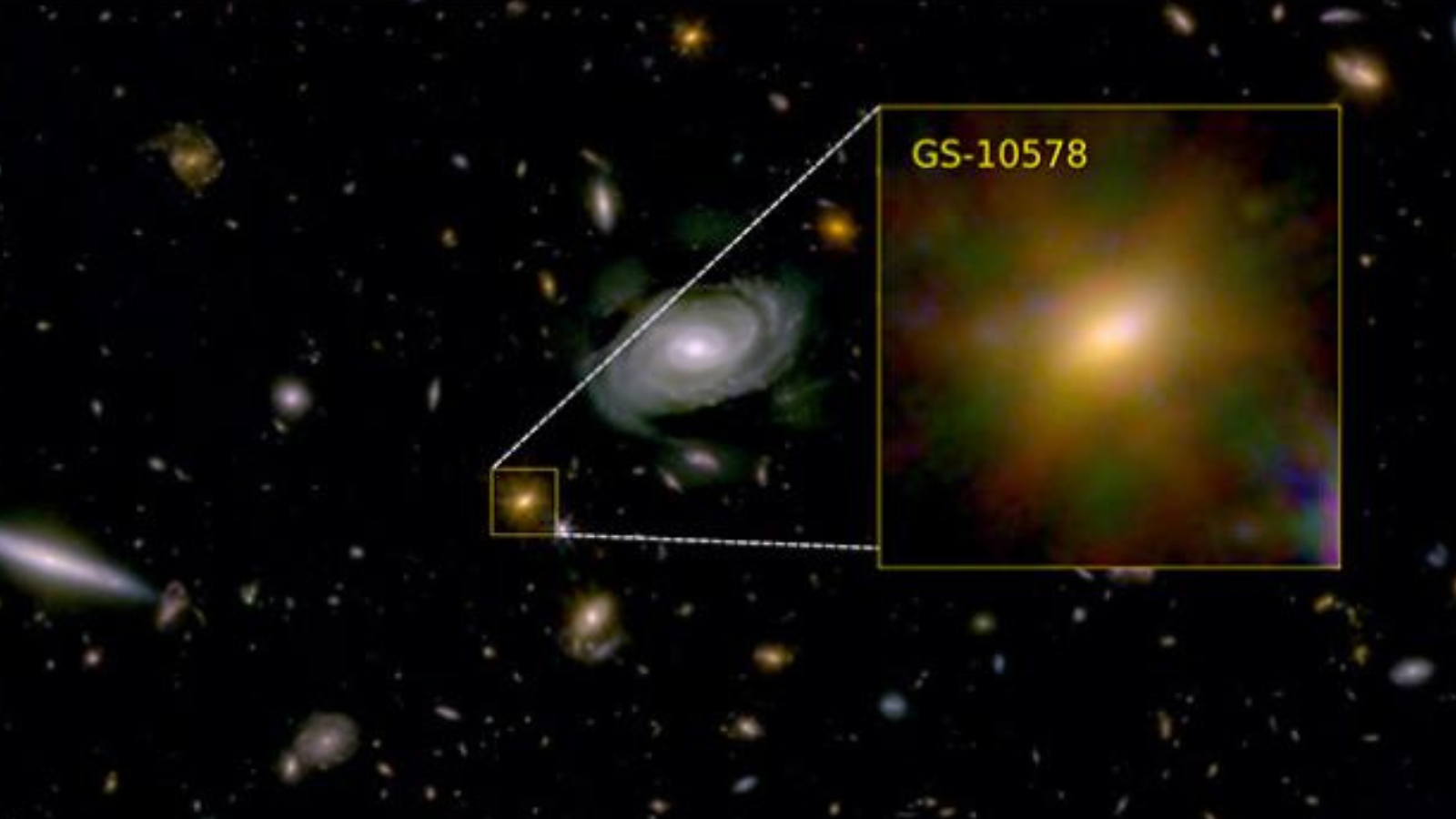
Astronomers have discovered that a young galaxy was gradually starved by its central supermassive black hole, in what was effectively a cosmic “death by a thousand cuts.”
The James Webb Space Telescope (JWST) and the Atacama Large…

Join us for a public webinar on Social Health and Digital Play: A Conversation, Not a Conclusion where we aim to share insights from WHO’s work on social connection; reflect on the current state of the evidence on how video gameplay may…

Laurie Leshin, once a young Tempe girl enamored with space who went on to become a world-class space scientist, is back home. She joined Arizona State University on Jan. 1 as the University Professor for Space Futures.
Leshin was…

Excerpted from “A Long Game” by Elizabeth McCracken, Radcliffe fellow ’08
Once at an excellent weekend writers’ conference, I gave a craft talk. It was called “On Failure” and at least partly concerned why I refused to participate…
Tue 13/1/2026
Minister News
H.H. Sheikh Abdullah bin Zayed Al Nahyan, Deputy Prime…

